


 Sign Out
Sign Out
Pharmacology: Pharmacodynamics: Antivirals for systemic use.
Mechanism of action: Valaciclovir, an antiviral, is the L-valine ester of aciclovir. Aciclovir is a purine (guanine) nucleoside analogue.
Valaciclovir is rapidly and almost completely converted in man to aciclovir and valine, probably by the enzyme referred to as valaciclovir hydrolase.
Aciclovir is a specific inhibitor of the herpes viruses with in vitro activity against herpes simplex viruses (HSV) type 1 and type 2, varicella zoster virus (VZV), cytomegalovirus (CMV), Epstein-Barr Virus (EBV), and human herpes virus 6 (HHV-6). Aciclovir inhibits herpes virus DNA synthesis once it has been phosphorylated to the active triphosphate form.
The first stage of phosphorylation requires the activity of a virus-specific enzyme. In the case of HSV, VZV and EBV this enzyme is the viral thymidine kinase (TK), which is only present in virus-infected cells. Selectivity is maintained in CMV with phosphorylation, at least in part, being mediated through the phosphotransferase gene product of UL97. This requirement for activation of aciclovir by a virus-specific enzyme largely explains its selectivity.
The phosphorylation process is completed (conversion from mono- to triphosphate) by cellular kinases. Aciclovir triphosphate competitively inhibits the virus DNA polymerase and incorporation of this nucleoside analogue results in obligate chain termination, halting virus DNA synthesis and thus blocking virus replication.
Pharmacodynamic effects: Resistance to aciclovir is normally due to a thymidine kinase deficient phenotype which results in a virus which is disadvantaged in the natural host. Reduced sensitivity to aciclovir has been described as a result of subtle alterations in either the virus thymidine kinase or DNA polymerase. The virulence of these variants resembles that of the wild-type virus.
Monitoring of clinical HSV and VZV isolates from patients receiving aciclovir therapy or prophylaxis has revealed that virus with reduced sensitivity to aciclovir is extremely rare in the immunocompetent host and is found infrequently in severely immunocompromised individuals e.g. organ or bone marrow transplant recipients, patients receiving chemotherapy for malignant disease and people infected with the human immunodeficiency virus (HIV).
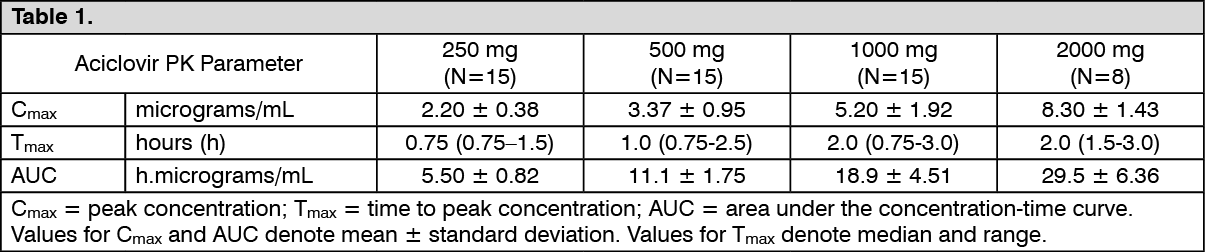
Pharmacokinetics: Absorption: Valaciclovir is a prodrug of aciclovir. The bioavailability of aciclovir from valaciclovir is about 3.3 to 5.5-fold greater than that historically observed for oral aciclovir. After oral administration valaciclovir is well absorbed and rapidly and almost completely converted to aciclovir and valine. This conversion is probably mediated by an enzyme isolated from human liver referred to as valaciclovir hydrolase. The bioavailability of aciclovir from 1000 mg valaciclovir is 54%, and is not reduced by food. Valaciclovir pharmacokinetics is not dose-proportional. The rate and extent of absorption decreases with increasing dose, resulting in a less than proportional increase in Cmax over the therapeutic dose range and a reduced bioavailability at doses above 500 mg. Aciclovir pharmacokinetic (PK) parameter estimates following single doses of 250 to 2000 mg valaciclovir to healthy subjects with normal renal function are shown as follows. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePeak plasma concentrations of unchanged valaciclovir are only about 4% of peak aciclovir levels, occur at a median time of 30 to 100 min post-dose, and are at or below the limit of quantification 3 h after dosing. The valaciclovir and aciclovir pharmacokinetic profiles are similar after single and repeat dosing. Herpes zoster, herpes simplex and HIV infection do not significantly alter the pharmacokinetics of valaciclovir and aciclovir after oral administration of valaciclovir compared with healthy adults. In transplant recipients receiving valaciclovir 2000 mg 4 times daily, aciclovir peak concentrations are similar to or greater than those in healthy volunteers receiving the same dose. The estimated daily AUCs are appreciably greater.
Distribution: Binding of valaciclovir to plasma proteins is very low (15%). CSF penetration, determined by CSF/plasma AUC ratio, is independent of renal function and was about 25% for aciclovir and the metabolite 8-OH-ACV, and about 2.5% for the metabolite CMMG.
Biotransformation: After oral administration, valaciclovir is converted to aciclovir and L-valine by first-pass intestinal and/or hepatic metabolism. Aciclovir is converted to a small extent to the metabolites 9(carboxymethoxy) methylguanine (CMMG) by alcohol and aldehyde dehydrogenase and to 8-hydroxy-aciclovir (8-OH-ACV) by aldehyde oxidase. Approximately 88% of the total combined plasma exposure is attributable to aciclovir, 11% to CMMG and 1% to 8-OH-ACV. Neither valaciclovir nor aciclovir is metabolized by cytochrome P450 enzymes.
Elimination: Valaciclovir is eliminated in the urine principally as aciclovir (greater than 80% of the recovered dose) and the aciclovir metabolite CMMG (about 14% of the recovered dose). The metabolite 8-OH-ACV is detected only in small amounts in urine (< 2% of the recovered dose). Less than 1% of the administered dose of valaciclovir is recovered in the urine as unchanged drug. In patients with normal renal function the plasma elimination half-life of aciclovir after both single and multiple dosing with valaciclovir is approximately 3 h.