Adults: Herpes Zoster (Shingles) Including Ophthalmic Zoster: 1000 mg to be taken 3 times daily for 7 days.
Herpes Simplex Infections: Immunocompetent Adults and Adolescents ≥12 years: 500 mg to be taken twice daily.
For recurrent episodes, treatment should be for 3 or 5 days. For initial episodes, which can be more severe, treatment may have to be extended from 5-10 days. Dosing should begin as early as possible. For recurrent episodes of herpes simplex, this should ideally be during the prodromal period or immediately when the 1st signs or symptoms appear. Valtrex can prevent lesion development when taken at the 1st signs and symptoms of an HSV recurrence.
Alternatively, for herpes labialis (cold sores), Valtrex 2 g twice daily for 1 day is an effective treatment. The 2nd dose should be taken about 12 hrs (no sooner than 6 hrs) after the 1st dose. When using this dosing regimen, treatment should not exceed 1 day since this has been shown not to provide additional clinical benefit. Therapy should be initiated at the earliest symptom of a cold sore (eg, tingling, itching or burning).
Prevention (Suppression) of Recurrences of Herpes Simplex Infections: Immunocompetent Adults and Adolescents ≥12 years: In immunocompetent patients, 500 mg to be taken once daily.
Some patient with very frequent recurrences (eg, ≥10 recurrences/year) may gain additional benefit from the daily dose of 500 mg being taken as a divided dose (250 mg twice daily).
Immunocompromised Adults: For immunocompromised patients, the dose is 500 mg twice daily.
Reduction of Transmission of Genital Herpes: In immunocompetent heterosexual adults with ≤9 recurrences/year, Valtrex 500 mg to be taken once daily by the infected partner.
There are no data on the reduction of transmission in other patient populations.
Prophylaxis of Cytomegalovirus Infection and Disease: The dosage of Valtrex in adults and adolescents (from 12 years) is 2 g 4 times daily to be initiated as early as possible post-transplant. This dose should be reduced according to CrCl (see Renal Impairment as follows).
The duration of treatment will usually be 90 days but may need to be extended in high risk patients.
Elderly: The possibility of renal impairment in the elderly must be considered and the dosage should be adjusted accordingly (see Renal Impairment as follows).
Adequate hydration should be maintained.
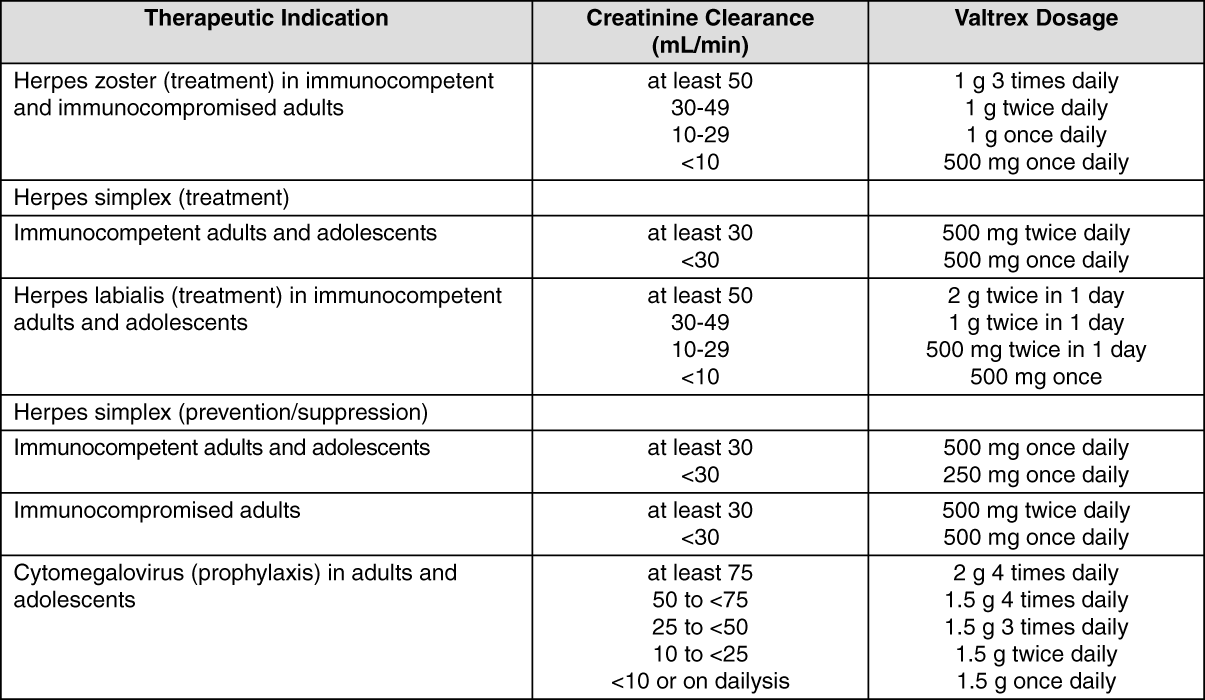
Renal Impairment: Caution is advised when administering valaciclovir to patients with impaired renal function. Adequate hydration should be maintained.
The dosage of Valtrex should be reduced in patients with significantly impaired renal function as shown in the table as follows: See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In patients on intermittent hemodialysis, the Valtrex dosage recommended for patients with a CrCl <15 mL/min should be used. This should be administered after the hemodialysis has been performed.
The CrCl should be monitored frequently, especially during periods when renal function is changing rapidly eg, immediately after transplantation or engraftment. The Valtrex dosage should be adjusted accordingly.
Hepatic Impairment: Studies with Valtrex 1 g unit dose show that dose modification is not required in patients with mild or moderate cirrhosis (hepatic synthetic function maintained). Pharmacokinetic data in patients with advanced cirrhosis (impaired hepatic synthetic function and evidence of portal-systemic shunting) do not indicate the need for dosage adjustment; however, clinical experience is limited. For higher doses, (≥4 g/day), see Precautions.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out