Frequency Estimates: Frequent: >10%, occasional: 1-10%, rare: 0.001-1%, isolated cases: <0.001%.
Rifampicin: Rifampicin may cause reddish discoloration of body fluids and occasionally other body secretions eg, urine, sputum, lacrimal fluid, feces, saliva, sweat. It may permanently discolor soft contact lenses.
Unwanted Effects which may Occur During Continuous Daily or Intermittent Therapy: Skin and Appendages: Occasional: Flushing, itching with or without skin rash, urticaria and reddening of the eyes. Isolated Cases: Severe signs and symptoms eg, exudative conjunctivitis or generalized hypersensitivity reactions involving the skin (eg, exfoliative dermatitis, Lyell's syndrome) and pemphigoid reactions.
Gastrointestinal Tract: Occasional: Anorexia, nausea, abdominal pains, gaseous distention. Rarely: Vomiting or diarrhea. Isolated Cases: Erosive gastritis and pseudomembranous colitis.
Liver: Frequently, an asymptomatic increase in liver enzymes. Rarely: Hepatitis or jaundice. Isolated Cases: Induction of porphyria.
Central and Peripheral Nervous System: Occasional: Tiredness, drowsiness, headache, lightheadedness and dizziness. Rarely: Ataxia and mental confusion. Isolated Cases: Muscular weakness and visual disturbances.
Blood: Isolated Cases: Transient leukopenia; eosinophilia, thrombocytopenia and thrombocytopenic purpura are encountered more frequently under intermittent therapy than on continuous daily treatment, during which they occur only in isolated cases.
Endocrine Reactions: Rarely, disturbances in the menstrual cycle; induction of a crisis in Addison patients (see Interactions).
Unwanted Effects Chiefly Occurring During Intermittent Therapy or Upon Resumption of Treatment After Temporary Interruption: In patients taking rifampicin other than daily or in those resuming treatment with the drug after a temporary interruption, an influenza-like syndrome ("flu syndrome") may set in, this being very probably of immunopathological origin. It is characterized by fever, shivering and possibly headache, dizziness and pain in the limbs. In rare cases, the "flu syndrome" may be followed by thrombocytopenia, purpura, dyspnea, asthma-like attacks, hemolytic anemia, shock and acute renal failure. These serious complications may, however, also set in suddenly with no preceding "flu syndrome", chiefly when treatment is resumed after a temporary interruption or when rifampicin is given only once a week in high doses (≥25 mg/kg). When rifampicin is administered in lower doses (600 mg) 2-3 times a week, the syndrome is only rarely encountered, its incidence then being comparable to that observed during daily medication.
Isoniazid:
Central and Peripheral Nervous System: Frequently, peripheral neuropathy (usually preceded by paresthesias of feet and hands, dose-dependent and more common in undernourished patients, in alcoholics and in diabetics); rarely, damage to the optic nerve, convulsions, psychoses, dizziness, lightheadedness, headache. Isolated Cases: Toxic encephalopathy. High doses may increase the frequency of seizures in epileptics.
Gastrointestinal Tract: Occasionally, nausea, vomiting, epigastric distress.
Liver: Frequently, disturbances of liver function (usually transient); rarely, hepatitis, which in isolated instances may be severe; the frequency of hepatitis rises with increasing age.
The common prodromal symptoms of severe hepatitis are anorexia, nausea, vomiting, fatigue, malaise and weakness. The frequency of progressive liver damage increases with age.
It is rare in persons <20, but occurs in up to 2.3% of those >50 years.
Hematological Reactions: Isolated cases of agranulocytosis, eosinophilia, thrombocytopenia, anemia (hemolytic, hypoplastic).
Allergic and Miscellaneous Reactions: Occasional: Drug rash and fever. Rarely: Dryness of the mouth, heartburn, disorders of micturition, rheumatic syndrome, lupus erythematosus-like signs and symptoms, pellagra. Isolated Cases: Gynecomastia and vasculitis, lymphadenopathy, hyperglycemia, metabolic acidosis.
Pyrazinamide:
Liver: The liver toxicity of pyrazinamide depends on the dosage, the duration of treatment and concomitant therapy. It can vary from occasional mild liver disorders eg, a transient increase in serum transaminase levels to isolated cases of acute yellow atrophy of the liver. Rarely, attacks of porphyria.
Gastrointestinal Tract: Nausea, anorexia, vomiting, diarrhea and abdominal pain may occur. Aggravation of peptic ulcer.
Urogenital System: Decreased renal excretion of uric acid, resulting in hyperuricemia, may occur with pyrazinamide in dosages exceeding 2 g/day.
Occasionally, arthralgia and rarely, attacks of gout have been reported; these always proved reversible after the drug had been withdrawn or the dosage decreased and appropriate therapy given.
Blood: Rarely, sideroblastic anemia, thrombocytopenia.
Central Nervous System: Mild fever and malaise may occur.
Skin: Allergic skin reactions, including urticaria, rash, flushing, pruritus, burning sensations and photosensitization have been observed.


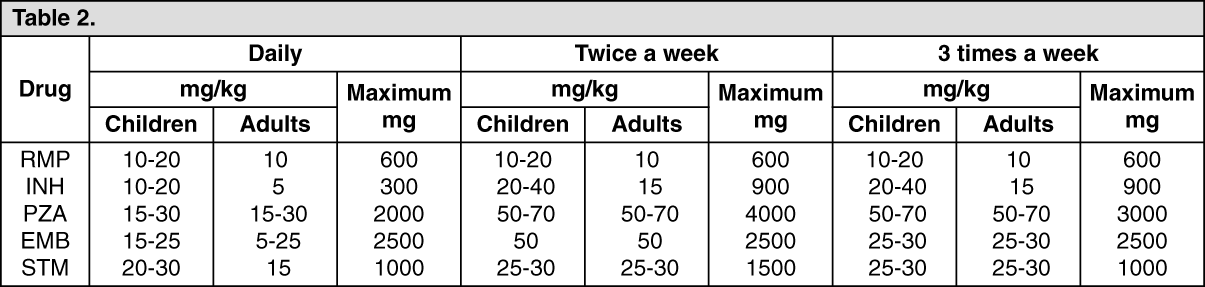 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out