Pharmacotherapeutic group: Interleukin inhibitors.
ATC code: L04AC10.
Pharmacology: Mechanism of action (MOA): Secukinumab is a fully human IgG1 antibody that selectively binds to and neutralizes the proinflammatory cytokine interleukin-17A (IL-17A). Secukinumab works by targeting IL-17A and inhibiting its interaction with the IL-17 receptor, which is expressed on various cell types including keratinocytes and synoviocytes. As a result, secukinumab inhibits the release of proinflammatory cytokines, chemokines and mediators of tissue damage and reduces IL-17A-mediated contributions to autoimmune and inflammatory diseases. Clinically relevant levels of secukinumab reach the skin and reduce local inflammatory markers. As a direct consequence treatment with secukinumab reduces erythema, induration, and desquamation present in plaque psoriasis lesions.
IL-17A is a naturally occurring cytokine that is involved in normal inflammatory and immune responses. IL-17A plays a key role in the pathogenesis of plaque psoriasis, psoriatic arthritis and axial spondyloarthritis (ankylosing spondylitis and non-radiographic axial spondyloarthritis). Increased numbers of IL-17A producing lymphocytes and innate immune cells and increased levels of IL-17A have been found in the blood of patients with plaque psoriasis, psoriatic arthritis, axial spondyloarthritis and affected skin of patients with plaque psoriasis. IL-17A is highly up-regulated in lesional skin in contrast to non-lesional skin of plaque psoriasis patients. Furthermore higher frequency of IL-17-producing cells was detected in the synovial fluid of patients with psoriatic arthritis. The frequency of IL-17 producing cells was also significantly higher in the subchondral bone marrow of facet joints from patients with axial spondyloarthritis. Inhibition of IL-17A was shown to be effective in the treatment of AS, thus establishing the key role of this cytokine in axial spondyloarthritis (see Clinical Studies as follows).
IL-17A also promotes tissue inflammation, neutrophil infiltration, bone and tissue destruction, and tissue remodeling including angiogenesis and fibrosis.
Pharmacodynamics: Serum levels of total IL-17A (free and secukinumab-bound IL-17A) are increased due to reduced clearance of secukinumab-bound IL-17A within 2 to 7 days in patients receiving secukinumab, indicating that secukinumab selectively captures free IL-17A which plays a key role in the pathogenesis of plaque psoriasis.
In a study with secukinumab, infiltrating epidermal neutrophils and various neutrophil associated markers that are increased in lesional skin of plaque psoriasis patients were significantly reduced after one to two weeks of treatment.
Secukinumab has been shown to lower (within 1 to 2 weeks of treatment) levels of C-reactive protein, which is a marker of inflammation in psoriatic arthritis and axial spondyloarthritis (ankylosing spondylitis and non-radiographic axial spondyloarthritis).
Clinical Studies: Psoriasis: Adult patients: The safety and efficacy of secukinumab were assessed in four randomized, double-blind, placebo-controlled phase 3 studies in patients with moderate to severe plaque psoriasis who were candidates for phototherapy or systemic therapy [ERASURE, FIXTURE, FEATURE, JUNCTURE]. The efficacy and safety of secukinumab 150 mg and 300 mg were evaluated versus either placebo or etanercept. In addition, one study assessed a chronic treatment regimen versus a 'retreatment as needed' regimen [SCULPTURE].
Of the 2,403 patients who were included in the placebo-controlled studies, 79% were biologic-naïve, 45% were non-biologic failures, 8% were biologic failures, 6% were anti-TNF failures, and 2% were anti-p40 failures. Baseline disease characteristics were generally consistent across all treatment groups with a median baseline Psoriasis Area Severity Index (PASI) score from 19 to 20, IGA mod 2011 baseline score ranged from "moderate" (62%) to "severe" (38%), median baseline Body Surface Area (BSA) ≥27 and median Dermatology Life Quality Index (DLQI) score from 10 to 12. Approximately 15 to 25% of patients in phase III studies had psoriatic arthritis (PsA) at baseline.
Psoriasis Study 1 (ERASURE) evaluated 738 patients. Patients randomized to secukinumab received 150 mg or 300 mg doses at weeks 0, 1, 2, 3 and 4 followed by the same dose every month. Patients randomized to receive placebo who were non-responders at week 12 were then crossed over to receive secukinumab (either 150 mg or 300 mg) at weeks 12, 13, 14, and 15, followed by the same dose every month starting at week 16. All patients were followed for up to 52 weeks following first administration of study treatment.
Psoriasis Study 2 (FIXTURE) evaluated 1,306 patients. Patients randomized to secukinumab received 150 mg or 300 mg doses at weeks 0, 1, 2, 3 and 4 followed by the same dose every month. Patients randomized to etanercept received 50 mg doses twice per week for 12 weeks followed by 50 mg every week. Patients randomized to receive placebo who were non-responders at week 12 then crossed over to receive secukinumab (either 150 mg or 300 mg) at weeks 12, 13, 14, and 15, followed by the same dose every month starting at week 16. All patients were followed for up to 52 weeks following first administration of study treatment.
Psoriasis Study 3 (FEATURE) evaluated 177 patients using a pre-filled syringe compared with placebo after 12 weeks of treatment to assess the safety, tolerability, and usability of secukinumab self-administration via the pre-filled syringe. Patients randomized to secukinumab received 150 mg or 300 mg doses at weeks 0, 1, 2, 3 and 4 followed by the same dose every month. Patients were also randomized to receive placebo at weeks 0, 1, 2, 3 and 4 followed by the same dose every month.
Psoriasis Study 4 (JUNCTURE) evaluated 182 patients using a pre-filled pen compared with placebo after 12 weeks of treatment to assess the safety, tolerability, and usability of secukinumab self-administration via the pre-filled pen. Patients randomized to secukinumab received 150 mg or 300 mg doses at weeks 0, 1, 2, 3, and 4 followed by the same dose every month. Patients were also randomized to receive placebo at weeks 0, 1, 2, 3 and 4 followed by the same dose every month.
Psoriasis Study 5 (SCULPTURE) evaluated 966 patients. All patients received secukinumab 150 mg or 300 mg doses at weeks 0, 1, 2, 3, 4, 8 and 12 and then were randomized to receive either a maintenance regimen of the same dose every month starting at Week 12 or a "retreatment as needed" regimen of the same dose. Patients randomized to "retreatment as needed" did not achieve adequate maintenance of response and therefore a fixed monthly maintenance regimen is recommended.
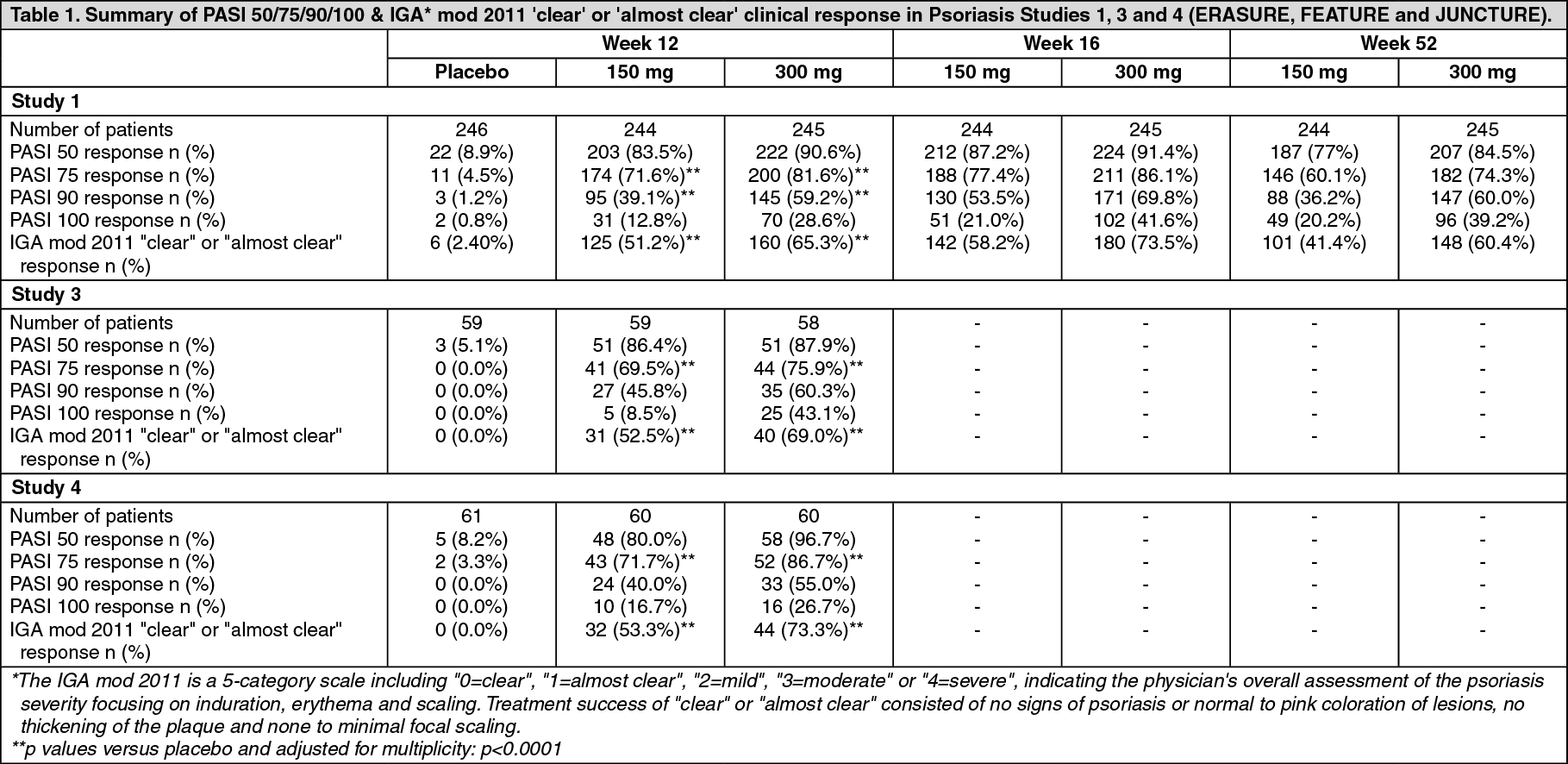
The co-primary endpoints in the placebo and active controlled studies were the proportion of patients who achieved a PASI 75 response and IGA mod 2011 'clear' or 'almost clear' response versus placebo at Week 12 (see Tables 1 and 2). The 300 mg dose provided improved skin clearance across efficacy endpoints of PASI 75/90/100, and IGA mod 2011 'clear' or 'almost clear' responses across all studies with peak effects seen at week 16, therefore this dose is recommended. (See Tables 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
An additional psoriasis study (CLEAR) evaluated 676 patients. Secukinumab 300 mg met the primary and secondary endpoints by showing superiority to ustekinumab based on PASI 90 response at Week 16 (primary endpoint), speed of onset of PASI 75 response at Week 4, and long-term PASI 90 response at Week 52. Greater efficacy of secukinumab compared to ustekinumab for the endpoints PASI 75/90/100 and IGA mod 2011 0 or 1 response ("clear" or "almost clear") was observed early and continued through Week 52. (See Table 3.)
Click on icon to see table/diagram/image
Secukinumab was efficacious in biologic-naive, biologic/anti-TNF-exposed and biologic/anti-TNF-failure patients.
Secukinumab was associated with a fast onset of efficacy as shown in the figure as follows with a 50% reduction in mean PASI by week 3 for 300 mg. (See figure.)
Click on icon to see table/diagram/image
All plaque psoriasis phase III studies included approximately 15 to 25% of patients with concurrent psoriatic arthritis at baseline. Improvements in PASI 75 in this patient population were similar to those in the overall plaque psoriasis population.
In the placebo controlled studies 1 and 2 in the subset of psoriatic arthritis patients, physical function was assessed using the HAQ Disability Index (HAQ-DI). In these studies, patients treated with 150 mg or 300 mg secukinumab showed greater improvement from baseline in the HAQ-DI score (mean decreases of -27.5% and -50.2% at week 12) compared to placebo (-8.9%). This improvement was maintained up to week 52.
Specific locations/forms of plaque psoriasis: In two additional placebo-controlled studies, improvement was seen in both nail psoriasis (TRANSFIGURE, 198 patients) and palmoplantar plaque psoriasis (GESTURE, 205 patients). In the TRANSFIGURE study, secukinumab was superior to placebo at Week 16 (46.1% for 300 mg, 38.4% for 150 mg and 11.7% for placebo) as assessed by significant improvement from baseline in the Nail Psoriasis Severity Index (NAPSI %) for patients with moderate to severe plaque psoriasis with nail involvement. In the GESTURE study, secukinumab was superior to placebo at Week 16 (33.3% for 300 mg, 22.1% for 150 mg, and 1.5% for placebo) as assessed by significant improvement of ppIGA 0 or 1 response ("clear" or "almost clear") for patients with moderate to severe palmoplantar psoriasis.
The placebo-controlled SCALP study evaluated 102 patients with moderate to severe scalp psoriasis, defined as having a Psoriasis Scalp Severity Index (PSSI) score of ≥12, an IGA mod 2011 scalp only score of 3 or greater, and at least 30% of the scalp affected. In this study, 62% of patients had at least 50% or more of scalp surface area affected. Secukinumab 300 mg was superior to placebo at Week 12 as assessed by significant improvement from baseline in both the PSSI 90 response (52.9% vs. 2.0%) and IGA mod 2011 0 or 1 scalp only response (56.9% vs. 5.9%). Greater efficacy of secukinumab 300 mg over placebo for both endpoints was observed by Week 3. Improvement in both endpoints was sustained for secukinumab patients who continued treatment through Week 24 (PSSI 90 response 58.8% and IGA mod 2011 0 or 1 scalp only response 62.7%).
Quality of Life/Patient reported outcomes: Statistically significant improvements at week 12 (Studies 1-4) from baseline compared to placebo were demonstrated in the DLQI (Dermatology Life Quality Index), these improvements were maintained for 52 weeks (Studies 1 and 2).
Statistically significant improvements at week 12 from baseline compared to placebo (Studies 1 and 2) in patient reported signs and symptoms of itching, pain and scaling were demonstrated in the validated Psoriasis Symptom Diary.
Statistically significant improvements at Week 4 from baseline in patients treated with secukinumab compared to patients treated with ustekinumab (CLEAR) were demonstrated in the DLQI (Dermatology Life Quality Index), and these improvements were maintained for up to 52 weeks. The Work Productivity and Activity Impairment Questionnaire-Psoriasis outcomes (WPAI-PSO) showed greater improvement in patients treated with secukinumab compared to patients treated with ustekinumab.
Statistically significant improvements in patient reported signs and symptoms of itching, pain and scaling at Week 16 and Week 52 (CLEAR) were demonstrated in the Psoriasis Symptom Diary in patients treated with secukinumab compared to patients treated with ustekinumab.
Statistically significant improvements at Week 12 from baseline compared to placebo (SCALP) were demonstrated in the HRQoL (Health Related Quality of Life Index) as measured by Scalpdex. These improvements were observed starting at Week 4 and were maintained through 24 weeks.
Statistically significant improvements (decreases) at week 12 from baseline (SCALP) were demonstrated in patient reported signs and symptoms of scalp itching (-59.4%), pain (-45.9%), and scaling (-69.5%), whereas placebo treated patients demonstrated worsening (increases) in scalp itching (7.7%) and pain (38.5%), and less improvement in scalp scaling (-4.7%).
Pediatric patients: Severe plaque psoriasis: A 52-week, randomized, double-blind, placebo and etanercept-controlled phase III study enrolled 162 pediatric patients 6 to less than 18 years of age, with severe plaque psoriasis (as defined by a PASI score ≥20, an IGA mod 2011 score of 4, and involving ≥10% of the body surface area) who were candidates for systemic therapy. Approximately 43% had prior exposure to phototherapy, 53% to conventional systemic therapy, 3% to biologics, and 9% had concomitant psoriatic arthritis.
Patients were randomized to receive one of the following four treatments: low dose secukinumab (75 mg for body weight <50 kg or 150 mg for body weight ≥50 kg) at Weeks 0, 1, 2, 3, and 4 followed by the same dose every 4 weeks; high dose secukinumab (75 mg for body weight <25 kg, 150 mg for body weight ≥25 kg and <50 kg, or 300 mg for body weight ≥50 kg) at Weeks 0, 1, 2, 3, and 4 followed by the same dose every 4 weeks; placebo at Weeks 0, 1, 2, 3, and 4 followed by the same dose every 4 weeks; etanercept (0.8 mg/kg) weekly (up to a maximum of 50 mg).
Patients randomized to receive placebo who were non-responders at Week 12 were switched to either the secukinumab low or high dose group (dose based on body weight group) and received study drug at Weeks 12, 13, 14, and 15, followed by the same dose every 4 weeks starting at Week 16.
The co-primary endpoints were the proportion of patients who achieved a reduction in PASI score of at least 75% (PASI 75) and IGA mod 2011 'clear' or 'almost clear' (0 or 1) with at least a 2 point improvement from baseline to Week 12. The key secondary endpoint was the proportion of patients who achieved a reduction in PASI score of at least 90% (PASI 90) from baseline to Week 12. Other secondary endpoints included PASI 50, 100 responder rates at Week 12, PASI 50, 75, 90, 100 and IGA 0/1 responder rates at Week 16 and over time up to and including Week 52, change in PASI score over time up to and including Week 52 and IGA score over time up to and including Week 52, the proportion of patients with a Children's Dermatology Life Quality Index (CDLQI) score of 0 or 1 at Week 12 and over time up to and including Week 52, and change from baseline in CDLQI compared to placebo at Week 12 and over time up to and including Week 52.
During the 12 week placebo-controlled period, the efficacy of both the low and the high dose of secukinumab was comparable for the co-primary endpoints. The odds ratio estimates in favor of both secukinumab doses were clinically relevant and statistically significant for both the PASI 75 and IGA mod 2011 'clear' or 'almost clear' (0 or 1) responses.
All patients were followed for efficacy and safety during the 52 weeks following the first dose. The proportion of patients achieving PASI 75 and IGA mod 2011 'clear' or 'almost clear' (0 or 1) responses showed separation between secukinumab treatment groups and placebo at the first post-baseline visit at Week 4, the difference becoming more prominent at Week 12. The response was maintained throughout the 52 week time period. Improvement in PASI 50, 90, 100 responder rates and CDLQI 0 or 1 scores were also maintained throughout the 52 week time period.
In addition, PASI 75, IGA 0 or 1, PASI 90 response rates at Weeks 12 and 52 for both secukinumab low and high dose groups were higher than the rates for patients treated with etanercept.
Beyond Week 12, efficacy of both the low and the high dose of secukinumab was comparable although the efficacy of the high dose was higher for patients ≥50 kg. The safety profiles of the low dose and the high dose were comparable.
The efficacy results at Weeks 12 and 52 are presented in Table 4. (See Table 4.)
Click on icon to see table/diagram/image
A higher proportion of pediatric patients treated with secukinumab reported improvement in health-related quality of life as measured by a CDLQI score of 0 or 1 compared to placebo at Week 12 (low dose 44.7%, high dose 50%, placebo 15%). From Week 12 through Week 52, the proportion of pediatric patients in both secukinumab dose groups with a CDLQI score of 0 or 1 was numerically higher than for the etanercept group (low dose 60.6%, high dose 66.7%, etanercept 44.4%).
Moderate to severe plaque psoriasis: An open-label, two-arm, parallel-group, multicentre phase III study enrolled 84 pediatric patients 6 to less than 18 years of age with moderate to severe plaque psoriasis (as defined by a PASI score ≥12, an IGA mod 2011 score of ≥3, and involving ≥10% of the body surface area) who were candidates for systemic therapy.
Patients were randomized to receive secukinumab at Weeks 0, 1, 2, 3, and 4 followed by the same dose every 4 weeks as follows: low dose secukinumab (75 mg for body weight <50 kg or 150 mg for body weight ≥50 kg); high dose secukinumab (75 mg for body weight <25 kg, 150 mg for body weight between ≥25 kg and <50 kg, or 300 mg for body weight ≥50 kg).
The co-primary endpoints were the proportion of patients who achieved a reduction in PASI score of at least 75% (PASI 75) and IGA mod 2011 'clear' or 'almost clear' (0 or 1) with at least a 2 point improvement from baseline to Week 12. Secondary and additional endpoints included PASI 90 response at Week 12, PASI 75, 90, 100, and IGA mod 2011 'clear' or 'almost clear' (0 or 1), and CDLQI responses over time up to end of treatment.
The efficacy of both the low and the high dose of secukinumab was comparable and showed statistically and clinically meaningful improvement compared to historical placebo for the co-primary endpoints. The odds ratio estimates in favor of both secukinumab doses were clinically relevant and statistically significant for both the PASI 75 and IGA mod 2011 0 or 1 responses versus historical placebo. The estimated posterior probability of a positive treatment effect was 100%.
All patients were followed for efficacy for at least 24 weeks following first administration. Efficacy (defined as PASI 75 response and IGA mod 2011 'clear' or 'almost clear' [0 or 1]) was observed as early as Week 2 and the proportion of patients who achieved a PASI 75 response and IGA mod 2011 'clear' or 'almost clear' (0 or 1) increased throughout the 24-week time period. Improvement in PASI 90 and PASI 100 were also observed at Week 12 and increased throughout the 24-week time period.
Beyond Week 12, efficacy of both the low and the high dose of secukinumab was comparable.
The safety profiles of the low dose and the high dose were comparable.
The efficacy results at Weeks 12 and 24 are presented in Table 5. (See Table 5.)
Click on icon to see table/diagram/image
In the low dose group, 50% and 70.7% of patients achieved a CDLQI 0 or 1 score at Weeks 12 and 24, respectively. In the high dose group, 61.9% and 60.5% achieved a CDLQI 0 or 1 score at Weeks 12 and 24, respectively.
Psoriatic arthritis: The safety and efficacy of secukinumab were assessed in 1,999 patients in three randomized, double-blind, placebo-controlled phase III studies in patients with active psoriatic arthritis (≥3 swollen and ≥3 tender joints) despite non-steroidal anti-inflammatory drug (NSAID), corticosteroids or disease-modifying anti-rheumatic drug (DMARD) therapy. Over 61% and 42% of the PsA patients had enthesitis and dactylitis at baseline, respectively.
The efficacy and safety of secukinumab 75 mg, 150 mg and/or 300 mg were evaluated versus placebo with either an i.v. or s.c. loading dose regimen. In Psoriatic Arthritis 1 Study (PsA1 Study), Psoriatic Arthritis 2 Study (PsA2 Study) and Psoriatic Arthritis 3 Study (PsA3 Study), 29%, 35% and 30% of patients, respectively, were previously treated with an anti-TNFα agent and discontinued the anti-TNFα agent for either lack of efficacy or intolerance (anti-TNFα-IR patients).
PsA1 Study (FUTURE 1) evaluated 606 patients, of whom 60.7% had concomitant MTX. Patients randomized to secukinumab received 10 mg/kg, i.v., at Weeks 0, 2, and 4, followed by either 75 mg or 150 mg s.c. every month starting at Week 8. Patients randomized to receive placebo who were non-responders at Week 16 were then crossed over to receive secukinumab (either 75 mg or 150 mg) at Week 16 followed by the same dose every month. Patients randomized to receive placebo who were responders at Week 16 were then crossed over to receive secukinumab (either 75 mg or 150 mg) at Week 24 followed by the same dose every month. The primary endpoint was American College of Rheumatology (ACR) 20 response at Week 24.
PsA2 Study (FUTURE 2) evaluated 397 patients, of whom 46.6% had concomitant MTX. Patients randomized to secukinumab received 75 mg, 150 mg or 300 mg s.c. at Weeks 0, 1, 2, 3 and 4 followed by the same dose every month. Patients randomized to receive placebo who were non-responders at Week 16 were then crossed over to receive secukinumab (either 150 mg or 300 mg, s.c.) at Week 16 followed by the same dose every month. Patients randomized to receive placebo who were responders at Week 16 were crossed over to receive secukinumab (either 150 mg or 300 mg) at Week 24 followed by the same dose every month. The primary endpoint was ACR 20 response at Week 24.
PsA3 Study (FUTURE 5) evaluated 996 patients, of whom 50.1% had concomitant MTX treatment. Patients were randomized to receive secukinumab 150 mg, 300 mg, or placebo s.c. at Weeks 0, 1, 2, 3 and 4 followed by the same dose every month, or a once monthly injection of secukinumab 150 mg. Patients randomized to receive placebo who were non-responders at Week 16 were then crossed over to receive secukinumab (either 150 mg or 300 mg, s.c.) at Week 16 followed by the same dose every month. Patients randomized to receive placebo who were responders at Week 16 were crossed over to receive secukinumab (either 150 mg or 300 mg) at Week 24 followed by the same dose every month. The primary endpoint was ACR 20 response at Week 16, and the key secondary endpoint was the change from baseline in modified Total Sharp Score (mTSS) at Week 24.
Clinical response: Signs and symptoms: Treatment with secukinumab resulted in significant improvement in the measure of disease activity compared to placebo at Weeks 16, 24, and 52 (see Table 6).
Click on icon to see table/diagram/image
The onset of action of secukinumab occurred as early as Week 2. Statistically significant difference in ACR 20 vs placebo was reached at Week 3. In PsA2 efficacy responses were maintained up to Week 104.
Similar responses for primary and key secondary endpoints were seen in PsA patients regardless of whether they were on concomitant MTX treatment or not.
Both, anti-TNFα-naïve and anti-TNFα-IR secukinumab-treated patients, had a significantly higher ACR 20 response compared to placebo at Weeks 16 and 24 with a slightly higher response in the anti-TNFα-naïve group (in PsA2 anti-TNFα-naïve: 64% and 58% for 150 mg and 300 mg, respectively, compared to placebo 15.9%; anti-TNFα-IR: 30% and 46% for 150 mg and 300 mg, respectively, compared to placebo 14.3%). Anti-TNFα-IR patients on 300 mg showed higher response rates on ACR20 compared to placebo patients (p<0.05) and demonstrated clinical meaningful benefit over 150 mg on multiple secondary endpoints. Improvements in the PASI75 response were seen regardless of previous anti-TNFα exposure.
In PsA1 Study, secukinumab-treated patients demonstrated significantly improved PsA signs and symptoms at Week 24 with similar magnitude of response to PsA2 Study. Efficacy was maintained up to Week 104.
Radiographic response: In PsA3 Study, structural damage was assessed radiographically and expressed by the modified Total Sharp Score (mTSS) and its components, the Erosion Score (ES) and the Joint Space Narrowing Score (JSN). Radiographs of hands, wrists, and feet were obtained at baseline Week 16 and/or Week 24 and scored independently by at least two readers who were blinded to treatment group and visit number.
Secukinumab 150 mg and 300 mg treatment significantly inhibited the rate of progression of peripheral joint damage compared with placebo treatment as measured by change from baseline in mTSS at Week 24 (Table 7).
The percentage of patients with no disease progression (defined as a change from baseline in mTSS of ≤0.5) from randomization to Week 24 was 79.8%, 88.0% and 73.6% for secukinumab150 mg, 300 mg and placebo, respectively. An effect of inhibition of structural damage was observed irrespective of concomitant MTX use or TNF status.
Structural damage was also assessed in the PsA1 Study. Radiographs of hands, wrists, and feet were obtained at baseline and Week 24 during the double-blind period when patients were on secukinumab or placebo and at Week 52 when all patients were on open-label secukinumab.
By Week 24, secukinumab 150 mg treatment significantly inhibited the rate of progression of peripheral joint damage compared with placebo treatment as measured by change from baseline in mTSS (see Table 4). Inhibition of structural damage was maintained with secukinumab treatment up to Week 52. (See Table 7.)
Click on icon to see table/diagram/image
In PsA1, radiographic inhibition was observed in both anti-TNFα-naïve and anti-TNFα patients. Similar effect of inhibition of structural damage was observed irrespective of concomitant MTX use. Inhibition of structural damage was maintained with secukinamab treatment up to Week 104.
The percentage of patients with no-disease progression (defined as a change from baseline in mTSS of ≤0.5) from randomization to Week 24 was 82.3% in secukinumab 10 mg/kg i.v. load - 150 mg s.c. maintenance and 75.7% in placebo.
Axial manifestations in PsA: A randomized, double-blind, placebo-controlled study (MAXIMISE) assessed the efficacy of secukinumab in 485 PsA patients with axial manifestations who were naive to biologic treatment and responded inadequately to NSAIDs. The primary variable was at least a 20% improvement in Assessment of Spondyloarthritis International Society (ASAS 20) criteria at Week 12. Treatment with secukinumab 300 mg and 150 mg compared to placebo resulted in significant improvement in signs and symptoms (including greater decreases from baseline in spinal pain) and improvement in physical function (see Table 8).
Click on icon to see table/diagram/image
Improvement in ASAS 20 and ASAS 40 for both secukinumab doses were observed by Week 4 and were maintained up to 52 weeks.
Physical function and health related quality of life: In PsA2 and PsA3 Studies, patients treated with secukinumab 150 mg and 300 mg showed improvement in physical function compared to patients treated with placebo as assessed by Heath Assessment Questionnaire-Disability Index (HAQ-DI) at Week 24 and Week 16 respectively. The proportion of patients on 150 mg or 300 mg who achieved a minimal clinically important difference (MCID) of ≥0.3 improvement in HAQ-DI score from baseline was greater compared to placebo at Week 16 (PsA3: 54.8%, 62.3% vs. 35.6%; p<0.0001) and Week 24 (PsA2: 46.0%, 49.0% vs. 16.3%, p<0.0001) and the response in PsA2 was maintained up to Week 104.
There was greater improvement in Dermatology Life Quality Index (DLQI) scores in the secukinumab groups as compared to placebo at Week 24 (p<0.01). There was also greater improvement in Functional Assessment of Chronic Illness Therapy - Fatigue (FACIT-F) scores in the 150 mg and 300 mg secukinumab groups when compared to placebo at Week 24 (p<0.01), and these improvements were maintained up to Week 104 in PsA2. Secukinumab-treated patients reported significant improvements in health-related quality of life as measured by the Short Form (36) Health Survey Physical Component Summary (SF-36 PCS) score (p<0.001). Improvements were also seen for EQ-5D. In addition improvements were seen in the psoriatic arthritis QoL (PsAQoL p<0.01) and in psoriatic arthritis-related productivity at work and within household, as reported by the Work Productivity and Activity Impairment-General Health questionnaire (WPAI-GH) compared to placebo at Week 24.
In PsA1 Study, secukinumab-treated patients significantly improved physical function as assessed by HAQ-DI and SF-36 Physical Components at Week 24. Efficacy was maintained up to Week 52.
Axial spondyloarthritis (axSpA) with or without radiographic damage: Ankylosing spondylitis (AS)/axSpA with radiographic damage: The safety and efficacy of secukinumab were assessed in 816 patients in three randomized, double-blind, placebo-controlled phase III studies in patients with active ankylosing spondylitis (AS) with a Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) ≥4 despite non-steroidal anti-inflammatory drug (NSAID), corticosteroid or disease-modifying anti-rheumatic drug (DMARD) therapy. Patients in the AS1 Study and AS2 Study had a diagnosis of AS for a median of 2.7 to 5.8 years.
The efficacy and safety of secukinumab 75 mg, 150 mg, and 300 mg were evaluated versus placebo with either an i.v. or s.c. loading regimen. In Ankylosing Spondylitis 1 Study (AS1 Study), Ankylosing Spondylitis 2 Study (AS2 Study), and Ankylosing Spondylitis 3 Study (AS3 Study), 27.0%, 38.8%, and 23.5% of patients, respectively, were previously treated with an anti-TNFα agent and discontinued the anti-TNFα agent for either lack of efficacy or intolerance (anti-TNFα-IR patients).
AS1 Study (MEASURE 1) evaluated 371 patients, of whom 14.8% and 33.4% used concomitant MTX or sulfasalazine, respectively. Patients randomized to secukinumab received 10 mg/kg, i.v., at Weeks 0, 2, and 4, followed by either 75 mg or 150 mg s.c. every month. Patients randomized to receive placebo who were non-responders at Week 16 were crossed over to receive secukinumab (either 75 mg or 150 mg) at Week 16, followed by the same dose every month. Patients randomized to receive placebo who were responders at Week 16 were crossed over to receive secukinumab (either 75 mg or 150 mg) at Week 24, followed by the same dose every month. The primary end point was at least a 20% improvement in Assessment of Spondyloarthritis International Society (ASAS20) criteria at Week 16.
AS2 Study (MEASURE 2) evaluated 219 patients, of whom 11.9% and 14.2% used concomitant MTX or sulfasalazine, respectively. Patients randomized to secukinumab received 75 mg or 150 mg s.c. at Weeks 0, 1, 2, 3 and 4 followed by the same dose every month. At Week 16, patients who were randomized to placebo at baseline were re-randomized to receive secukinumab (either 75 mg or 150 mg) s.c. every month. The primary end point was ASAS 20 at Week 16.
AS3 Study (MEASURE 3) evaluated 226 patients, of whom 13.3% and 23.5% used concomitant MTX or sulfasalazine, respectively. Patients randomized to secukinumab received 10 mg/kg, i.v. at Weeks 0, 2, and 4, followed by either 150 mg or 300 mg s.c. every month. At Week 16, patients who were randomized to placebo at baseline were re-randomized to receive secukinumab (either 150 mg or 300 mg) s.c. every month. The primary end point was ASAS20 at Week 16. Patients were blinded to the treatment regimen up to Week 52, and the study continued to Week 156.
Clinical response: Signs and symptoms: In AS2 Study, treatment with secukinumab 150 mg resulted in greater improvement in ASAS20, ASAS40, high-sensitivity C-reactive protein (hsCRP), ASAS 5/6 and BASDAI score compared with placebo at Week 16 (see Table 9).
Click on icon to see table/diagram/image
The onset of action of secukinumab 150 mg occurred as early as Week 1 for ASAS20 (superior to placebo) in AS2 Study.
ASAS20 responses were improved at Week 16 in both anti-TNFα-naïve patients (68.2% vs. 31.1%; p<0.05) and anti-TNFα-IR patients (50.0% vs. 24.1%; p<0.05) for secukinumab 150 mg compared with placebo, respectively.
The magnitude of response (treatment difference versus placebo) with regards to signs and symptoms at Week 16 was similar in anti-TNFα-naïve and anti-TNFα-IR patients in both studies, with higher absolute response rates in anti-TNFα-naïve patients.
In AS3 Study, secukinumab-treated patients (150 mg and 300 mg) demonstrated improved signs and symptoms, and had comparable efficacy responses regardless of dose that were superior to placebo at Week 16 for the primary endpoint (ASAS20). Overall, the efficacy response rates for the 300 mg group were consistently greater compared to the 150 mg group for the secondary endpoints. During the blinded period, the ASAS20 and ASAS40 responses were 69.7% and 47.6% for 150 mg and 74.3% and 57.4% for 300 mg at Week 52, respectively. The ASAS20 and ASAS40 responses were maintained through Week 156 (69.5% and 47.6% for 150 mg vs. 74.8% and 55.6% for 300 mg). The ASAS partial remission (ASAS PR) responses were 9.5% and 21.1% for 150 mg and 300 mg respectively, compared to 1.3% for placebo at Week 16. The ASAS PR responses were 18.1% and 24.3% for 150 mg and 300 mg at Week 52, respectively. These responses were maintained through Week 156 (15.1% for 150 mg and 27.2% for 300 mg).
Physical function and health-related quality of life: In AS2 Study, patients treated with secukinumab 150 mg showed improvements by Week 16 compared to placebo-treated patients in physical function as assessed by the BASFI (-2.15 vs -0.68, p <0.0001) and in pain as assessed by the Total and Nocturnal Back Pain scale (-29.64 vs -9.64, p<0.0001). Secukinumab-treated patients reported improvements compared to placebo-treated patients in tiredness (fatigue) as reported at Week 16 by scores on the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-Fatigue) scale and in health-related quality of life as measured by ASQoL (LS mean change: -4.00 vs -1.37, p<0.001) and SF-36 Physical Component Summary (SF-36 PCS) (LS mean change: 6.06 vs 1.92, p <0.001). Secukinumab 150 mg had numerically larger mean improvements than placebo for three of the four Work Productivity and Activity Impairment-General Health (WPAI-GH) outcomes at Week 16. These improvements were sustained up to Week 52.
In AS1 Study, secukinumab-treated patients reported improvement in physical function compared to placebo-treated patients at Week 16, as assessed by the BASFI, Total and Nocturnal Back Pain scale, FACIT-Fatigue, ASQoL, EQ-5D and SF-36 Physical Component Summary. Numerically greater increases in work productivity as measured with the WPAI-GH were also observed at Week 16 (tests of significance not performed). These improvements in physical function were all sustained up to Week 52.
Non-radiographic axial spondyloarthritis (nr-axSpA)/axSpA without radiographic damage: The safety and efficacy of secukinumab were assessed in 555 patients in one randomized, double-blind, placebo-controlled phase III study in patients with active non-radiographic axial spondyloarthritis (nr-axSpA) fulfilling the Assessment of Spondyloarthritis International Society (ASAS) classification criteria for axial spondyloarthritis (axSpA) with no radiographic evidence of changes in the sacroiliac joints that would meet the modified New York criteria for ankylosing spondylitis (AS). Patients enrolled had active disease, defined as a Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) ≥4, a Visual Analogue Scale (VAS) for total back pain of ≥40 (on a scale of 0 to 100 mm), despite current or previous non-steroidal anti-inflammatory drug (NSAID) therapy and increased C-reactive protein (CRP) and/or evidence of sacroiliitis on Magnetic Resonance Imaging (MRI). Patients in this study had a diagnosis of axSpA for a mean of 2.1 to 3.0 years and 54% of the study participants were female.
In nr-axSpA 1 Study, 57.6% of patients had increased CRP, 72.2% had evidence of sacroiliitis on MRI and 29.9% had both increased CRP and evidence of sacroiliitis on MRI. In addition, 9.7% of patients were previously treated with an anti-TNF-alpha agent and discontinued the anti-TNF-alpha agent for either lack of efficacy or intolerance (anti-TNF-alpha-IR patients).
Nr-axSpA 1 Study (PREVENT) evaluated 555 patients, of whom 9.9% and 14.8% used concomitant MTX or sulfasalazine, respectively. In the double-blind period, patients received either placebo or secukinumab for 52 weeks. Patients randomized to secukinumab received 150 mg s.c. at Weeks 0, 1, 2, 3 and 4 followed by the same dose every month, or a once monthly injection of secukinumab 150 mg. The primary endpoint was at least 40% improvement in ASAS 40 at Week 16 in TNF-naive patients.
Clinical response: Signs and symptoms: In nr-axSpA1 Study, treatment with secukinumab 150 mg resulted in significant improvements in the measures of disease activity compared to placebo at Week 16 (see Table 10).
Click on icon to see table/diagram/image
The onset of action of secukinumab 150 mg occurred as early as Week 3 for ASAS 40 in anti-TNF-alpha naive patients (superior to placebo) in nr-axSpA1 Study. Patients treated with secukinumab maintained their response compared to placebo up to Week 52.
ASAS 40 responses were also improved at Week 16 in anti-TNF-alpha-IR patients (28.6% vs. 13.3%) for secukinumab 150 mg compared with placebo. The magnitude of response (treatment difference versus placebo) with respect to signs and symptoms at Week 16 was similar in anti-TNF-alpha-naïve and anti-TNF-alpha-IR patients, with higher absolute response rates in anti-TNF-alpha-naïve patients.
Physical function and health-related quality of life: Patients treated with secukinumab 150 mg showed statistically significant improvements by Week 16 compared to placebo-treated patients in physical function as assessed by the BASFI (Week 16: -1.75 vs -1.01, p<0.01). Patients treated with secukinumab reported significant improvements compared to placebo-treated patients by Week 16 in health-related quality of life as measured by ASQoL (LS mean change: Week 16: -3.45 vs -1.84, p<0.001) and SF-36 Physical Component Summary (SF-36 PCS) (LS mean change: Week 16: 5.71 vs 2.93, p<0.001). These improvements were sustained up to Week 52.
Pharmacokinetics: Absorption: Following a single subcutaneous dose of either 150 mg or 300 mg in plaque psoriasis patients, secukinumab reached peak serum concentrations of 13.7 ± 4.8 μg/mL or 27.3 ± 9.5 μg/mL, respectively, between 5 and 6 days post dose.
After the initial weekly dosing during the first month, the time to reach the maximum concentration was between 31 and 34 days.
Peak concentrations at steady-state (C
max,ss) following subcutaneous administration of 150 mg or 300 mg were 27.6 μg/mL and 55.2 μg/mL, respectively. Steady-state is reached after 20 weeks with monthly dosing regimens.
Compared with exposure after a single dose, patients exhibited a 2-fold increase in peak serum concentrations and AUC following repeated monthly dosing during maintenance.
Secukinumab is absorbed with an average absolute bioavailability of 73%.
Distribution: The mean volume of distribution during the terminal phase (V
z) following a single intravenous administration ranged from 7.10 to 8.60 L in plaque psoriasis patients suggesting that secukinumab undergoes limited distribution to peripheral compartments.
Secukinumab concentrations in interstitial fluid in the skin of plaque psoriasis patients ranged from 28% to 39% of those in serum at 1 and 2 weeks after a single subcutaneous dose of 300 mg secukinumab.
Elimination: Mean systemic clearance (CL) was 0.19 L/d in plaque psoriasis patients. Clearance was dose- and time-independent, as expected for a therapeutic IgG1 monoclonal antibody interacting with a soluble cytokine target, such as IL-17A.
The mean elimination half-life was estimated to be 27 days in plaque psoriasis patients. Estimated half-lives in individual plaque psoriasis patients range from 17 to 41 days.
Dose linearity: The single and multiple dose pharmacokinetics of secukinumab in plaque psoriasis patients were determined in several studies with intravenous doses ranging from 1 x 0.3 mg/kg to 3 x 10 mg/kg and with subcutaneous doses ranging from 1 x 25 mg to multiple doses of 300 mg. Exposure was dose proportional across all dosing regimens.
The PK properties of secukinumab observed in psoriatic arthritis and axial spondyloarthritis (ankylosing spondylitis and non-radiographic axial spondyloarthritis) patients were similar to those displayed in plaque psoriasis patients.
Special populations: Elderly patients: Of the 3,430 plaque psoriasis patients exposed to secukinumab in clinical studies, a total of 230 were 65 years of age or older and 32 patients were 75 years of age or older.
Of the 2,536 PsA patients exposed to secukinumab in clinical studies, a total of 236 patients were 65 years of age or older and 25 patients were 75 years of age or older.
Of the 794 AS patients exposed to secukinumab in clinical studies, a total of 29 patients were 65 years of age or older and 3 patients were 75 years of age or older.
Of the 524 non-radiographic axial spondyloarthritis patients exposed to secukinumab in clinical studies, a total of 9 patients were 65 years of age or older and 2 patients were 75 years of age or older.
Based on population PK analysis, clearance in elderly patients and patients less than 65 years of age was similar.
Patients with renal and hepatic impairment: No pharmacokinetic data are available in patients with hepatic or renal impairment.
Pediatric patients: In a pool of the two pediatric studies, patients with moderate to severe plaque psoriasis (6 to less than 18 years of age) were administered secukinumab at the recommended pediatric dosing regimen. At Week 24, patients weighing ≥25 and <50 kg had a mean ± SD steady-state trough concentration of 19.8 ± 6.96 microgram/mL (n=24) after 75 mg of secukinumab, and patients weighing ≥50 kg had a mean ± SD steady-state trough concentration of 27.3 ± 10.1 microgram/mL (n=36) after 150 mg of secukinumab. The mean ± SD steady-state trough concentration in patients weighing <25 kg (n=8) was 32.6 ± 10.8 microgram/mL at Week 24 after 75 mg dose.
Toxicology: Non-Clinical Safety Data: Non-clinical data revealed no special hazard for humans based on tissue cross-reactivity testing, safety pharmacology, repeated dose and reproductive toxicity studies performed with secukinumab or a murine anti-murine IL-17A antibody.
Since secukinumab binds to cynomolgus monkey and human IL-17A, its safety was studied in the cynomolgus monkey. No undesirable effects of secukinumab were seen following subcutaneous administration to cynomolgus monkeys for up to 13 weeks and intravenous administration up to 26 weeks (including pharmacokinetic, pharmacodynamic, immunogenicity and immunotoxicity (e.g. T cell dependent antibody response and NK cell activity) evaluations). The average serum concentrations observed in monkeys after 13 weekly subcutaneous doses of 150 mg/kg are 48-fold higher than the predicted average serum concentration expected in psoriatic patients at the highest clinical dose. The exposure multiples are even higher when the average serum concentration from the 26 weeks intravenous toxicology study in cynomolgus monkeys are taken into consideration. Antibodies to secukinumab were detected in only one out of 101 animals. No non-specific tissue cross-reactivity was demonstrated when secukinumab was applied to normal human tissues.
Animal studies have not been conducted to evaluate the carcinogenic potential of secukinumab.
For information on reproductive toxicity, see Use in Pregnancy & Lactation.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image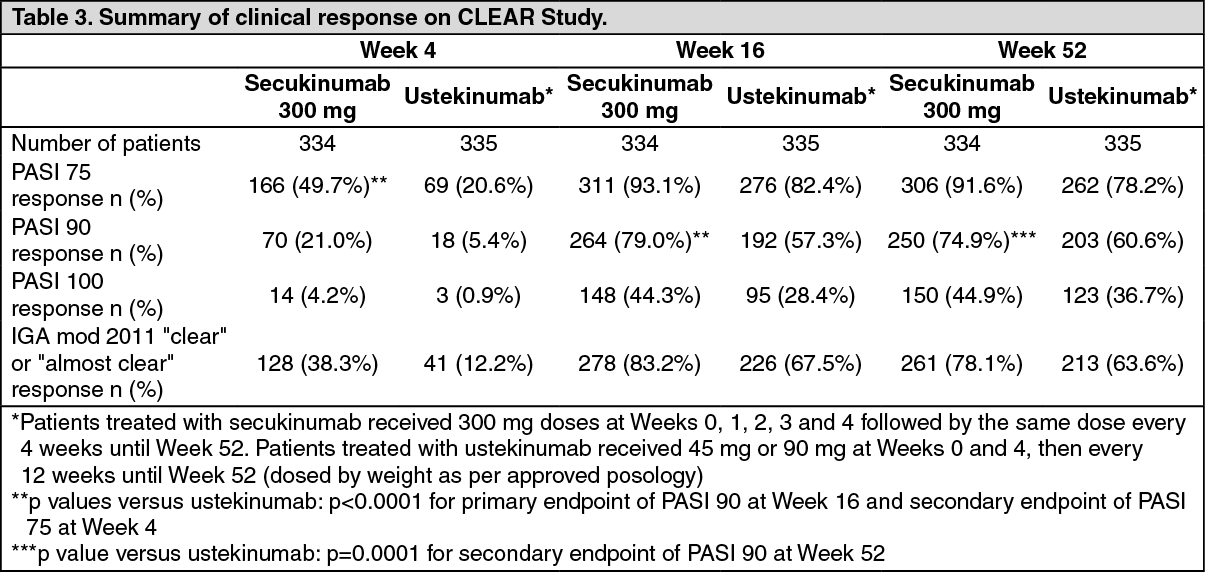 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image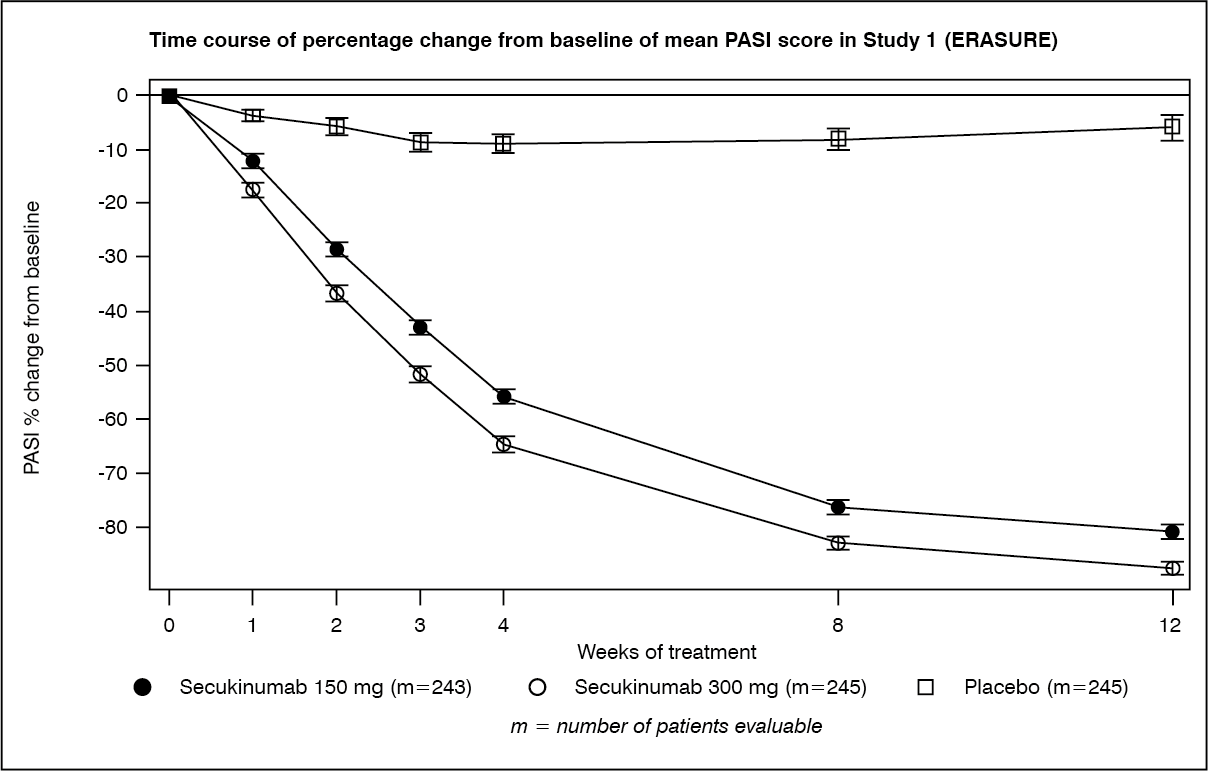 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image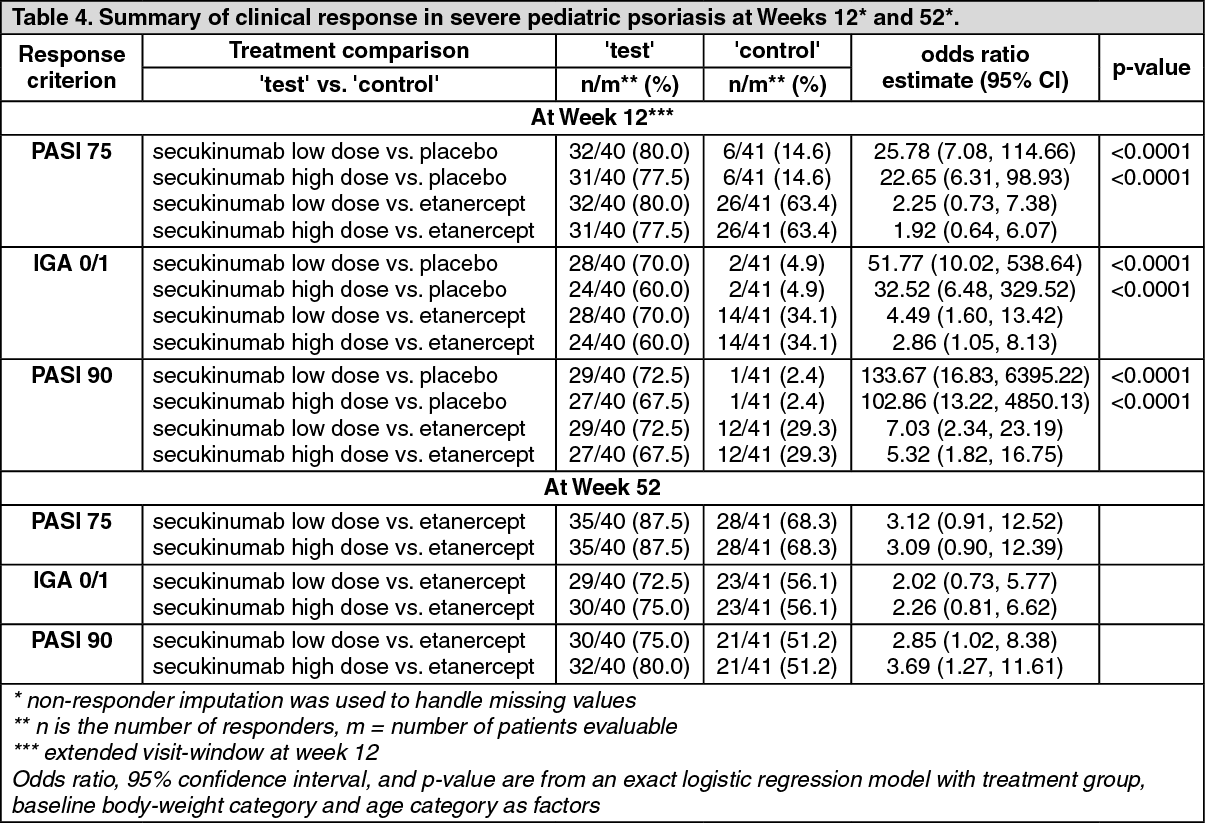 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image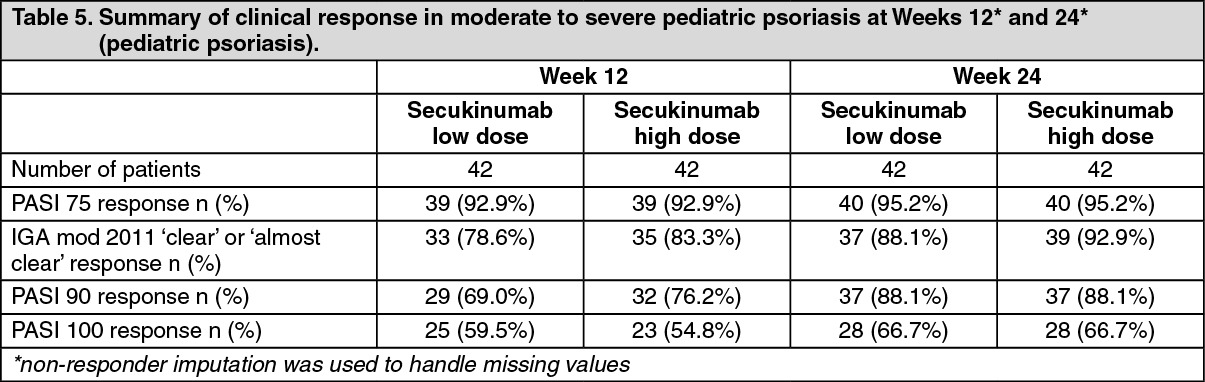 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image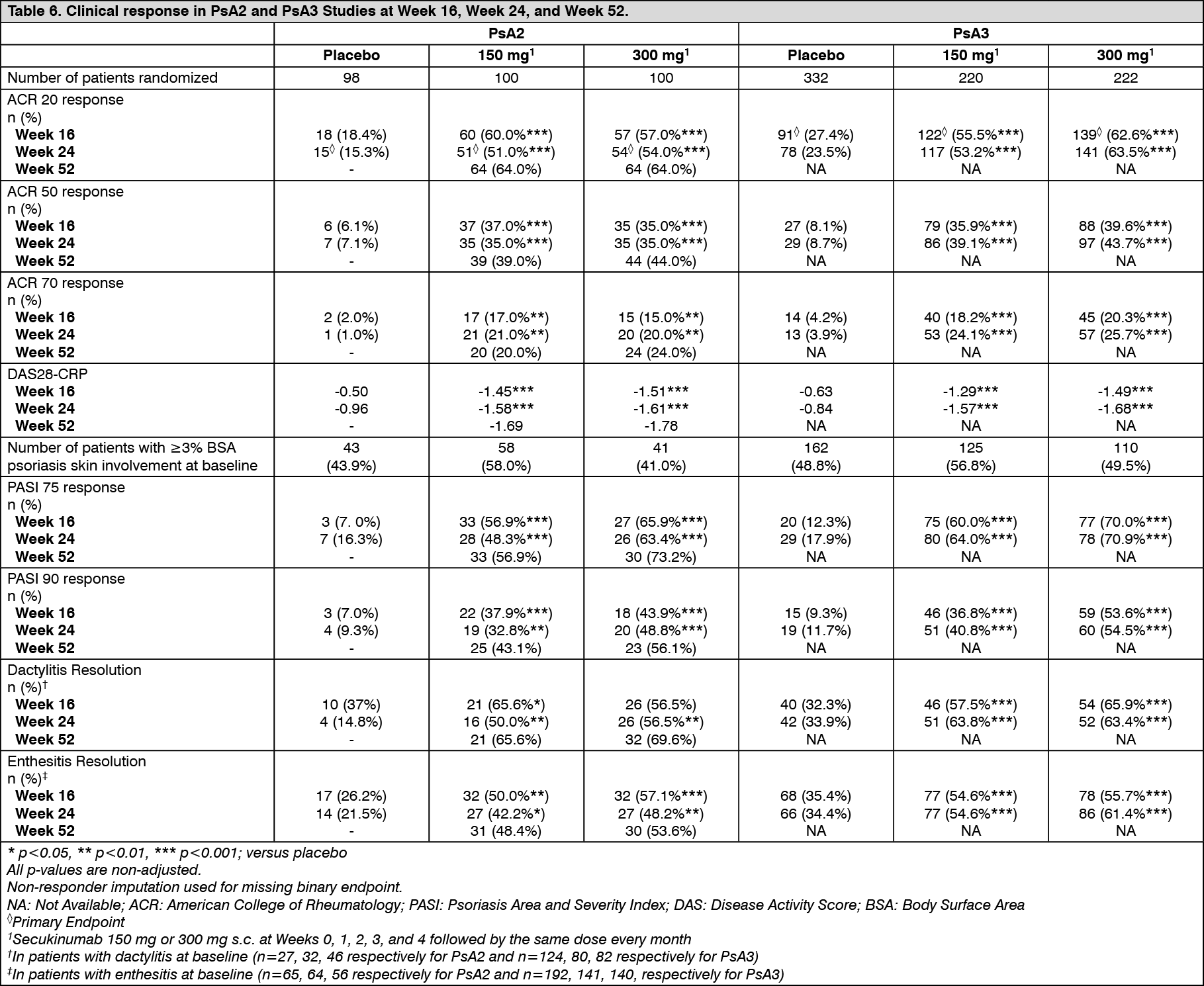 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image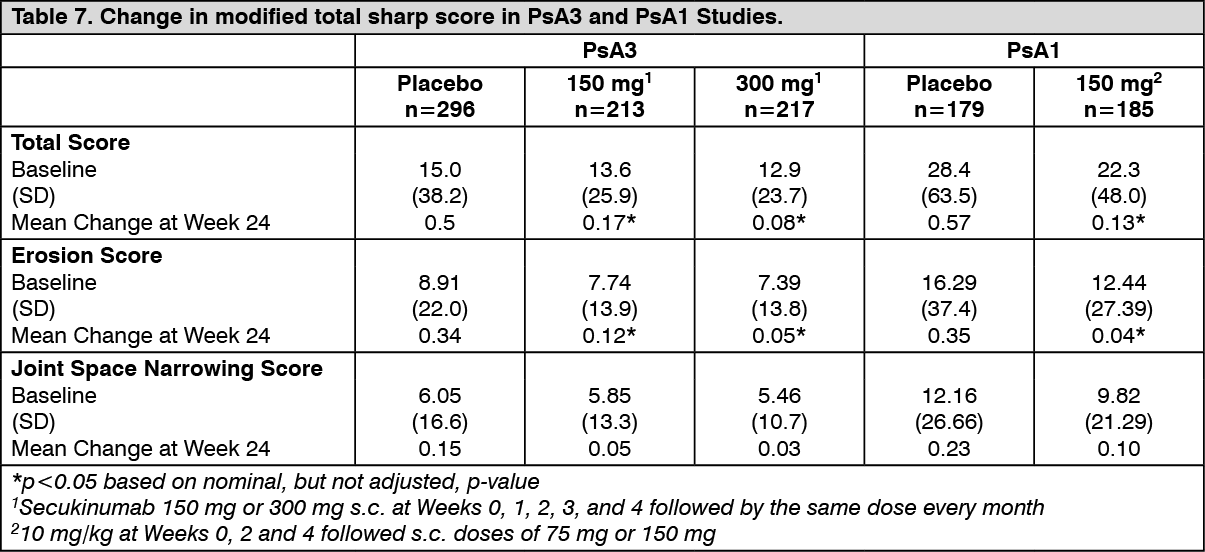 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image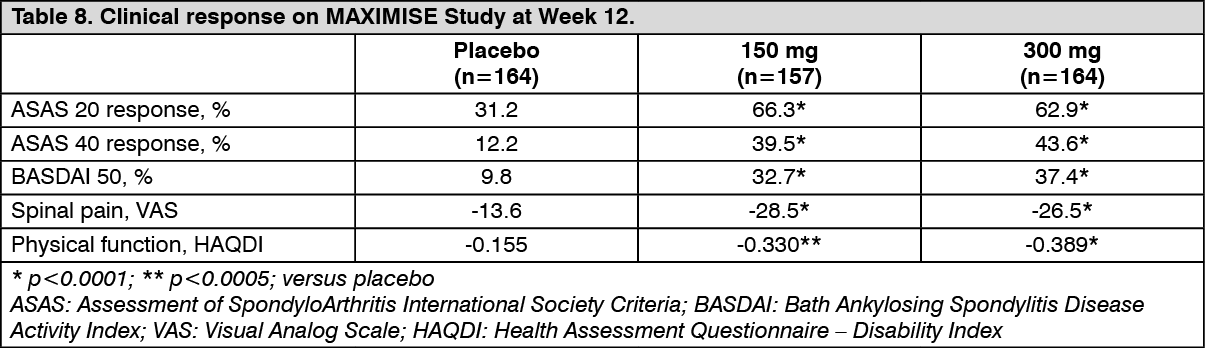 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image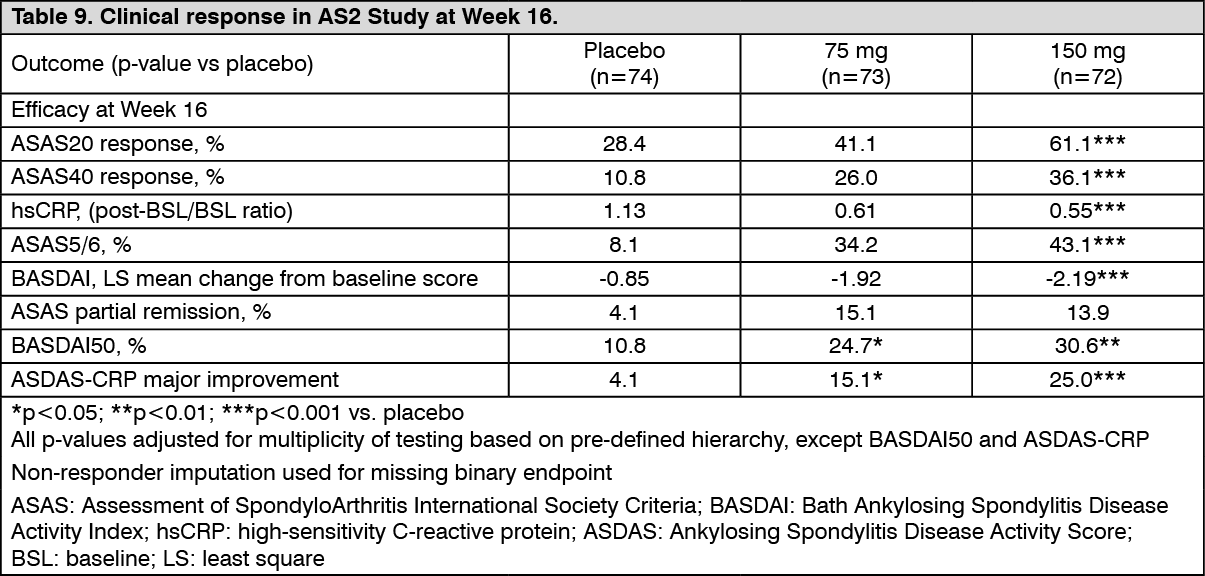 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image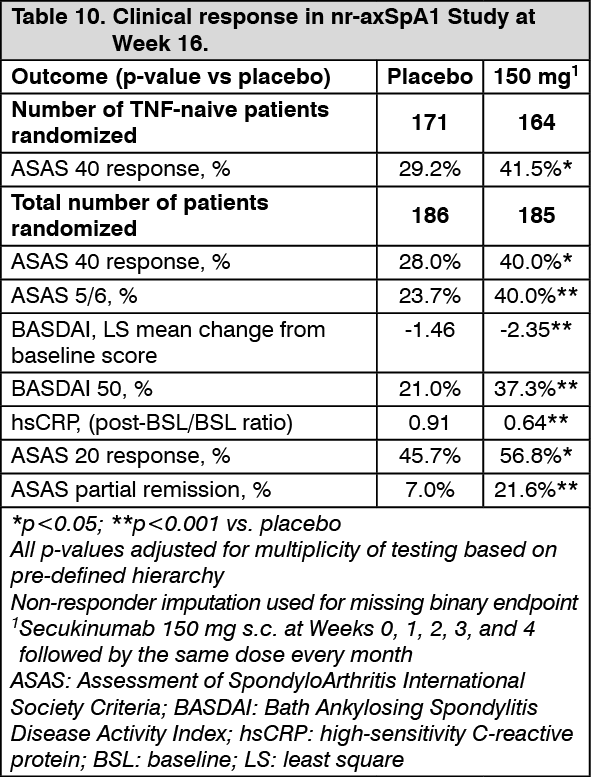 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image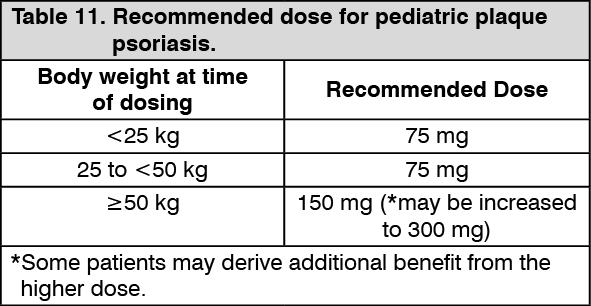 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out