Pharmacology: Pharmacodynamics: In healthy subjects receiving a single dose of Samsca 60 mg, the onset of the aquaretic and sodium increasing effects occurs within 2-4 hrs post-dose. A peak effect of about a 6-mEq increase in serum sodium and about 9 mL/min increase in urine excretion rate is observed between 4 and 8 hrs post-dose; thus, the pharmacological activity lags behind the plasma concentrations of tolvaptan. About 60% of the peak effect on serum sodium is sustained at 24 hrs post-dose, but the urinary excretion rate is no longer elevated by this time. Tolvaptan doses >60 mg do not increase aquaresis or serum sodium further. The effects of tolvaptan in the recommended dose range of 15-60 mg once daily appear to be limited to aquaresis and the resulting increase in sodium concentration.
In a parallel-arm, double-blind (for tolvaptan and placebo), placebo- and positive-controlled, multiple-dose study of the effect of tolvaptan on the QTc interval, 172 healthy subjects were randomized to tolvaptan 30 mg, tolvaptan 300 mg, placebo or moxifloxacin 400 mg once daily. At both, the 30-mg and 300-mg doses, no significant effect of administering tolvaptan on the QTc interval was detected on day 1 and 5. At the 300-mg dose, peak tolvaptan plasma concentrations were approximately 4-fold higher than the peak concentrations following a 30-mg dose. Moxifloxacin increased the QT interval by 12 millisec at 2 hrs after dosing on day 1 and 17 millisec at 1 hr after dosing on day 5, indicating that the study was adequately designed and conducted to detect tolvaptan's effect on the QT interval, had an effect been present.
Mechanism of Action: Tolvaptan is a selective vasopressin V
2-receptor antagonist with an affinity for the V
2-receptor that is 1.8 times that of native arginine vasopressin (AVP). Tolvaptan affinity for the V
2-receptor is 29 times greater than for the V
1a-receptor. When taken orally, tolvaptan 15-60 mg doses antagonize the effect of vasopressin and cause an increase in urine water excretion that results in an increase in free water clearance (aquaresis), a decrease in urine osmolality and a resulting increase in serum sodium concentrations. Urinary excretion of sodium and potassium and plasma potassium concentrations are not significantly changed. Tolvaptan metabolites have no or weak antagonist activity for human V
2-receptors compared with tolvaptan.
Plasma concentrations of native AVP may increase (average 2-9 pg/mL) with tolvaptan administration.
Clinical Studies: Hyponatremia: In 2 double-blind, placebo-controlled, multicenter studies (SALT-1 and SALT-2), a total of 424 patients with euvolemic or hypervolemic hyponatremia (serum sodium <135 mEq/L) resulting from a variety of underlying causes [heart failure, liver cirrhosis, syndrome of inappropriate antidiuretic hormone (SIADH) and others] were treated for 30 days with tolvaptan or placebo, then followed for an additional 7 days after withdrawal. Symptomatic patients, patients likely to require saline therapy during the course of therapy, patients with acute and transient hyponatremia associated with head trauma or postoperative state and patients with hyponatremia due to primary polydipsia, uncontrolled adrenal insufficiency or uncontrolled hypothyroidism were excluded. Patients were randomized to receive either placebo (N=220) or tolvaptan (N=223) at an initial oral dose of 15 mg once daily. The mean serum sodium concentration at study entry was 129 mEq/L. Fluid restriction was to be avoided if possible during the first 24 hrs of therapy to avoid overly rapid correction of serum sodium and during the first 24 hrs of therapy, 87% of patients had no fluid restriction. Thereafter, patients could resume or initiate fluid restriction (defined as daily fluid intake of ≤1 L/day) as clinically indicated.
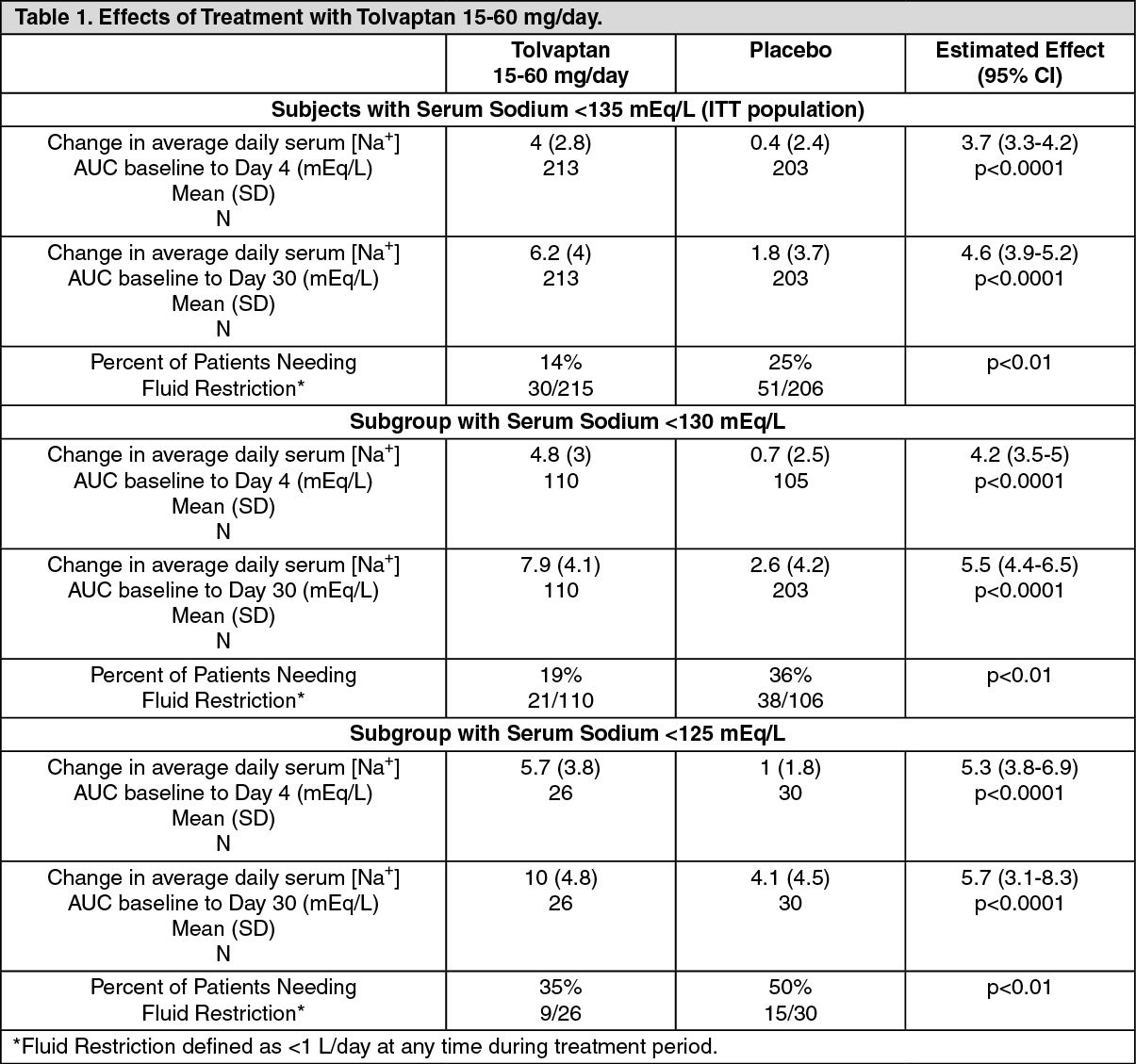
The dose of tolvaptan could be increased at 24-hr intervals to 30 mg once daily, then to 60 mg once daily, until either the maximum dose of 60 mg or normonatremia (serum sodium >135 mEq/L) was reached. Serum sodium concentrations were determined at 8 hrs after study drug initiation and daily up to 72 hrs, within which time titration was typically completed. Treatment was maintained for 30 days with additional serum sodium assessments on days 11, 18, 25 and 30. On the day of study discontinuation, all patients resumed previous therapies for hyponatremia and were reevaluated 7 days later. The primary endpoint for these studies was the average daily area under the concentration-time curve (AUC) for change in serum sodium from baseline to day 4 and baseline to day 30 in patients with a serum sodium <135 mEq/L. Compared to placebo, tolvaptan caused a statistically greater increase in serum sodium (p<0.0001) during both periods in both studies (see Table 1). For patients with a serum sodium of <130 mEq/L or <125 mEq/L, the effects at day 4 and day 30 remained significant (see Table 1). This effect was also seen across all disease etiology subsets [eg, congestive heart failure (CHF), cirrhosis, SIADH/other].
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In patients with hyponatremia (defined as <135 mEq/L), serum sodium concentration increased to a significantly greater degree in tolvaptan-treated patients compared to placebo-treated patients as early as 8 hrs after the 1st dose and the change was maintained for 30 days. The percentage of patients requiring fluid restriction (defined as ≤1 L/day at any time during the treatment period) was also significantly less (p<0.0017) in the tolvaptan-treated group (30/215, 14%) as compared with the placebo-treated group (51/206, 25%).
Figure 1 shows the change from baseline in serum sodium by visit in patients with serum sodium <135 mEq/L. Within 7 days of tolvaptan discontinuation, serum sodium concentrations in tolvaptan-treated patients declined to levels similar to those of placebo-treated patients.
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In the open-label study SALTWATER, 111 patients, 94 of them hyponatremic (serum sodium <135 mEq/L), previously on tolvaptan or placebo therapy were given tolvaptan as a titrated regimen (15-60 mg once daily) after having returned to standard care for at least 7 days. By this time, their baseline mean serum sodium concentration had fallen to between their original baseline and post-placebo therapy level. Upon initiation of therapy, average serum sodium concentrations increased to approximately the same levels as observed for those previously treated with tolvaptan and were sustained for at least a year. Figure 3 shows results from 111 patients enrolled in the SALTWATER Study.
Click on icon to see table/diagram/image
Heart Failure: In a phase 3 double-blind, placebo-controlled study (EVEREST), 4133 patients with worsening heart failure were randomized to tolvaptan or placebo as an adjunct to standard of care. Long-term tolvaptan treatment (mean duration of treatment of 0.75 years) had no demonstrated effect, either favorable or unfavorable, on all-cause mortality [HR (95% CI): 0.98 (0.9, 1.1)] or the combined endpoint of cardiovascular mortality or subsequent hospitalization for worsening heart failure [HR (95% CI): 1 (0.9, 1.1)].
Adjunct Treatment of Volume Overload in Heart Failure (Japanese Data): The efficacy of oral administration of Samsca at 15 mg for 7 days in congestive heart failure patients with volume overload despite the use of a conventional diuretic was evaluated in a double-blind phase 3 study. Changes in body weight from baseline at the end of treatment, the primary efficacy endpoint, were -1.54±1.61 kg (mean±SD) in the Samsca 15-mg group (baseline: 59.42±12.3 kg, n=53) and -0.45±0.93 kg in the placebo group (baseline: 55.68±12.6 kg, n=57), showing that Samsca 15 mg significantly decreased body weight compared with placebo (p<0.0001, t-test). A marked reduction in body weight was observed in the Samsca 15-mg group on day 1, with subsequent decrease during the treatment period (see Figure 4). Signs and symptoms associated with cardiac edema, including jugular venous distention, hepatomegaly and lower limb edema, were also improved at the end of treatment (see Table 2).
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics: In healthy subjects, the pharmacokinetics of tolvaptan after single doses of up to 480 mg and multiple doses up to 300 mg once daily have been examined. Area under the concentration-time curve increases proportionally with dose. After administration of doses ≥60 mg, however, maximum plasma concentration (C
max) increases less than proportionally with dose. The pharmacokinetic properties of tolvaptan are stereospecific, with a steady-state ratio of the S-(-) to the R-(+) enantiomer of about 3. The absolute bioavailability of tolvaptan is approximately 56%. At least 40% of the dose is absorbed as tolvaptan or metabolites. Peak concentrations of tolvaptan are observed between 2 and 4 hrs post-dose. Food does not impact the bioavailability of tolvaptan.
In vitro data indicate that tolvaptan is a substrate and inhibitor of P-gp. Tolvaptan is highly plasma protein bound (99%) and distributed into an apparent volume of distribution of about 3 L/kg. Tolvaptan is eliminated entirely by nonrenal routes and mainly, if not exclusively, metabolized by CYP3A. After oral dosing, clearance is about 4 mL/min/kg and the terminal phase half-life (t
½) is about 12 hrs. The accumulation factor of tolvaptan with the once-daily regimen is 1.3 and the trough concentrations amount to ≤16% of the peak concentrations, suggesting a dominant t
½ somewhat shorter than 12 hrs. There is marked intersubject variation in peak and average exposure to tolvaptan with a percent coefficient of variation ranging between 30% and 60%.
In patients with hyponatremia of any origin, the clearance of tolvaptan is reduced to about 2 mL/min/kg. Moderate or severe hepatic impairment or congestive heart failure decrease the clearance, and increase the volume of distribution of tolvaptan, but the respective changes are not clinically relevant. Exposure and response to tolvaptan in subjects with creatinine clearance (CrCl) ranging between 79 and 10 mL/min and patients with normal renal function are not different.
Special Populations: Use in Patients with Hepatic Impairment: In a population pharmacokinetic analysis in patients with hyponatremia of various origin, moderate to severe hepatic impairment did not affect exposure to tolvaptan to a clinically relevant extent.
In a population pharmacokinetic analysis in patients with hepatic edema, AUC of tolvaptan in severely (Child-Pugh class C) and moderately (Child-Pugh classes A and B) hepatic impaired patients were 3.1 and 2.3 times higher than that in healthy subjects.
Use in Patients with Renal Impairment: Samsca has been studied in subjects with varying degrees of renal function following a single 60-mg dose. Samsca AUC in subjects with CrCl <30 mL/min was approximately 1.9 times higher than that in subjects with CrCl >60 mL/min but there was no correlation between Samsca AUC and changes in pharmacodynamic endpoints (urine volume, fluid intake, creatinine and free water clearances, urinary excretions of creatinine, Na
+ and K
+). No dose adjustment is necessary. Exposure and response to tolvaptan in patients with a CrCl <10 mL/min or in patients on chronic dialysis have not been studied. No benefit can be expected in patients who are anuric (see Contraindications).
Use in Patients with Congestive Heart Failure: In a population pharmacokinetic analysis in patients with hyponatremia of various origin, there was no clinically relevant increase in exposure to tolvaptan in patients with hyponatremia secondary to congestive heart failure.
In a clinical pharmacology study, AUC of tolvaptan in patients with cardiac edema (congestive heart failure) was 3.4 times higher than that in healthy subjects.
Toxicology: Nonclinical Toxicology: Carcinogenicity, Mutagenicity and Impairment of Fertility: Up to 2 years of oral administration of tolvaptan to male and female rats at doses up to 1000 mg/kg/day [162 times the maximum recommended human dose (MRHD) on a body surface area basis], to male mice at doses up to 60 mg/kg/day (5 x MRHD) and to female mice at doses up to 100 mg/kg/day (8 x MRHD) did not increase the incidence of tumors.
Tolvaptan tested negative for genotoxicity in
in vitro (bacterial reverse mutation assay and chromosomal aberration test in Chinese hamster lung fibroblast cells) and
in vivo (rat micronucleus assay) test systems.
In a fertility study in which male and female rats were orally administered, tolvaptan at 100, 300 or 1000 mg/kg/day, the highest dose level was associated with significantly fewer
corpora lutea and implants than control.
Reproductive and Developmental Toxicology: In pregnant rats, oral administration of tolvaptan at 10, 100 and 1000 mg/kg/day during organogenesis was associated with a reduction in maternal body weight gain and food consumption at 100 and 1000 mg/kg/day and reduced fetal weight and delayed ossification of fetuses at 1000 mg/kg/day (162 x MRHD on a body surface area basis). Oral administration of tolvaptan at 100, 300 and 1000 mg/kg/day to pregnant rabbits during organogenesis was associated with reductions in maternal body weight gain and food consumption at all doses and abortions at mid- and high-doses. At 1000 mg/kg/day (324 x MRHD), increased incidences of embryofetal death, fetal microphthalmia, open eyelids, cleft palate, brachymelia and skeletal malformations were observed. There are no adequate and well-controlled studies of Samsca in pregnant women. Samsca should be used in pregnancy only if the potential benefit justifies the risk to the fetus.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image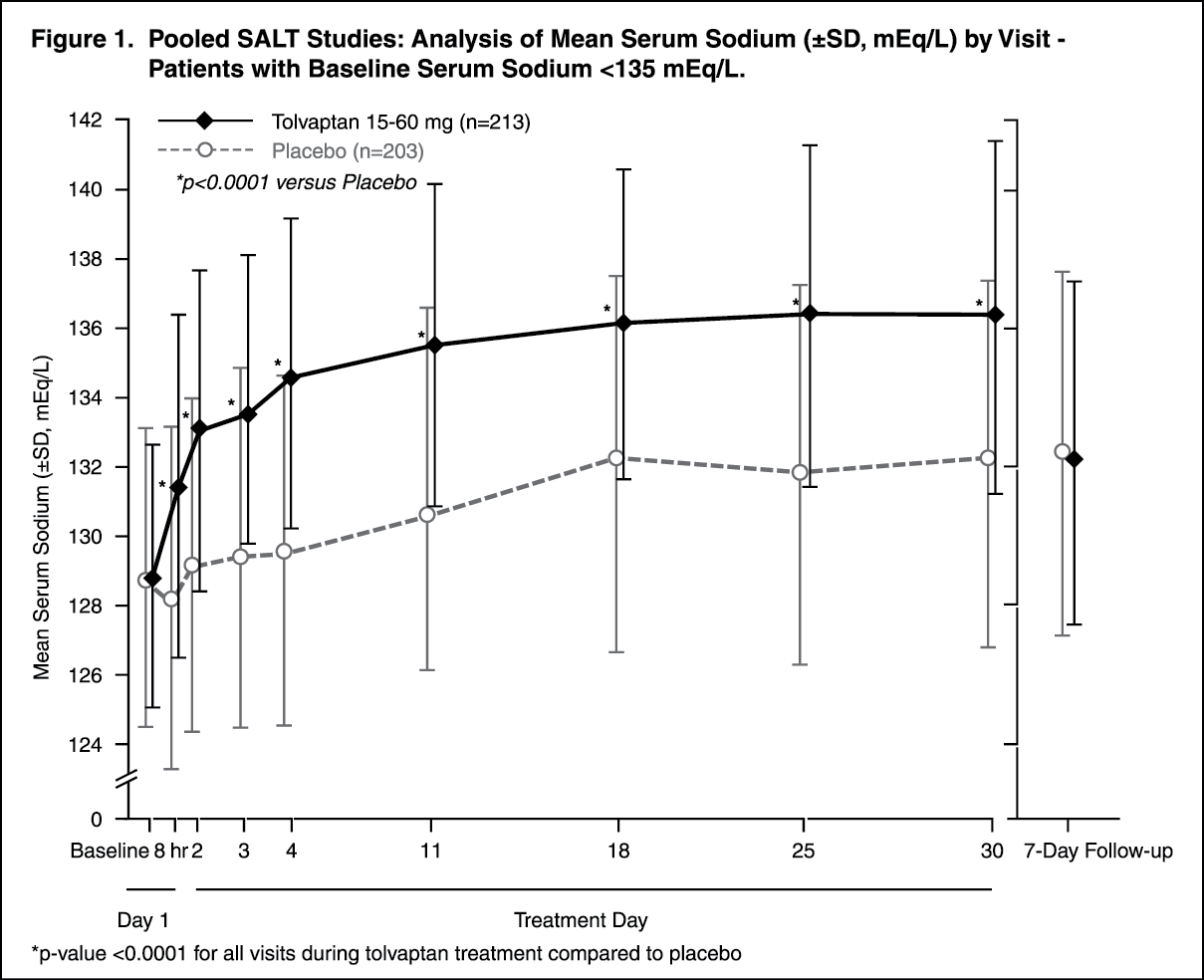 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image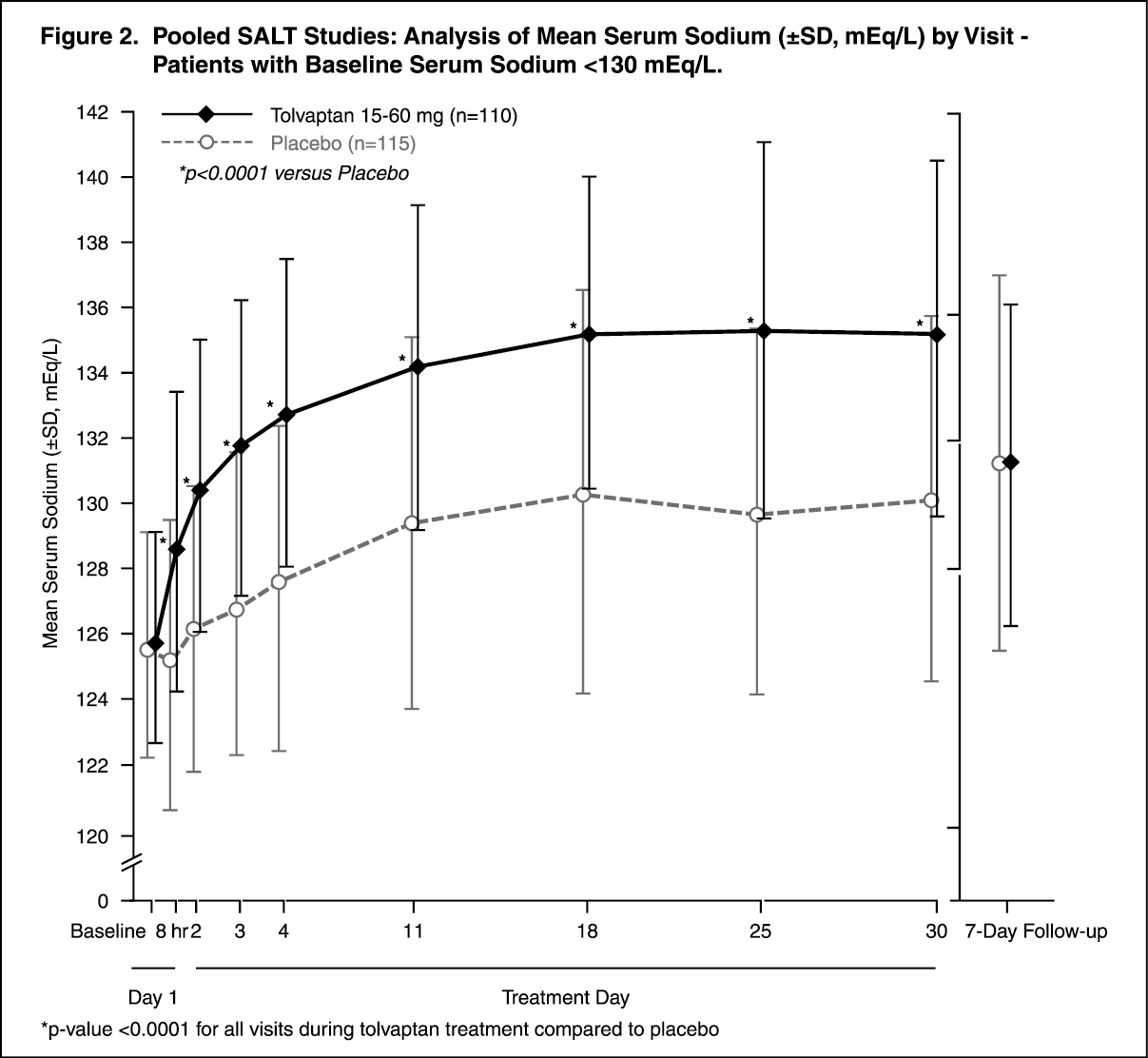 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image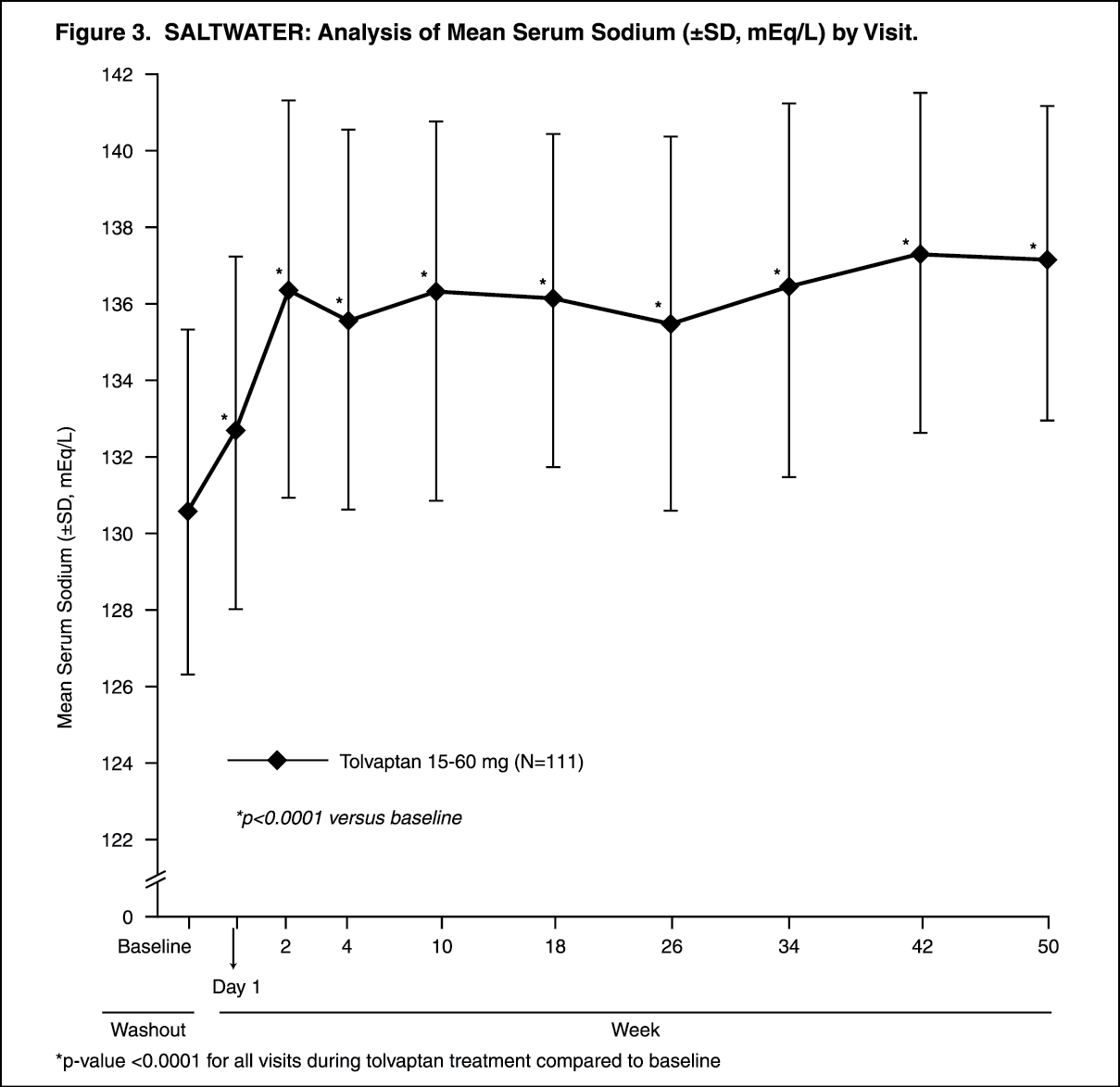 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image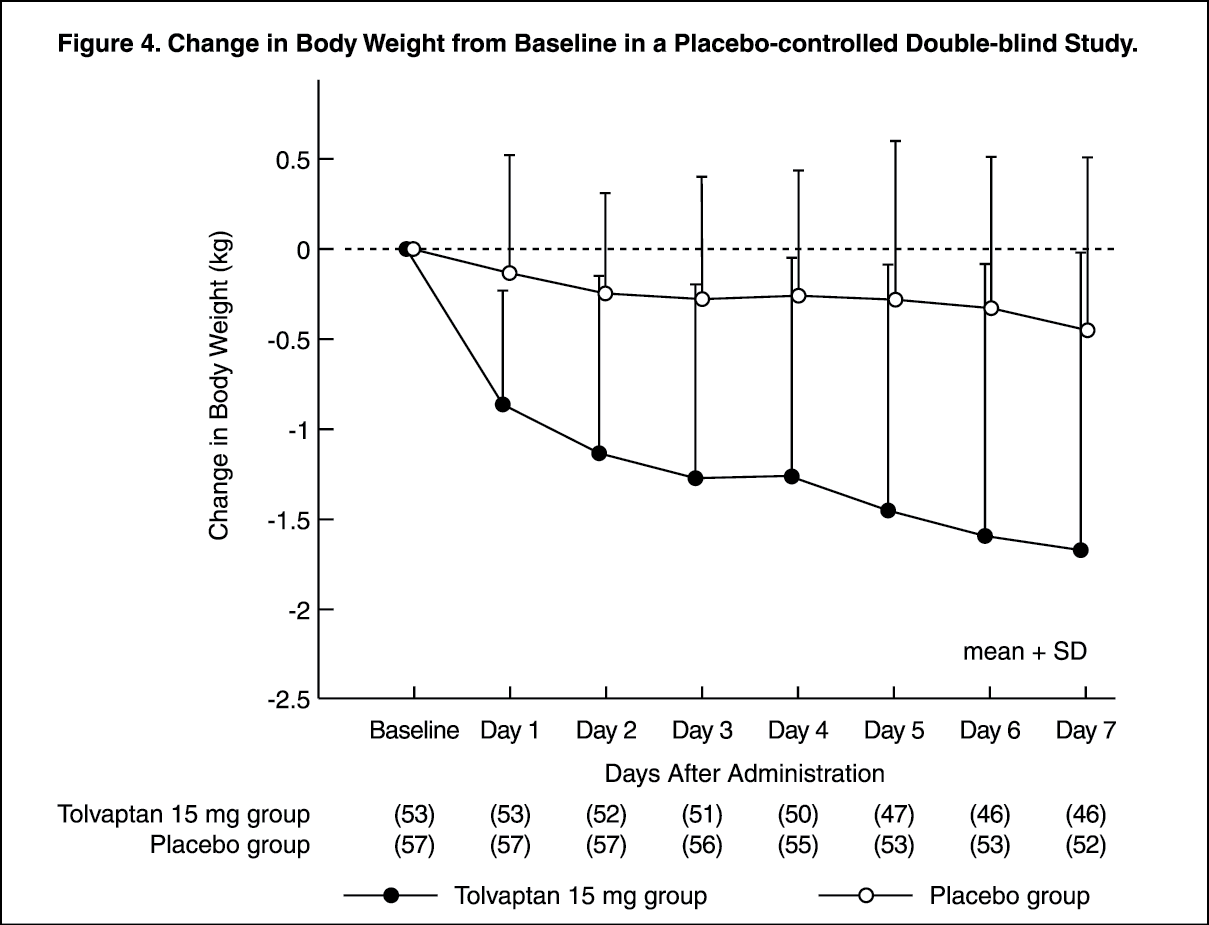 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image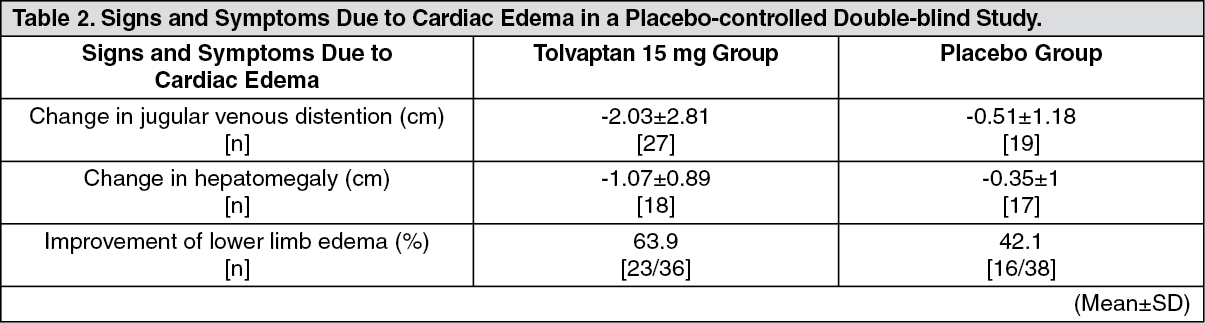 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
