


 Sign Out
Sign Out




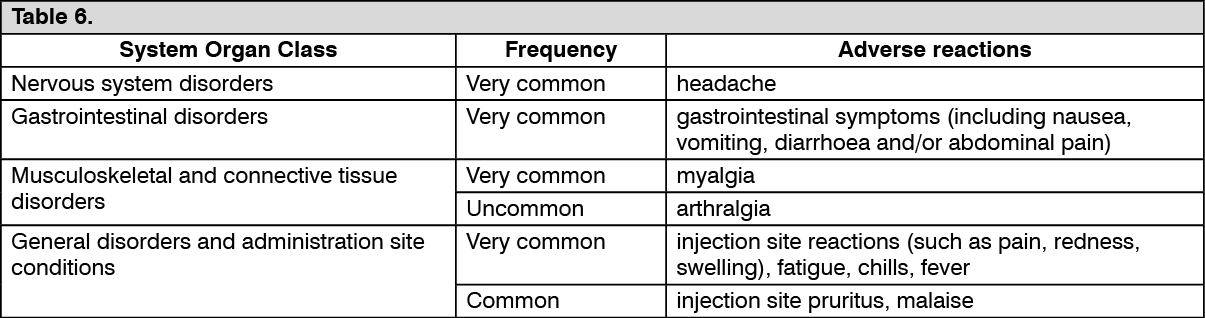
Additionally, in clinical studies, 1,587 subjects ≥ 18 years of age who are immunodeficient or immunosuppressed due to disease or therapy (referred to as immunocompromised (IC)), were vaccinated with at least 1 dose of Shingrix. The reported adverse reactions were consistent with those presented in the Table as follows.
Adverse reactions reported are listed according to the following frequency: Very common (≥1/10); Common (≥1/100 to <1/10); Uncommon (≥1/1,000 to <1/100); Rare (≥1/10,000 to <1/1,000); Very rare (<1/10,000). (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOverall, there was a higher incidence of some adverse reactions in younger age groups. However, the overall frequency and severity of these events did not indicate a clinically meaningful different reactogenicity profile in the younger age strata. In IC adult studies, there was a higher incidence of pain at the injection site, fatigue, myalgia, headache, shivering and fever in subjects aged 18 to 49 years compared with those aged 50 years and older. In older adult studies, there was a higher incidence of pain and swelling at the injection site, fatigue, myalgia, headache, shivering, fever and gastrointestinal symptoms in subjects aged 50 to 69 years compared with those aged 70 years and older.
In a clinical study where 119 subjects ≥ 50 years of age were vaccinated with Shingrix following a 0, 6-month schedule, the safety profile was similar to that observed in subjects vaccinated with Shingrix following a 0, 2-month schedule.
In a clinical study including 865 adults ≥ 50 years of age, fever and shivering were reported more frequently when PPV23 vaccine was co-administered with Shingrix (16% and 21%, respectively) compared to when Shingrix was given alone (7% for both adverse reactions).
Post-marketing data: See Table 7.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form