Pharmacotherapeutic group: nucleosides and nucleotides excl. reverse transcriptase inhibitors.
ATC code: J05A B14.
Pharmacology: Pharmacodynamics: Mechanism of action: Valganciclovir is an L-valyl ester (prodrug) of ganciclovir. After oral administration, valganciclovir is rapidly and extensively metabolised to ganciclovir by intestinal and hepatic esterases. Ganciclovir is a synthetic analogue of 2'-deoxyguanosine and inhibits replication of herpes viruses in vitro and in vivo. Sensitive human viruses include human cytomegalovirus (HCMV), herpes simplex virus-1 and -2 (HSV-1 and HSV-2), human herpes virus -6, -7 and -8 (HHV-6, HHV-7, HHV8), Epstein-Barr virus (EBV), varicella-zoster virus (VZV) and hepatitis B virus (HBV).
In CMV-infected cells, ganciclovir is initially phosphorylated to ganciclovir monophosphate by the viral protein kinase, pUL97. Further phosphorylation occurs by cellular kinases to produce ganciclovir triphosphate, which is then slowly metabolised intracellularly. Triphosphate metabolism has been shown to occur in HSV- and HCMV-infected cells with half-lives of 18 and between 6 and 24 hours respectively, after the removal of extracellular ganciclovir. As the phosphorylation is largely dependent on the viral kinase, phosphorylation of ganciclovir occurs preferentially in virus-infected cells.
The virustatic activity of ganciclovir is due to inhibition of viral DNA synthesis by: (a) competitive inhibition of incorporation of deoxyguanosine-triphosphate into DNA by viral DNA polymerase, and (b) incorporation of ganciclovir triphosphate into viral DNA causing termination of, or very limited, further viral DNA elongation.
Antiviral activity: The in-vitro anti-viral activity, measured as IC50 of ganciclovir against CMV, is in the range of 0.08 µM (0.02 µg/ml) to 14 µM (3.5 µg/ml).
The clinical antiviral effect of Valganciclovir has been demonstrated in the treatment of AIDS patients with newly diagnosed CMV retinitis. CMV shedding was decreased in urine from 46 % (32/69) of patients at study entry to 7 % (4/55) of patients following four weeks of Valganciclovir treatment.
Clinical efficacy and safety: Treatment of CMV retinitis: Patients with newly diagnosed CMV retinitis were randomised in one study to induction therapy with either Valganciclovir 900 mg b.i.d or intravenous ganciclovir 5 mg/kg b.i.d. The proportion of patients with photographic progression of CMV retinitis at week 4 was comparable in both treatment groups, 7/70 and 7/71 patients progressing in the intravenous ganciclovir and valganciclovir arms respectively.
Following induction treatment dosing, all patients in this study received maintenance treatment with Valganciclovir given at the dose of 900 mg once daily. The mean (median) time from randomisation to progression of CMV retinitis in the group receiving induction and maintenance treatment with Valganciclovir was 226 (160) days and in the group receiving induction treatment with intravenous ganciclovir and maintenance treatment with Valganciclovir was 219 (125) days.
Prevention of CMV disease in transplantation: A double-blind, double-dummy, clinical active comparator study has been conducted in heart, liver and kidney transplant patients (lung and gastro-intestinal transplant patients were not included in the study) at high-risk of CMV disease (D+/R-) who received either Valganciclovir (900 mg od) or oral ganciclovir (1000 mg t.i.d.) starting within 10 days of transplantation until Day 100 post-transplant. The incidence of CMV disease (CMV syndrome + tissue invasive disease) during the first 6 months post-transplant was 12.1 % in the Valganciclovir arm (n=239) compared with 15.2 % in the oral ganciclovir arm (n=125). The large majority of cases occurred following cessation of prophylaxis (post-Day 100) with cases in the valganciclovir arm occurring on average later than those in the oral ganciclovir arm. The incidence of acute rejection in the first 6 months was 29.7 % in patients randomised to valganciclovir compared with 36.0 % in the oral ganciclovir arm, with the incidence of graft loss being equivalent, occurring in 0.8 % of patients, in each arm.
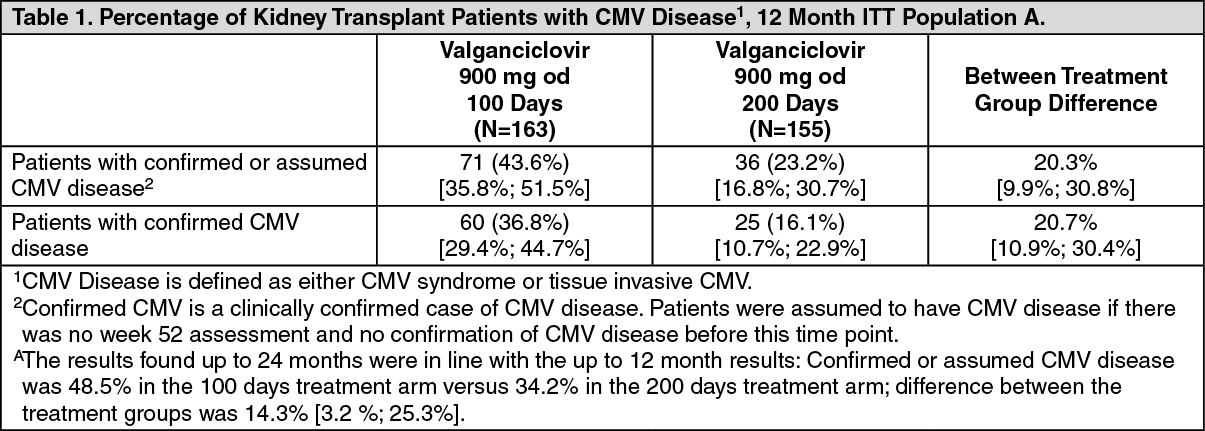
A double-blind, placebo controlled study has been conducted in 326 kidney transplant patients at high risk of CMV disease (D+/R-) to assess the efficacy and safety of extending Valganciclovir CMV prophylaxis from 100 to 200 days post-transplant. Patients were randomized (1:1) to receive Valganciclovir tablets (900 mg od) within 10 days of transplantation either until Day 200 post-transplant or until Day 100 post-transplant followed by 100 days of placebo.
The proportion of patients who developed CMV disease during the first 12 months post-transplant is shown in the table as follows. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Significantly less high risk kidney transplant patients developed CMV disease following CMV prophylaxis with Valganciclovir until Day 200 post-transplant compared to patients who received CMV prophylaxis with Valganciclovir until Day 100 post-transplant.
The graft survival rate as well as the incidence of biopsy proven acute rejection was similar in both treatment groups. The graft survival rate at 12 months post-transplant was 98.2 % (160/163) for the 100 day dosing regimen and 98.1 % (152/155) for the 200 day dosing regimen. Up to 24 month post-transplant, four additional cases of graft loss were reported, all in the 100 days dosing group. The incidence of biopsy proven acute rejection at 12 months post-transplant was 17.2% (28/163) for the 100 day dosing regimen and 11.0% (17/155) for the 200 day dosing regimen. Up to 24 month post-transplant, one additional case has been reported in the 200 days dosing group.
Viral resistance: Virus resistant to ganciclovir can arise after chronic dosing with valganciclovir by selection of mutations in the viral kinase gene (UL97) responsible for ganciclovir monophosphorylation and/or the viral polymerase gene (UL54). Viruses containing mutations in the UL97 gene are resistant to ganciclovir alone, whereas viruses with mutations in the UL54 gene are resistant to ganciclovir but may show cross-resistance to other antivirals that also target the viral polymerase.
Treatment of CMV retinitis: Genotypic analysis of CMV in polymorphonuclear leucocytes (PMNL) isolates from 148 patients with CMV retinitis enrolled in one clinical study has shown that 2.2%, 6.5%, 12.8 %, and 15.3% contain UL97 mutations after 3, 6, 12 and 18 months, respectively, of valganciclovir treatment.
Prevention of CMV disease in transplantation: Active comparator study: Resistance was studied by genotypic analysis of CMV in PMNL samples collected) on Day 100 (end of study drug prophylaxis) and ii) in cases of suspected CMV disease up to 6 months after transplantation. From the 245 patients randomised to receive valganciclovir, 198 Day 100 samples were available for testing and no ganciclovir resistance mutations were observed. This compares with 2 ganciclovir resistance mutations detected in the 103 samples tested (1.9 %) for patients in the oral ganciclovir comparator arm. Of the 245 patients randomised to receive valganciclovir, samples from 50 patients with suspected CMV disease were tested and no resistance mutations were observed. Of the 127 patients randomised on the ganciclovir comparator arm, samples from 29 patients with suspected CMV disease were tested, from which two resistance mutations were observed, giving an incidence of resistance of 6.9%.
Extending prophylaxis study from 100 to 200 days post-transplant: Genotypic analysis was performed on the UL54 and UL97 genes derived from virus extracted from 72 patients who met the resistance analysis criteria: patients who experienced a positive viral load (>600 copies/ml) at the end of prophylaxis and/or patients who had confirmed CMV disease up to 12 months (52 weeks) post-transplant. Three patients in each treatment group had a known ganciclovir resistance mutation.
Paediatric population: A phase II pharmacokinetic and safety study in paediatric solid organ transplant recipients (aged 4 months to 16 years, n = 63) receiving valganciclovir once daily for up to 100 days according to a dosing algorithm produced exposures similar to that in adults. Follow up after treatment was 12 weeks. CMV D/R serology status at baseline was D+/R- in 40%, D+/R+ in 38%, D-/R+ in 19% and D-/R- in 3% of the cases. Presence of CMV virus was reported in 7 patients. The observed adverse drug reactions were of similar nature as those in adults. These data are too limited to allow conclusions regarding efficacy or posology recommendations for paediatric patients.
The pharmacokinetics and safety of single dose valganciclovir (dose range 14-16-20 mg/kg/dose) was studied in 24 neonates (aged 8-34 days) with symptomatic congenital CMV disease. The neonates received 6 weeks of antiviral treatment, whereas 19 of the 24 patients received up to 4 weeks of treatment with oral valganciclovir, in the remaining 2 weeks they received i.v. ganciclovir. The 5 remaining patients received i.v. ganciclovir for the most time of the study period. This treatment indication is not recommended presently for valganciclovir. The design of the study and obtained results are too limited to allow appropriate efficacy and safety conclusions on valganciclovir.
Pharmacokinetics: The pharmacokinetic properties of valganciclovir have been evaluated in HIV- and CMV-seropositive patients, patients with AIDS and CMV retinitis and in solid organ transplant patients.
Absorption: Valganciclovir is a prodrug of ganciclovir. It is well absorbed from the gastrointestinal tract and rapidly and extensively metabolised in the intestinal wall and liver to ganciclovir. Systemic exposure to valganciclovir is transient and low. The absolute bioavailability of ganciclovir from valganciclovir is approximately 60% across all the patient populations studied and the resultant exposure to ganciclovir is similar to that after its intravenous administration (please see as follows). For comparison, the bioavailability of ganciclovir after administration of 1000 mg oral ganciclovir (as capsules) is 6-8%.
Valganciclovir in HIV positive, CMV positive patients: Systemic exposure of HIV positive, CMV positive patients after twice daily administration of ganciclovir and valganciclovir for one week is: See Table 2.
Click on icon to see table/diagram/image
The efficacy of ganciclovir in increasing the time-to-progression of CMV retinitis has been shown to correlate with systemic exposure (AUC).
Valganciclovir in solid organ transplant patients: Steady state systemic exposure of solid organ transplant patients to ganciclovir after daily oral administration of ganciclovir and valganciclovir is: See Table 3.
Click on icon to see table/diagram/image
Distribution: Because of rapid conversion of valganciclovir to ganciclovir, protein binding of valganciclovir was not determined. Plasma protein binding of ganciclovir was 1-2% over concentrations of 0.5 and 51 g/ml. The steady state volume of distribution (Vd) of ganciclovir after intravenous administration was 0.680 ± 0.161 l/kg (n=114).
Biotransformation: Valganciclovir is rapidly and extensively metabolised to ganciclovir; no other metabolites have been detected. No metabolite of orally administered radiolabelled ganciclovir (1000 mg single dose) accounted for more than 1-2% of the radioactivity recovered in the faeces or urine.
Elimination: Following dosing with Valganciclovir, renal excretion, as ganciclovir, by glomerular filtration and active tubular secretion is the major route of elimination of valganciclovir. Renal clearance accounts for 81.5 % ± 22 % (n=70) of the systemic clearance of ganciclovir. The half-life of ganciclovir from valganciclovir is 4.1 ± 0.9 hours in HIV- and CMV-seropositive patients.
Pharmacokinetics in special clinical situations: Patients with renal impairment: Decreasing renal function resulted in decreased clearance of ganciclovir from valganciclovir with a corresponding increase in terminal half-life. Therefore, dosage adjustment is required for renally impaired patients.
Patients undergoing haemodialysis: For patients receiving haemodialysis dose recommendations for Valganciclovir 450 mg film-coated tablets cannot be given. This is because an individual dose of Valganciclovir required for these patients is less than the 450 mg tablet strength. Thus, Valganciclovir film-coated tablets should not be used in these patients.
Patients with hepatic impairment: The safety and efficacy of Valganciclovir film-coated tablets have not been studied in patients with hepatic impairment. Hepatic impairment should not affect the pharmacokinetics of ganciclovir since it is excreted renally and, therefore, no specific dose recommendation is made.
Paediatric population: In a phase II pharmacokinetic and safety study in paediatric solid organ transplant recipients (aged 4 months to 16 years, n = 63) valganciclovir was given once daily for up to 100 days. Pharmacokinetics parameters were similar across organ type and age range and comparable with adults. Population pharmacokinetic modeling suggested that bioavailability was approximately 60%. Clearance was positively influenced by both body surface area and renal function. The mean total clearance was 5.3 l/hr (88.3 ml/min) for a patient with creatinine clearance of 70.4 ml/min. The following table shows the mean C
max, t
½ and AUC values including standard deviations for the relevant paediatric age groups compared to adult data: See Table 4.
Click on icon to see table/diagram/image
The once daily dose of Valganciclovir was based on body surface area (BSA) and creatinine clearance (CrCl) derived from a modified Schwartz formula, and was calculated using the equation as follows: See Equation 1.
Click on icon to see table/diagram/image
where k = 0.45 for patients aged <2 years, 0.55 for boys aged 2 to <13 years and girls aged 2 to 16 years, and 0.7 for boys aged 13 to 16 years.
The dose should not exceed the adult 900 mg dose. In addition, if the calculated Schwartz creatinine clearance exceeds 150 ml/min/1.73m
2, then a maximum value of 150 ml/min/1.73m
2 should be used in the equation. It should be noted that the paediatric dosage algorithm was developed based on pharmacokinetic data only and has not been verified in efficacy and safety studies.
Ganciclovir pharmacokinetics were also evaluated in 24 neonates aged 8 to 34 days with symptomatic congenital CMV disease. All patients received 6 mg/kg intravenous ganciclovir twice daily. Patients were then treated with oral valganciclovir, where the dose of valganciclovir powder for oral solution ranged from 14 mg/kg to 20 mg/kg twice daily. A dose of 16 mg/kg twice daily of valganciclovir powder for oral solution provided comparable ganciclovir exposure as 6 mg/kg intravenous ganciclovir twice daily in neonates, and also achieved ganciclovir exposure similar to the effective adult 5 mg/kg intravenous dose. The following table shows the mean AUC, C
max, and t
½ values including standard deviations compared adult data: See Table 5.
Click on icon to see table/diagram/image
The pharmacokinetic modeling suggested that the typical value of clearance (l/hr), volume of distribution (l), and bioavailability of ganciclovir in neonates were 0.146 x Weight 1.68, 1.15 x Weight, and 54%, respectively. These data are too limited to allow conclusions regarding efficacy or posology recommendations for paediatric patients with congenital CMV infection.
Toxicology: Preclinical safety data: Valganciclovir is a pro-drug of ganciclovir and therefore effects observed with ganciclovir apply equally to valganciclovir. Toxicity of valganciclovir in pre-clinical safety studies was the same as that seen with ganciclovir and was induced at ganciclovir exposure levels comparable to, or lower than, those in humans given the induction dose.
These findings were gonadotoxicity (testicular cell loss) and nephrotoxicity (uraemia, cell degeneration), which were irreversible; myelotoxicity (anaemia, neutropenia, lymphocytopenia) and gastrointestinal toxicity (mucosal cell necrosis), which were reversible.
Further studies have shown ganciclovir to be mutagenic, carcinogenic, teratogenic, embryotoxic, aspermatogenic (i.e. impairs male fertility) and to suppress female fertility.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image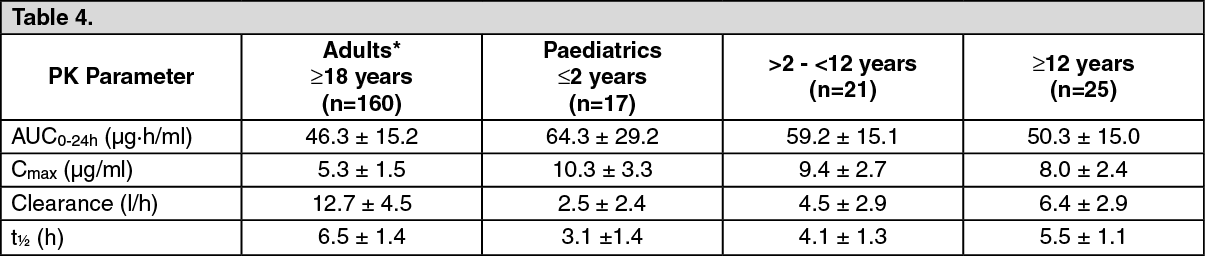 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image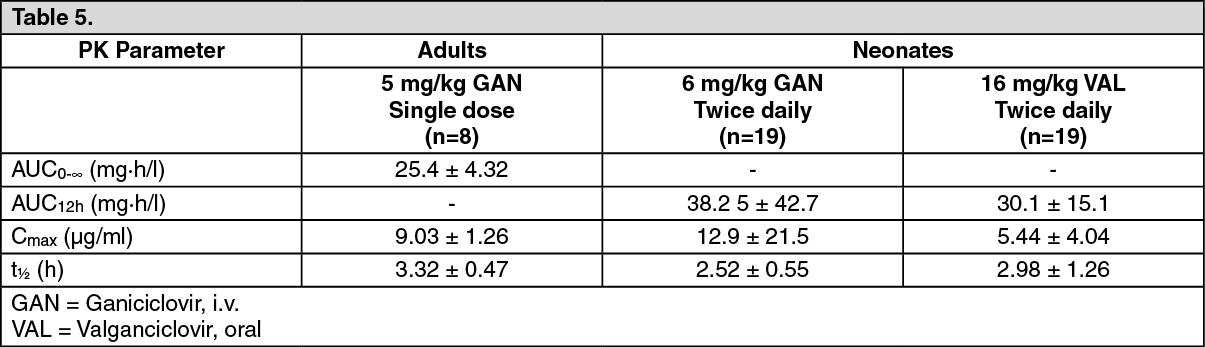 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image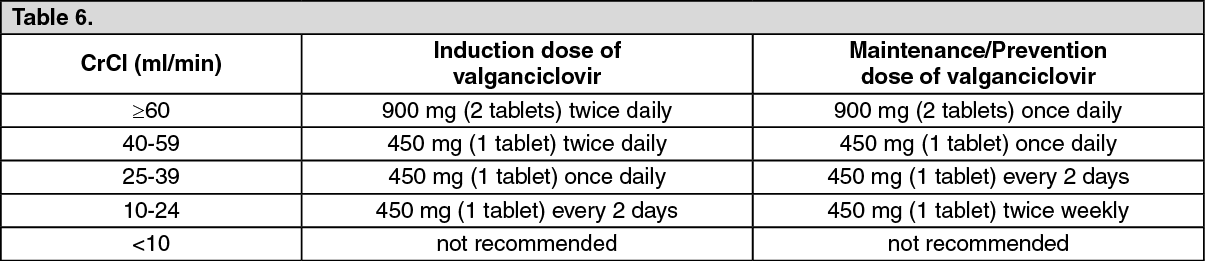 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image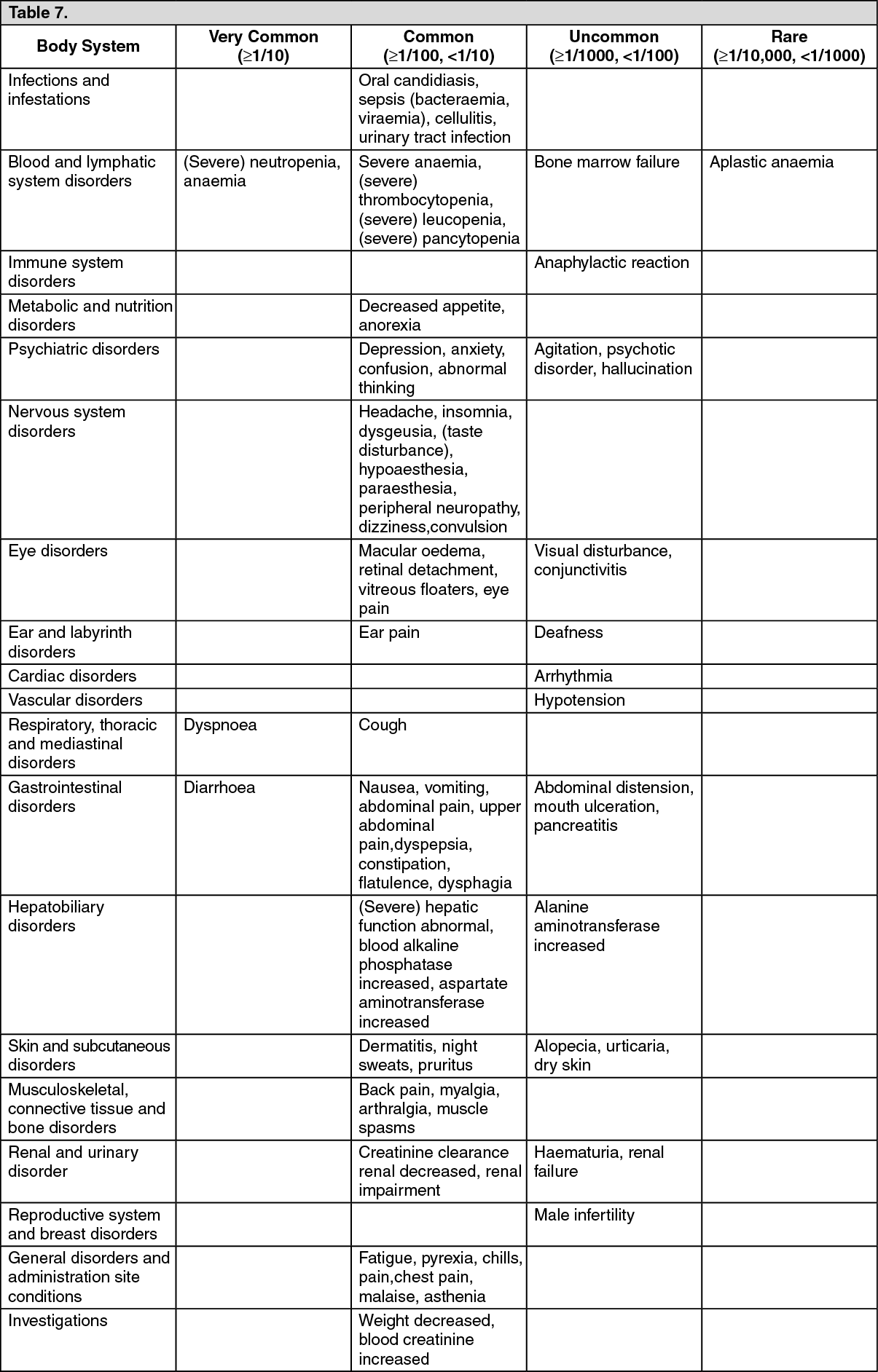 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image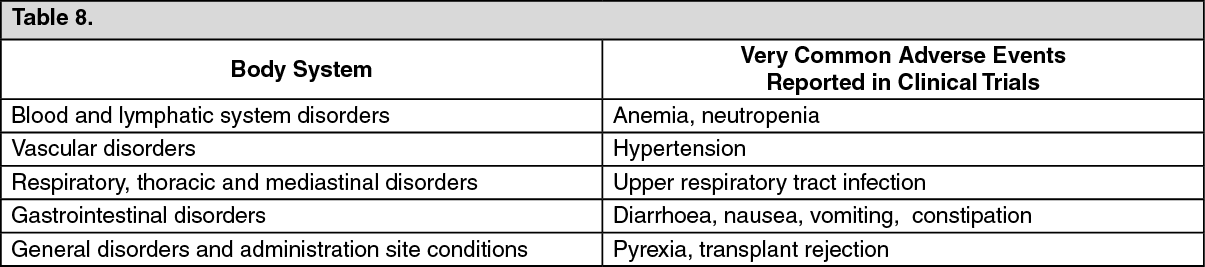 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out