


 Sign Out
Sign Out

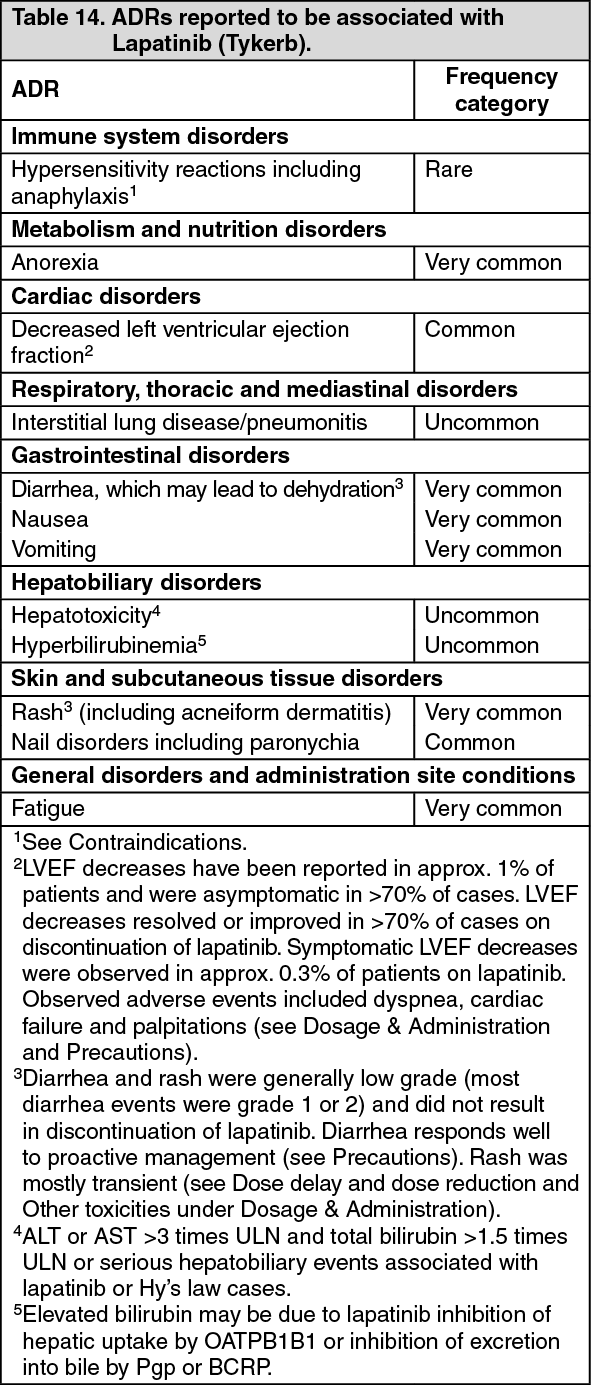
Tabulated summary of adverse drug reactions (ADRs) from clinical trials: ADRs from clinical trials are listed by MedDRA system organ class (SOC) in Tables 14 to 18. Within each SOC, the ADRs are ranked by frequency, with the most frequent first. The corresponding frequency category for each ADRs is based on the following convention (CIOMS III): very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000).
ADRs with lapatinib (Tykerb) monotherapy: The following ADRs have been reported to be associated with lapatinib (Tykerb): See Table 14.
 Click on icon to see table/diagram/image
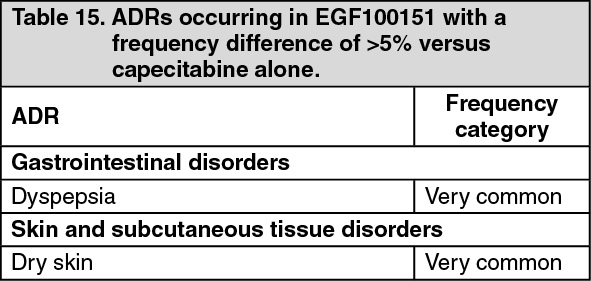
Click on icon to see table/diagram/imageADRs with lapatinib (Tykerb) in combination with capecitabine: In addition to the ADRs observed with lapatinib (Tykerb) monotherapy, the following additional ADRs were reported to be associated with lapatinib (Tykerb) in combination with capecitabine in study EGF100151 with a frequency difference of > 5% versus capecitabine alone. These data are based on exposure to this combination in 198 patients. (See Table 15.)
 Click on icon to see table/diagram/image
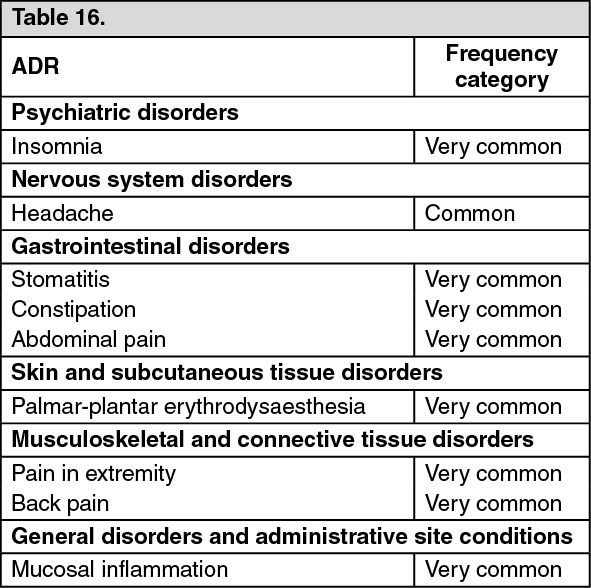
Click on icon to see table/diagram/imageThe following ADRs listed in Table 16 as follows were reported to be associated with lapatinib (Tykerb) in combination with capecitabine but were seen at a similar frequency in the capecitabine monotherapy arm. (See Table 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageADRs with lapatinib (Tykerb) in combination with trastuzumab: No additional ADRs were reported to be associated with lapatinib (Tykerb) in combination with trastuzumab. There was an increased incidence of cardiac toxicity, but these events were comparable in nature and severity to those reported from the lapatinib (Tykerb) clinical program (see Precautions). These data are based on exposure to this combination in 149 patients in the phase III study EGF104900.
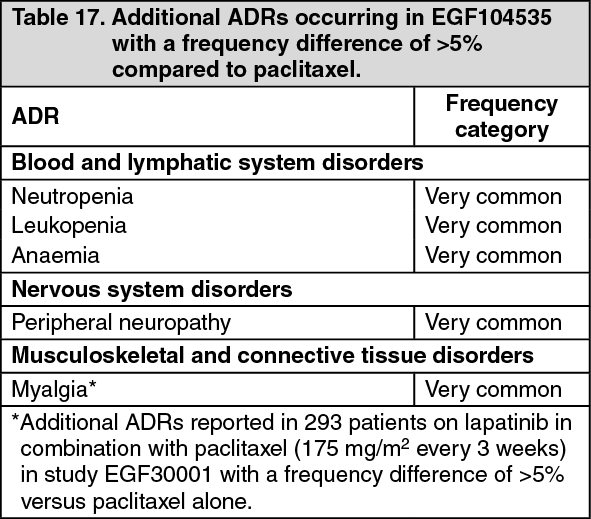
ADRs with lapatinib (Tykerb) in combination with paclitaxel: In addition to the ADRs observed with lapatinib (Tykerb) monotherapy, the following ADRs were reported to be associated with lapatinib (Tykerb) in combination with paclitaxel (80 mg/m2 weekly) with a frequency difference of >5% versus paclitaxel alone. These data are based on exposure to this combination in 222 patients in study EGF104535. (See Table 17.)
 Click on icon to see table/diagram/image
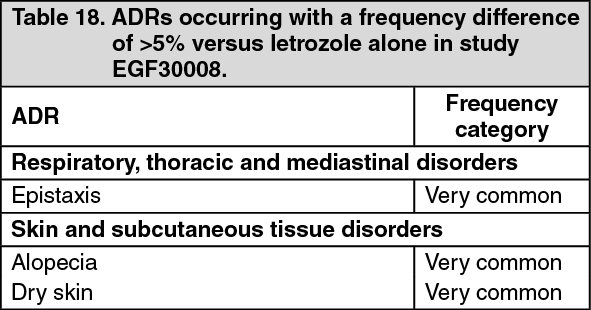
Click on icon to see table/diagram/imageAdverse reactions with lapatinib (Tykerb) in combination with letrozole: In addition to the ADRs observed with lapatinib (Tykerb) monotherapy, the following ADRs were reported to be associated with lapatinib (Tykerb) in combination with letrozole in study EGF30008 with a frequency difference of >5% versus letrozole alone. These data are based on exposure to this combination in 654 patients. (See Table 18.)
 Click on icon to see table/diagram/image
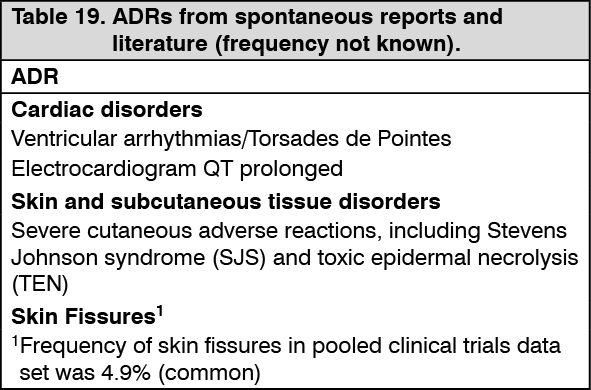
Click on icon to see table/diagram/imagePost marketing data: The following ADRs are from post-marketing experience with lapatinib (Tykerb) via spontaneous case reports and literature cases. As these reactions are reported voluntarily from a population of uncertain size, it is not possible to reliably estimate their frequency which is therefore categorized as not known. ADRs are listed according to MedDRA SOCs. Within each SOC, ADRs are presented in order of decreasing seriousness. (See Table 19.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form