


 Sign Out
Sign Out
Cefixime exerts its bactericidal activity by interfering with the synthesis of the bacterial cell wall. It binds to specific penicillin-binding proteins responsible for the synthesis of peptidoglycan, a heteropolymeric structure that gives the cell wall its mechanical stability. The final stage of peptidoglycan synthesis involves completion of the cross-linking of the terminal glycine residue of the pentaglycine bridge to the fourth residue of the pentapeptide. The transpeptidase that catalyzes this step is inhibited by cephalosporins. Thus, inhibition of the transpeptidase interrupts peptidoglycan synthesis, causing formation of defective cell walls and osmotically unstable spheroplasts and lysis of the bacteria.
Pharmacokinetics: About 30% to 50% of a single oral dose of cefixime is absorbed. Food decreases the rate but generally does not affect the extent of drug absorption. When cefixime oral suspension at a single dose of 4, 6, or 8 mg/kg body weight was administered to children 6 months to 6 years old or older, mean serum concentrations (Cmax) attained 3.5 to 4.5 hours after the dose were 2.18 to 2.44, 3.55 to 4.07, and 3.4 to 3.91 μg/mL, respectively. Serum concentrations of cefixime are not directly dose proportional at doses of 4 to 8 mg/kg body weight in children. Little or no accumulation of cefixime occurs after multiple dosing.
After oral administration, cefixime is distributed into bile, sputum, tonsils, maxillary sinus mucosa, middle ear discharge, blister fluid, and prostatic fluid. Sputum concentrations may be 2% to 10% of concurrent serum concentrations; in one study, a single 200 mg oral dose of cefixime resulted in sputum concentrations of 0.03 to 0.12 μg/mL. It is not known whether cefixime is distributed into CSF after oral administration.
In children 3 months to 5 years old with acute otitis media with effusion or with otitis media with effusion that required tympanostomy tube placement, a single 8 mg/kg body weight oral dose of cefixime resulted in middle ear fluid mean concentrations averaging 1.3 to 1.4 mg/mL at 3 to 5 hours after the dose; concurrent Cmax were 2.5 to 3.2 pg/mL.
About 65% to 75% of cefixime is bound to serum proteins, principally albumin, and such binding is not concentration-dependent over the range of 0.5 to 30 μg/mL. The fraction of free cefixime in plasma may be slightly greater in patients with renal impairment than in those with normal renal function.
Cefixime crosses the placenta and is distributed in low concentrations into amniotic fluid and cord serum; cord serum concentrations may be 15% to 50% of concurrent maternal plasma concentrations. No data are available on secretion of cefixime into human milk.
The half-life (t½) of cefixime is about 3 to 4 hours and is not dose-dependent. It is excreted renally via glomerular filtration and to a lesser extent by tubular secretion. Metabolites of cefixime have not been isolated from human serum or urine. About 7% to 41% of a single oral dose of the drug is excreted unchanged in urine within 24 hours. The remainder of the dose (up to 60%) is eliminated by nonrenal mechanism. In animal studies, it was noted that up to 10% of a single oral dose of cefixime is excreted unchanged in bile.
Cefixime is not removed to a significant degree by either hemodialysis or peritoneal dialysis.
Microbiology: Antimicrobial Spectrum of Activity: Cefixime is active against the following organisms, both in vitro and in clinical infections: See Table 1.
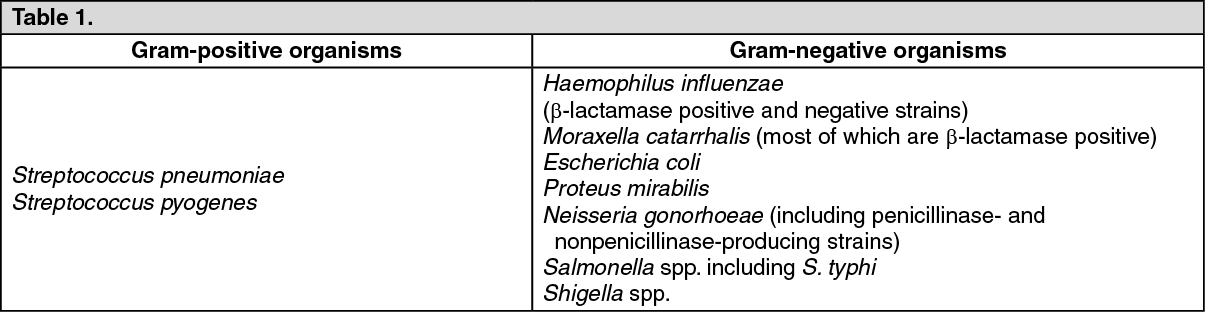 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageCefixime has been shown to be active in vitro against most strains of Gram-positive organisms such as Streptococcus agalactiae and most strains of Gram-negative organisms such as Haemophilus parainfluenzae (β-lactamase positive and negative strains), Neisseria meningitidis, Proteus vulgaris, Klebsiella pneumoniae, Klebsiella oxytoca, Pasteurella multocida, Providencia spp, Bordetella pertussis, Citrobacter freundii, Citrobacter amalonaticus, Citrobacter diversus, Helicobacter pylori and Serratia marcescens; however, clinical efficacy has not been established.
Pseudomonas spp, strains of group D streptococci (including enterococci), Listeria monocytogenes, most strains of staphylococci (including methicillin-resistant strains) and most strains of Enterobacter are resistant to cefixime. In addition, most strains of Bacteroides fragilis and Clostridia are resistant to cefixime.