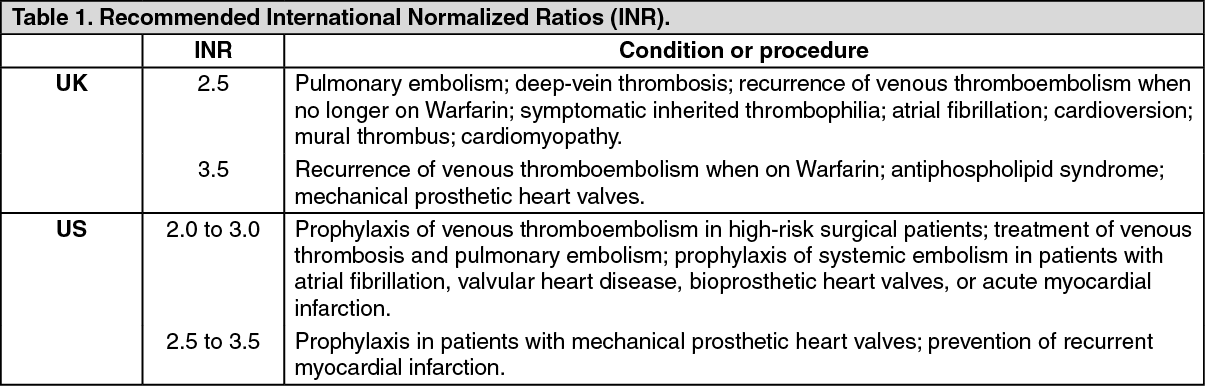
See Tables 2 and 3.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The major interactions are summarized in the Tables 2 and 3. Readers should be aware that while interactions of a pharmacodynamic nature occurring with one anticoagulant may well apply to another, this is not necessarily the case with interactions of a pharmacokinetic nature.
An interaction may be due to increased or decreased anticoagulant metabolism; with Warfarin some interacting drugs such as cimetidine, co-trimoxazole, or phenylbutazone have a selective effect on its stereoisomers. Altered absorption may sometimes play a part, as with colestyramine. Displacement of oral anticoagulants from plasma protein binding sites has been reported with many drugs, including some analgesics. Interference with the coagulation process may be responsible for the increased risk of hemorrhage when aspirin, clofibrate, or thyroid hormones are used with anticoagulants. Many other compounds, such as asparaginase, some contrast media, epoprostenol, streptokinase, and urokinase also carry this risk; while interactions between these compounds and anticoagulants are not discussed further as follows, the possibility of an increased risk of hemorrhage should be considered when they are used together.
Where there is a risk of serious hemorrhage from an interaction, then use of the 2 drugs is best avoided. In other instances the anticoagulant activity should be carefully monitored so as to increase or decrease the anticoagulant dose as required. Critical periods are when patients stabilized on an anticoagulant commence treatment with an interacting drug, or when patients stabilized on a regimen of an interacting drug and anticoagulant have the interacting drug withdrawn. Depending on the mechanism of the interaction, the clinical response to the interaction may be rapid or may take some days. Interactions involving displacement from plasma protein binding sites are often transient. Readers should also be aware that some interacting drugs do not produce predictable effects; there have for instance been reports of increased as well as decreased anticoagulant activity with disopyramide, phenytoin, quinidine, and oral contraceptives. Another problem occurs with dipyridamole; it can cause bleeding when given to patients taking anticoagulants but without any changes in the measures used for anticoagulant control.
Alcohol: Alcohol has a variable effect on Warfarin. Heavy regular drinkers may experience a diminished effect, perhaps through enzyme induction, although the effect of Warfarin may be increased in the presence of liver impairment; acute ingestion has enhanced the effect of Warfarin. A moderate alcohol intake is generally not considered to cause problems.
Analgesics and NSAIDs: All NSAIDs should be used with caution or not at all in patients on Warfarin. Many NSAIDs inhibit platelet function to some extent and have an irritant effect on the gastrointestinal tract, so increasing the risk of hemorrhage. Furthermore, some NSAIDs increase the hypoprothrombinemic effect of Warfarin, possibly by an intrinsic effect on coagulation or by displacement of Warfarin from plasma protein binding site. Changes in plasma concentration of unbound Warfarin resulting from displacement from plasma protein-binding sites are usually transient and are most likely to occur in the first few weeks after an NSAID is added to or withdrawn from Warfarin therapy.
High doses of aspirin and some other salicylates enhance the hypoprothrombinemic effect of Warfarin and should generally be avoided in patients on oral anticoagulant therapy. Low-dose aspirin with Warfarin may have a role in some patients but the risk of gastrointestinal bleeding is increased. The possibility of an interaction with topical salicylates should also be considered.
Concurrent administration of phenylbutazone and Warfarin has led to serious hemorrhage and should be avoided. Phenylbutazone affects the metabolism of the
R- and
S-isomers of Warfarin in complex and different ways with the net effect of enhancing its anticoagulant activity. Related drugs such as oxyphenbutazone, azapropazone, and feprazone behave similarly and should also be avoided.
For the following NSAIDs there are few isolated reports suggesting that they may enhance the hypoprothrombinemic effect of Warfarin or other specified oral anticoagulant: diflunisal (with nicoumalone or Warfarin), flurbiprofen (with nicoumalone), indomethacin, ketoprofen, meclofenamate sodium, mefenamic acid, piroxicam, (with Warfarin or nicoumalone), sulindac, tiaprofenic acid (with nicoumalone), and tolmetin sodium. NSAIDs with an apparently minimal effect on Warfarin activity include etodolac, ibuprofen, and naproxen.
In view of the previous considerations, paracetamol is recommended as the general analgesic and antipyretic of choice in patients on oral anticoagulant therapy. Caution should, however, be observed since, although it has no effect on the gastric mucosa or on platelet function, and isolated reports have demonstrated an increased risk of bleeding in patients taking regular doses of paracetamol while on an oral anticoagulant.
Although a study in healthy volunteers indicated that there was no interaction between Warfarin and celecoxib, a selective inhibitor of cyclo-oxygenase-2, there have been several reports of an increase in the INR with concomitant therapy; bleeding has also been reported in some patients. A small increase in INR has also been reported in a study of Warfarin with rofecoxib.
Antiarrhythmics: Amiodarone has been shown in several studies to increase the activity of Warfarin and nicoumalone, probably through inhibition of metabolism. The potentiating effect of amiodarone has been reported to persist for up to 4 months after its withdrawal. Isolated reports with disopyramide and quinidine have suggested that these drugs can enhance the anticoagulant effect of Warfarin.
Antibacterials: Some antibacterials may interfere with platelet function or with the bacterial synthesis of vitamin K in the gastrointestinal tract and thus have an anticoagulant effect of their own.
There are several reports of an enhanced Warfarin response with co-trimoxazole; stereospecific inhibition of Warfarin metabolism is probably responsible. The interaction is generally attributed to the sulfamethoxazole moiety and there are isolated reports suggesting that the activity of Warfarin (or other specified oral anticoagulant) may be enhanced by other sulfonamides including sulfafurazole, sulfamethizole, and sulfaphenazole (with phenindione).
There are several reports of potentiation of the effects of Warfarin by erythromycin or its salts; inhibition of Warfarin metabolism probably occurs. An enhance response to Warfarin has also been reported with azithromycin and with roxithromycin, including reports of spontaneous bleeding with the latter. Clarithromycin may potentiate the effect of nicoumalone and of Warfarin, although other factors may also have been involved in this case.
There have been few reports of increased activity of Warfarin (or other specified oral anticoagulant) by quinolone antibacterials including nalidixic acid (with Warfarin or nicoumalone), ciprofloxacin, norfloxacin, and ofloxacin.
There are isolated reports suggesting an enhanced effect of Warfarin (or other specified oral anticoagulant) with aminosalicylic acid, benzylpenicillin, chloramphenicol (with dicoumarol), doxycycline, isoniazid, and neomycin. Manufacturer's warnings of potentiation of Warfarin by aztreonam, trimethoprim, and tetracyclines.
Rifampicin diminishes the effect of Warfarin by induction of metabolizing enzymes in the liver. There are several reports of a similar effect with nafcillin and dicloxacillin sodium.
Antidepressants: Amitriptyline and nortriptyline prolong the half-life of dicoumarol.
There is a theoretical risk of increased Warfarin activity with MAOIs and with fluvoxamine and other SSRIs.
Increased Warfarin activity has been reported in a few patients taking fluoxetine.
An increase in the dose of Warfarin has been required by patients also taking trazodone.
Antidiabetics: An absence of effect has been documented for phenprocoumon and insulin, glibenclamide, or glibornuride, but there is a report of glibenclamide enhancing the effect of Warfarin.
There has been an isolated report of bleeding in a patient taking phenformin and Warfarin.
An enhanced response to Warfarin has been reported in a patient receiving troglitazone.
Antiepileptics: Barbiturates such as phenobarbital and primidone diminish the activity of Warfarin and other coumarins through increased metabolism. Carbamazepine is reported to have a similar effect. There are reports of phenytoin enhancing the effects of Warfarin and a report of initial enhancement followed by decreased anticoagulant action.
Antifungals: Griseofulvin has been reported to diminish the activity of Warfarin. There are several reports indicating that miconazole, given either systemically or topically as the oral gel, may enhance the activity of oral anticoagulants. There are isolated reports of the potentiation of Warfarin by itraconazole and ketoconazole. There has been a case report of a reduction in the effect of Warfarin by terbinafine.
Antigout drugs: Benziodarone has been reported to enhance the effects of Warfarin.
Antimalarials: The ingestion of large amounts of tonic water by 2 patients necessitated a reduction in their Warfarin dosage. The enhanced effect was attributed to the quinine content of the tonic water.
Antineoplastics and immunosuppressants: Cyclophosphamide for instance has been associated with an increase in Warfarin's activity when given with methotrexate and fluorouracil but with a decrease when given with non-antineoplastic drugs. Fluorouracil has also been reported to increase the effect of Warfarin when given with levamisole. The manufacturers of capecitabine state that altered coagulation parameters and bleeding have been reported in patients taking capecitabine and Warfarin or phenprocoumon.
Aminoglutethimide has led to decreased activity of Warfarin or nicoumalone, probably due to increased Warfarin metabolism. The manufacturers of the anti-androgen flutamide state that increases in prothrombin time have been reported after initiation of flutamide therapy in patients on long-term Warfarin. Mercaptopurine and mitotane have also decreased Warfarin activity. Severe bleeding occurred in a patient on long-term Warfarin treatment after discontinuing azathioprine.
Antiplatelets: The interaction between anticoagulants and dipyridamole is an oddity in that bleeding can occur without any alteration in prothrombin times; special care is therefore required as the usual method of monitoring the anticoagulant effect is of no value. This interaction has involved a small number of patients taking dipyridamole and Warfarin or phenindione; inhibition of platelet function by dipyridamole has been implicated. However, in general it does not appear to increase the risk of bleeding.
Antiprotozoals: Metronidazole enhances the activity of Warfarin through selective inhibition of the metabolism of its S-isomer.
Antivirals: Reductions in dosage of either Warfarin or nicoumalone were necessary. The interactions may have been due to decreased metabolism of the anticoagulant. A similar need for a reduced Warfarin dose has also been noted in other patients taking interferon alfa-2b or interferon beta.
An enhanced response to Warfarin has been reported in a patient taking saquinavir concomitantly. The mechanism may involve competitive inhibition of Warfarin metabolism and might also occur with other HIV-protease inhibitors. However, a decreased response to Warfarin seemed to be caused by ritonavir when it was added to the multidrug therapy of a patient.
Anxiolytic sedatives, hypnotics, and antipsychotics: Barbiturates, by inducing liver metabolism, can reduce the activity of anticoagulants; glutethimide has a similar action. Chloral hydrate may increase the anticoagulant activity of Warfarin. However, the increase is only transient and is probably the result of displacement of Warfarin from plasma protein binding sites by the metabolite trichloroacetic acid.
Triclofos sodium appears to increase the activity of Warfarin in a similar way.
Reduced anticoagulant activity has been reported with dichloralphenazone, ethchlorvynol (with dicoumarol), and haloperidol (with phenindione).
Betablockers: Possible potentiation of the effects of Warfarin by propranolol has been reported, particularly those with high lipid solubility such as propranolol, may inhibit the metabolism of Warfarin.
Corticosteroids and Corticotropin: There are several reports of corticosteroids or corticotropin either enhancing or diminishing the effects of anticoagulants.
Dermatological drugs: A patient's Warfarin dose had to be increased when he started treatment with etretinate.
Disulfiram: Two reports suggesting that disulfiram enhances the activity of Warfarin. Although inhibition of liver enzymes by disulfiram was considered responsible, a later study suggested that disulfiram acts directly on the liver to increase hypoprothrombinemia.
Diuretics: Tienilic acid produces the most serious interaction enhancing the activity of Warfarin and has led to hemorrhage. Ethacrynic acid has also been reported to enhance the activity of Warfarin.
Chlorthalidone and spironolactone have both been associated with a reduction in Warfarin's activity. It has been suggested that this might be a consequence of the diuresis concentrating the circulating clotting factors.
Gastrointestinal drugs: Bismuth carbonate and magnesium trisilicate for example have been reported to reduce Warfarin's absorption. There have been occasional reports of sucralfate diminishing the effect of Warfarin.
There are several reports indicating that cimetidine can enhance the anticoagulant effect of Warfarin and hemorrhage has occurred. A number of studies show that cimetidine can increase the plasma concentration and half-life of Warfarin and that there is a selective inhibitory effect on the metabolism of its
R-isomer.
There is a case report suggesting that potentiation of Warfarin by ranitidine may occasionally occur.
Pantoprazole appears to have no effect on the pharmacokinetics or pharmacodynamics of Warfarin.
A marked increase in the effect of Warfarin has been reported when cisapride was added in a therapy.
A reduction in the response to Warfarin with development of venous thrombosis has been reported in a patient receiving mesalazine, and in another patient receiving sulfasalazine.
Ginseng: Reduction in the response to Warfarin was reported in a patient after taking a ginseng preparation.
Glucagon: A dose-dependent enhancement of Warfarin's anticoagulant activity has been reported with glucagons.
Hypericum: Hypericum has been reported to reduce the anticoagulant effect of Warfarin.
Leukotriene antagonists: Zafirlukast is reported to decrease the clearance of S-Warfarin. The manufacturers of zafirlukast state that it probably inhibits the cytochrome P450 isoenzyme CYP2C9 which is involved in the metabolism of Warfarin. Patients receiving Warfarin may develop prolongation of the prothrombin time when zafirlukast is added and Warfarin dosage should be adjusted accordingly.
Levamisole: An increased INR has been reported in a patient receiving chronic Warfarin therapy after addition of levamisole and fluorouracil.
Lipid regulating drugs: Clofibrate can enhance the activity of Warfarin, sometimes to the point of hemorrhage. Bezafibrate has been reported to enhance the effect of phenprocoumon and Warfarin, and fenofibrate and gemfibrozil have been reported to enhance the effect of Warfarin.
Hypoprothrombinemia and bleeding has been reported to be the effect of Warfarin when lovastatin is given to patients. An increased response to Warfarin has also been reported in a number of patients receiving fluvastatin concomitantly.
Dextrothyroxine increase the anticoagulant effect of Warfarin sodium.
An opposite effect may occur with colestyramine which has reduced Warfarin's serum concentration and half-life as well as its activity. The mechanisms of this interaction include binding of Warfarin to colestyramine and reduced absorption; the enterohepatic recycling of Warfarin may also be interrupted.
Pesticides: Chlorinated insecticides diminished the activity of Warfarin.
Piracetam: Piracetam caused an increase in prothrombin time in a patient who had been stabilized on Warfarin.
Sex hormones: There have been a number of reports of steroids with anabolic or androgenic properties enhancing the activity of anticoagulants to the point of hemorrhage. Reports have covered oxymetholone enhancing Warfarin and nicoumalone; stanozolol enhancing Warfarin and dicoumarol; danazol enhancing Warfarin.
There has been a report of topically applied testosterone, which does not have a substituent, enhancing Warfarin.
There has also been a report of a single course of levonorgestrel for emergency contraception increasing the effect of Warfarin.
Thyroid and antithyroid drugs: Thyroid compounds do enhance the activity of oral anticoagulants possibly by increased metabolism of clotting factors. Propylthiouracil has been reported to have caused hypoprothrombinemia.
Ubidecarenone: Decreased INR values and reduced effect of Warfarin.
Vaccines: There have been a few reports of increased prothrombin time and bleeding in Warfarin-stabilized patients following influenza vaccination.
Vitamins: There have been reports of acetomenaphthone and phytomenadione reducing anticoagulant activity, or of foods or nutritional preparations containing vitamin K compounds doing the same.
There have also been isolated reports suggesting that vitamin E may enhance the activity of Warfarin.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image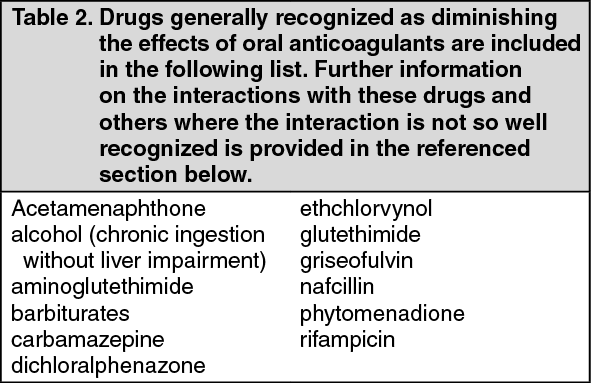 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image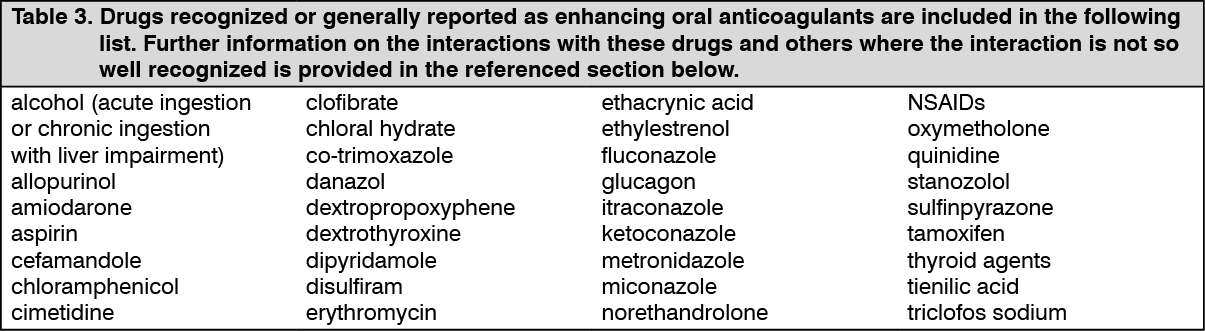 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out