


 Sign Out
Sign Out


Pharmacology: Pharmacodynamics: Mechanism of Action: Rocuronium (Repose) is a fast onset, intermediate acting non-depolarizing neuromuscular blocking agent, possessing all of the characteristic pharmacological actions of this class of drugs (curariform). It acts by competing for nicotinic cholinoceptors at the motor end-plate. This action is antagonized by acetylcholinesterase inhibitors such as neostigmine, edrophonium and pyridostigmine.
Pharmacodynamic effects: The ED90 (dose required to produce 90% depression of the twitch response of the thumb to stimulation of the ulnar nerve) during intravenous anesthesia is approximately 0.3 mg/kg rocuronium bromide. The ED95 in infants is lower than in adults and children (0.25, 0.35 and 0.40 mg/kg respectively).
The clinical duration (the duration until spontaneous recovery to 25% of control twitch height) with 0.6 mg/kg rocuronium bromide is 30-40 minutes. The total duration (time until spontaneous recovery to 90% of control twitch height) is 50 minutes. The mean time of spontaneous recovery of twitch response from 25 to 75% (recovery index) after a bolus dose of 0.6 mg/kg rocuronium bromide is 14 minutes. With lower dosages of 0.3-0.45 mg/kg rocuronium bromide (1-1½ x ED90), onset of action is slower and duration of action is shorter. With high doses of 2 mg/kg, clinical duration is 110 minutes.
Intubation during routine anesthesia: Within 60 seconds following intravenous administration of a dose of 0.6 mg/kg rocuronium bromide (2 x ED90 under intravenous anesthesia), adequate intubation conditions can be achieved in nearly all patients of which in 80% intubation conditions are rated excellent. General muscle paralysis adequate for any type of procedure is established within 2 minutes. After administration of 0.45 mg/kg rocuronium bromide, acceptable intubation conditions are present after 90 seconds.
Rapid Sequence Induction: During rapid sequence induction of anesthesia under propofol or fentanyl/thiopental anesthesia, adequate intubation conditions are achieved within 60 seconds in 93% and 96% of the patients respectively, following a dose of 1.0 mg/kg rocuronium bromide. Of these, 70% are rated excellent. The clinical duration with this dose approaches 1 hour, at which time the neuromuscular block can be safely reversed. Following a dose of 0.6 mg/kg rocuronium bromide, adequate intubation conditions are achieved within 60 seconds in 81% and 75% of the patients during a rapid sequence induction technique with propofol or fentanyl/thiopental, respectively.
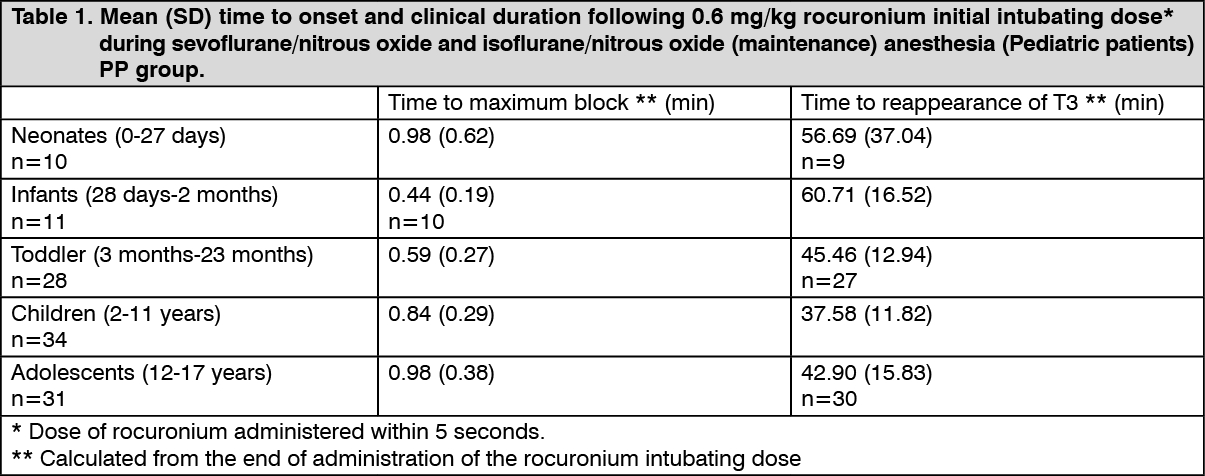
Pediatric population: Mean onset time in infants, toddlers and children at an intubation dose of 0.6 mg/kg is slightly shorter than in adults. Comparison within pediatric age groups showed that the mean onset time in neonates and adolescents (1.0 min.) is slightly longer than in infants, toddlers and children (0.4, 0.6 and 0.8 min., respectively). The duration of relaxation and the time to recovery tend to be shorter in children compared to infants and adults. Comparing within pediatric age groups demonstrated that mean time to reappearance of T3 was prolonged in neonates and infants (56.7 and 60.7 min., respectively) when compared to toddlers, children and adolescents (45.4, 37.6 and 42.9 min., respectively). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageGeriatric patients and patients with hepatic and/or biliary tract disease and/or renal failure: The duration of action of maintenance doses of 0.15 mg/kg rocuronium bromide might be somewhat longer under enflurane and isoflurane anesthesia in geriatric patients and in patients with hepatic and/or renal disease (approximately 20 minutes) than in patients without impairment of excretory organ functions under intravenous anesthesia (approximately 13 minutes) (see Dosage & Administration). No accumulation of effect (progressive increase in duration of action) with repetitive maintenance dosing at the recommended level has been observed.
Intensive Care Unit: Following continuous infusion in the Intensive Care Unit, the time to recovery of the train of four ratio to 0.7 depends on the level of block at the end of the infusion. After a continuous infusion for 20 hours or more the median (range) time between return of T2 to train of four stimulation and recovery of the train of four ratio to 0.7 approximates 1.5 (1-5) hours in patients without multiple organ failure and 4 (1-25) hours in patients with multiple organ failure.
Cardiovascular surgery: In patients scheduled for cardiovascular surgery the most common cardiovascular changes during the onset of maximum block following 0.6-0.9 mg/kg rocuronium bromide are a slight and clinically insignificant increase in heart rate up to 9% and an increase in mean arterial blood pressure up to 16% from the control values.
Reversal of muscle relaxation: Administration of acetylcholinesterase inhibitors, (neostigmine, pyridostigmine or edrophonium) at reappearance of T2 or at the first signs of clinical recovery, antagonizes the action of Rocuronium (Repose).
Pharmacokinetics: After intravenous administration of a single bolus dose of rocuronium bromide the plasma concentration time course runs in three exponential phases. In normal adults, the mean (95% CI) elimination half-life is 73 (66-80) minutes, the (apparent) volume of distribution at steady state conditions is 203 (193-214) mL/kg and plasma clearance is 3.7 (3.5-3.9) mL/kg/min.
Rocuronium is excreted in urine and bile. Excretion in urine approaches 40% within 12-24 hours. After injection of a radiolabeled dose of rocuronium bromide, excretion of the radiolabel is on average 47% in urine and 43% in feces after 9 days. Approximately 50% is recovered as the parent compound. No metabolites are detected in plasma.
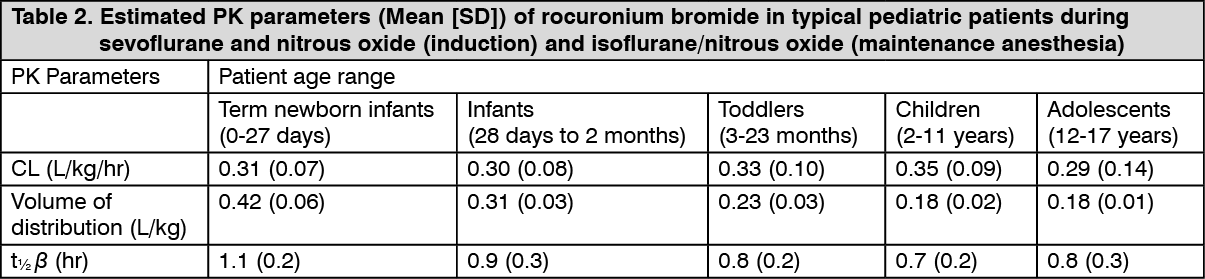
Pediatric population: Pharmacokinetics of rocuronium bromide in pediatric patients (n=146) with ages ranging from 0 to 17 years were evaluated using a population analysis of the pooled pharmacokinetic datasets from two clinical trials under sevoflurane (induction) and isoflurane/nitrous oxide (maintenance) anesthesia. All pharmacokinetic parameters were found to be linearly proportional to body weight illustrated by a similar clearance (l.hr-1.kg-1). The volume of distribution (l.kg-1) and elimination half-life (h) decrease with age (years). The pharmacokinetic parameters of typical pediatrics within each age group are summarized as follows: See Table 2.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageGeriatric patients and patients with hepatic and/or biliary tract disease and/or renal failure: In controlled studies the plasma clearance in geriatric patients and in patients with renal dysfunction was reduced, in most studies however without reaching the level of statistical significance. In patients with hepatic disease, the mean elimination half-life is prolonged by 30 minutes and the mean plasma clearance is reduced by 1 mL/kg/min. (See Dosage & Administration).
Intensive Care unit: When administered as a continuous infusion to facilitate mechanical ventilation for 20 hours or more, the mean elimination half-life and the mean (apparent) volume of distribution at steady state are increased. A large between patient variability is found in controlled clinical studies, related to nature and extent of (multiple) organ failure and individual patient characteristics. In patients with multiple organ failure a mean (± SD) elimination half-life of 21.5 (± 3.3) hours, a (apparent) volume of distribution at steady state of 1.5 (± 0.8) l/kg and a plasma clearance of 2.1 (± 0.8) mL/kg/min were found. (See Dosage & Administration).