Adverse effect with cefepime and tazobactam are similar to those reported with cefepime alone and generally are transient and mild to moderate in severity.
Adverse event reported for Cefepime are: Incidence equal to or greater than 1%: Local reactions (3.0%), including phlebitis (1.3%), pain and/or inflammation (0.6%)*; rash (1.1%).
Incidence less than 1% but greater than 0.1%: Colitis (including pseudomembranous colitis), diarrhea, fever, headache, nausea, oral moniliasis, pruritus, urticaria, vaginitis, vomiting.
At the higher dose of 2 g every 8 hours, the incidence of probably-related adverse events was higher among the 795 patients who received this dose of cefepime. They consisted of rash (4%), diarrhea (3%), nausea (2%), vomiting (1%), pruritus (1%), fever (1%), and headache (1%).
The following adverse laboratory changes, irrespective of relationship to therapy with cefepime, were reported as:
Incidence equal to or greater than 1%: Positive Coombs' test (without hemolysis) (16.2%); decreased phosphorus (2.8%); increased ALT/SGPT (2.8%), AST/SGOT (2.4%), eosinophils (1.7%); abnormal PTT (1.6%), PT (1.4%).
Incidence less than 1% but greater than 0.1%: Increased alkaline phosphatase, BUN, calcium, creatinine, phosphorus, potassium, total bilirubin; decreased calcium*, hematocrit, neutrophils, platelets, WBC.
Postmarketing Experience: The following adverse experiences have been reported during worldwide postmarketing experience (survey) of Cefepime injection.
As with some other drugs in this class, encephalopathy (disturbance of consciousness including confusion, hallucinations, stupor, and coma), myoclonus, and seizures have been reported. Although most cases occurred in patients with renal impairment who received doses of cefepime that exceeded the recommended dosage schedules, some cases of encephalopathy occurred in patients receiving a dosage adjustment for their renal function. If seizures associated with drug therapy occur, the drug should be discontinued. Anticonvulsant therapy can be given if clinically indicated. Precautions should be taken to adjust daily dosage in patients with renal insufficiency or other conditions that may compromise renal function to reduce antibiotic concentrations that can lead or contribute to these and other serious adverse events, including renal failure. As with other cephalosporins, anaphylaxis including anaphylactic shock, transient leukopenia, neutropenia, agranulocytosis and thrombocytopenia have been reported.
Cephalosporin-class Adverse Reactions: In addition to the adverse reactions listed previously that have been observed in patients treated with cefepime, the following adverse reactions and altered laboratory tests have been reported for cephalosporin-class antibiotics: Stevens-Johnson syndrome, erythematic multiforme, toxic epidermal necrolysis, renal dysfunction, toxic nephropathy, aplastic anemia, hemolytic anemia, hemorrhage, hepatic dysfunction including cholestasis, and pancytopenia.


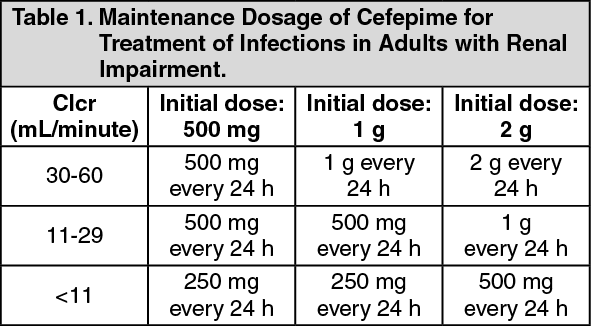 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image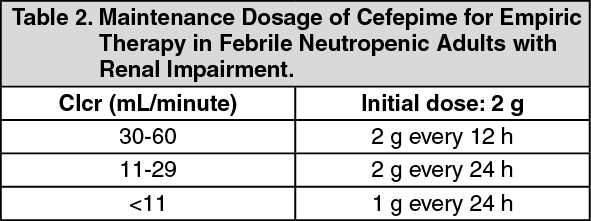 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out