


 Sign Out
Sign Out


ACS: Recommended usual dose: After an acute coronary syndrome, the recommended vascular protection regimen is one tablet of 2.5 mg Rivaroxaban (Xarelto) twice daily. Patients should also take a daily dose of 75-100 mg ASA or a daily dose of 75-100 mg ASA in addition to a daily dose of 75 mg clopidogrel or a standard daily dose of ticlopidine.
ACS: Duration of treatment: Treatment is recommended for at least 24 months.
Patients after ACS continue to be at risk for cardiovascular events and therefore may benefit from extended treatment.
ACS: Method and frequency of administration: Treatment with Rivaroxaban (Xarelto) 2.5 mg should be started as soon as possible after stabilization of the index ACS event (including revascularization procedures). Rivaroxaban (Xarelto) should be started earliest 24 hours after admission to hospital. Rivaroxaban (Xarelto) 2.5 mg should be started at the time when parenteral anticoagulation therapy would normally be discontinued.
One 2.5 mg tablet of Rivaroxaban (Xarelto) should be taken twice daily.
Rivaroxaban (Xarelto) 2.5 mg tablets may be taken with or without food.
For patients who are unable to swallow whole tablets, Rivaroxaban (Xarelto) tablet may be crushed and mixed with water or soft foods such as applesauce immediately prior to use and administered orally.
The crushed Rivaroxaban (Xarelto) tablet may be given through gastric tubes. Gastric placement of the tube should be confirmed before administering Rivaroxaban (Xarelto). The crushed tablet should be administered in a small amount of water via a gastric tube after which it should be flushed with water. (see Pharmacology: Pharmacokinetics under Actions).
ACS: Missed Dose: If a dose is missed the patient should continue with the regular 2.5 mg Rivaroxaban (Xarelto) dose as recommended at the next scheduled time.
CAD or PAD: Method of administration: Oral use.
CAD or PAD: Recommended usual dose: The recommended vascular protection regimen for patients with CAD or PAD is one tablet of 2.5 mg Rivaroxaban (Xarelto) twice daily in combination with a daily dose of 75-100 mg ASA.
CAD or PAD: Duration of treatment: Therapy with Rivaroxaban (Xarelto) should be continued long term provided the benefit outweighs the risk.
In patients with an acute thrombotic event or vascular procedure and a need for dual antiplatelet therapy, the continuation of Rivaroxaban (Xarelto) 2.5 mg twice daily should be evaluated depending on type of event or procedure and antiplatelet regimen. Safety and efficacy of Rivaroxaban (Xarelto) 2.5 mg twice daily in combination with ASA plus clopidogrel/ticlopidine has only been studied in patients with recent ACS. Dual antiplatelet therapy has not been studied in combination with Rivaroxaban (Xarelto) 2.5 mg twice daily in patients with CAD or PAD (see Pharmacology: Pharmacodynamics under Actions).
CAD or PAD: Method and frequency of administration: In patients diagnosed with CAD or PAD, treatment with Rivaroxaban (Xarelto) 2.5 mg twice daily in combination with ASA 75-100 mg once daily can be started at any time.
One 2.5 mg tablet of Rivaroxaban (Xarelto) should be taken twice daily.
Rivaroxaban (Xarelto) 2.5 mg tablets may be taken with or without food.
For patients who are unable to swallow whole tablets, Rivaroxaban (Xarelto) tablet may be crushed and mixed with water or soft foods such as applesauce immediately prior to use and administered orally.
The crushed Rivaroxaban (Xarelto) tablet may be given through gastric tubes. Gastric placement of the tube should be confirmed before administering Rivaroxaban (Xarelto). The crushed tablet should be administered in a small amount of water via a gastric tube after which it should be flushed with water (see Pharmacology: Pharmacokinetics under Actions).
CAD or PAD: Missed Dose: If a dose is missed, the patient should continue with the regular Rivaroxaban (Xarelto) dose as recommended at the next scheduled time.
Additional information on special populations: Patients with hepatic impairment: Rivaroxaban (Xarelto) is contraindicated in patients with hepatic disease which is associated with coagulopathy leading to a clinically relevant bleeding risk (see Contraindications).
No dose adjustment is necessary in patients with other hepatic diseases (see Pharmacology: Pharmacokinetics under Actions).
Limited clinical data in patients with moderate hepatic impairment (Child Pugh B) indicate a significant increase in the pharmacological activity. No clinical data are available for patients with severe hepatic impairment (Child Pugh C) (see Contraindications and Pharmacology: Pharmacokinetics under Actions).
Patients with renal impairment: No dose adjustment is required if Rivaroxaban (Xarelto) is administered in patients with mild (Creatinine clearance (CrC): ≤80-50 mL/min) or moderate (CrC: <50-30 mL/min) renal impairment (see Pharmacology: Pharmacokinetics under Actions).
Limited clinical data for patients with severe renal impairment (CrC: <30-15 mL/min) indicate that rivaroxaban plasma levels are significantly increased in this patient population. Therefore Rivaroxaban (Xarelto) must be used with caution in these patients (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Use of Rivaroxaban (Xarelto) is not recommended in patients with CrC <15 mL/min (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Converting from Vitamin K Antagonists (VKA) to Rivaroxaban (Xareltomisse): When converting patients from VKAs to Rivaroxaban (Xarelto), INR values will be falsely elevated after the intake of Rivaroxaban (Xarelto). The INR is not valid to measure the anticoagulant activity of Rivaroxaban (Xarelto), and therefore should not be used (see Interactions).
Converting from Rivaroxaban (Xarelto) to Vitamin K antagonists (VKA): There is a potential for inadequate anticoagulation during the transition from Rivaroxaban (Xarelto) to VKA. Continuous adequate anticoagulation should be ensured during any transition to an alternate anticoagulant. It should be noted that Rivaroxaban (Xarelto) can contribute to an elevated INR.
In patients converting from Rivaroxaban (Xarelto) to VKA, VKA should be given concurrently until the INR is ≥2.0. For the first two days of the conversion period, standard VKA dosing should be used followed by VKA dosing guided by INR testing. While patients are on both Rivaroxaban (Xarelto) and VKA, the INR should not be tested earlier than 24hours (after the previous dose but prior to the next dose of Rivaroxaban (Xarelto). Once Rivaroxaban (Xarelto) is discontinued INR testing may be done reliably 24 hours after the last dose (see Interactions).
Converting from parenteral anti-coagulants to Rivaroxaban (Xarelto): For patients currently receiving a parenteral anticoagulant, start Rivaroxaban (Xarelto) 0 to 2 hours before the time of the next scheduled administration of the parenteral drug (e.g. LMWH) or at the time of discontinuation of a continuously administered parenteral drug (e.g. intravenous unfractionated heparin).
Converting from Rivaroxaban (Xarelto) to parenteral anti-coagulants: Discontinue Rivaroxaban (Xarelto) and give the first dose of parenteral anticoagulant at the time that the next Rivaroxaban (Xarelto) dose would be taken.
Children and adolescents (from birth to 16 or 18 years depending on local law): Safety and efficacy have not been established in children and adolescents below 18 years.
Geriatric patients: No dose adjustment is required based on age (see Pharmacology: Pharmacokinetics under Actions).
Gender: No dose adjustment is required based on gender (see Pharmacology: Pharmacokinetics under Actions).
Body weight: No dose adjustment is required based on body weight (see Pharmacology: Pharmacokinetics under Action).
Ethnic differences: No dose adjustment is required based on ethnic differences (see Pharmacology: Pharmacokinetics under Action).
10, 15 and 20 mg: Treatment and prevention of recurrent DVT and PE: Method of administration: Oral use.
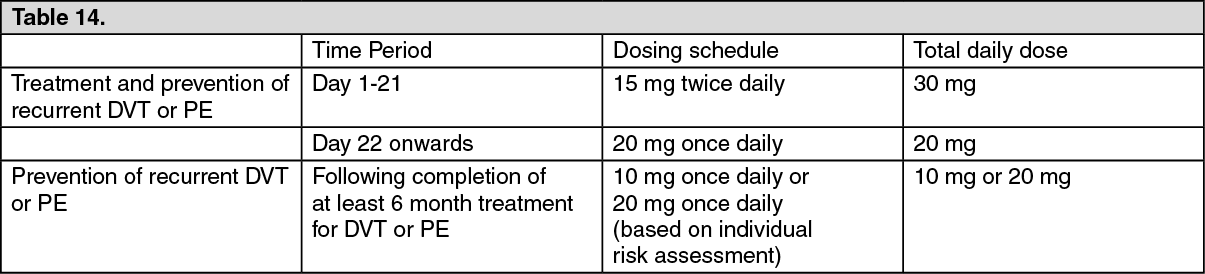
Treatment and prevention of recurrent DVT and PE: Recommended usual dose: The recommended dose for the initial treatment of acute DVT and PE is Rivaroxaban (Xarelto) 15 mg twice daily for the first three weeks followed by Rivaroxaban (Xarelto) 20 mg once daily for the continued treatment and the prevention of recurrent DVT and PE. Following completion of at least 6 months treatment for DVT or PE, Rivaroxaban (Xarelto) 10 mg once daily or Rivaroxaban (Xarelto) 20 mg once daily is recommended based on an individual assessment of the risk of recurrent DVT or PE against the risk for bleeding. See Table 14.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTreatment and prevention of recurrent DVT and PE: Duration of treatment: Therapy should be continued as long as the VTE risk persist (see Pharmacology: Pharmacodynamics: SPAF: Clinical efficacy and safety under Actions).
Treatment and prevention of recurrent DVT and PE: Method and frequency of administration: During the initial 3 weeks of acute treatment 15 mg of Rivaroxaban (Xarelto) should be taken twice daily.
After the initial 3 weeks treatment Rivaroxaban (Xarelto) should be continued at 20 mg once daily.
After at least 6 months treatment Rivaroxaban (Xarelto) should be taken at 10 mg once daily or 20 mg once daily (see Pharmacology: Pharmacodynamics under Actions).
Rivaroxaban (Xarelto) 15 mg tablets and Rivaroxaban (Xarelto) 20 mg tablets should be taken with food.
Rivaroxaban (Xarelto) 10 mg tablets may be taken with or without food (see Pharmacology: Pharmacokinetics under Actions).
For patients who are unable to swallow whole tablets, Rivaroxaban (Xarelto) tablet may be crushed and mixed with water or soft foods such as applesauce immediately prior to use and administered orally. After the administration of crushed Rivaroxaban (Xarelto) 15 mg or Rivaroxaban (Xarelto) 20 mg tablets, the dose should be immediately followed by food.
The crushed Rivaroxaban (Xarelto) tablet may be given through gastric tubes. Gastric placement of the tube should be confirmed before administering Rivaroxaban (Xarelto). The crushed tablet should be administered in a small amount of water via a gastric tube after which it should be flushed with water. After the administration of crushed Rivaroxaban (Xarelto)15 mg or 20 mg tablets, the dose should then be immediately followed by enteral feeding (see Pharmacology: Pharmacokinetics under Actions).
Treatment and prevention of recurrent DVT and PE: Missed Dose: It is essential to adhere to the dosage schedule provided.
If a dose is missed during the 15 mg twice daily treatment phase the patient should take Rivaroxaban (Xarelto) immediately to ensure intake of 30 mg Rivaroxaban (Xarelto) per day. In this case two 15 mg tablets may be taken at once. The patient should continue with the regular 15 mg twice daily intake as recommended on the following day.
If a dose is missed during the once daily treatment phase the patient should take Rivaroxaban (Xarelto) immediately to ensure intake of the recommended daily dose. The patient should continue with the regular once daily dose as recommended on the following day.
Treatment and prevention of recurrent DVT and PE: Maximum daily dose: The recommended maximum daily dose is 30 mg during the first 3 weeks of treatment.
In the following treatment phase the recommended maximum daily dose is 20 mg.
Treatment and prevention of recurrent DVT and PE: Additional information on special populations: Treatment and prevention of recurrent DVT and PE: Patients with hepatic impairment: Rivaroxaban (Xarelto) is contraindicated in patients with hepatic disease which is associated with coagulopathy leading to a clinically relevant bleeding risk (see Contraindications).
No dose adjustment is necessary in patients with other hepatic diseases (see Pharmacology: Pharmacokinetics under Actions).
Limited clinical data in patients with moderate hepatic impairment (Child Pugh B) indicate a significant increase in the pharmacological activity (see Pharmacology: Pharmacokinetics under Actions).
No clinical data are available for patients with severe hepatic impairment (Child Pugh C) (see Contraindications and Pharmacology: Pharmacokinetics under Actions).
Treatment and prevention of recurrent DVT and PE: Patients with renal impairment: No dose adjustment is required if Rivaroxaban (Xarelto) is administered in patients with mild (Creatinine clearance (CrC): ≤80-50 mL/min) or moderate (CrC: <50-30 mL/min) renal impairment (see Pharmacology: Pharmacokinetics under Actions).
Limited clinical data for patients with severe renal impairment (CrC: <30-15 mL/min) indicate that rivaroxaban plasma levels are significantly increased in this patient population. Therefore Rivaroxaban (Xarelto) must be used with caution in these patients (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Use of Rivaroxaban (Xarelto) is not recommended in patients with CrC: <15 mL/min (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Treatment and prevention of recurrent DVT and PE: Converting from Vitamin K Antagonists (VKA) to Rivaroxaban (Xarelto): VKA treatment should be stopped and Rivaroxaban (Xarelto) therapy should be initiated once the INR is ≤ 2.5.
When converting patients from VKAs to Rivaroxaban (Xarelto), INR values will be falsely elevated after the intake of Rivaroxaban (Xarelto). The INR is not valid to measure the anticoagulant activity of Rivaroxaban (Xarelto), and therefore should not be used (see Interactions).
Treatment and prevention of recurrent DVT and PE: Converting from Rivaroxaban (Xarelto) to Vitamin K antagonists (VKA): There is a potential for inadequate anticoagulation during the transition from Rivaroxaban (Xarelto) to VKA. Continuous adequate anticoagulation should be ensured during any transition to an alternate anticoagulant. It should be noted that Rivaroxaban (Xarelto) can contribute to an elevated INR.
In patients converting from Rivaroxaban (Xarelto) to VKA, VKA should be given concurrently until the INR is ≥2.0. For the first two days of the conversion period, standard VKA dosing should be used followed by VKA dosing guided by INR testing. While patients are on both Rivaroxaban (Xarelto) and VKA, the INR should not be tested earlier than 24 hours (after the previous dose but prior to the next dose of Rivaroxaban (Xarelto). Once Rivaroxaban (Xarelto) is discontinued INR testing may be done reliably 24 hours after the last dose (see Interactions).
Treatment and prevention of recurrent DVT and PE: Converting from parenteral anti-coagulants to Rivaroxaban (Xarelto): For patients currently receiving a parenteral anticoagulant, start Rivaroxaban (Xarelto) 0 to 2 hours before the time of the next scheduled administration of the parenteral drug (e.g. LMWH) or at the time of discontinuation of a continuously administered parenteral drug (e.g. intravenous unfractionated heparin).
Treatment and prevention of recurrent DVT and PE: Converting from Rivaroxaban (Xarelto) to parenteral anti-coagulants: Discontinue Rivaroxaban (Xarelto) and give the first dose of parenteral anticoagulant at the time that the next Rivaroxaban (Xarelto) dose would be taken.
Treatment and prevention of recurrent DVT and PE: Children and adolescents (from birth to 16 or 18 years depending on local law): Safety and efficacy have not been established in children and adolescents below 18 years.
Treatment and prevention of recurrent DVT and PE: Geriatric patients: No dose adjustment is required based on age (see Pharmacology: Pharmacokinetics under Actions).
Treatment and prevention of recurrent DVT and PE: Gender: No dose adjustment is required based on gender (see Pharmacology: Pharmacokinetics under Actions).
Treatment and prevention of recurrent DVT and PE: Body weight: No dose adjustment is required based on body weight (see Pharmacology: Pharmacokinetics under Actions).
Treatment and prevention of recurrent DVT and PE: Ethnic differences: No dose adjustment is required based on ethnic differences (see Pharmacology: Pharmacokinetics under Actions).
15 and 20 mg: SPAF: Method of administration: Oral use.
SPAF: Recommended usual dose: The recommended dose is 20 mg once daily.
For patients with moderate renal impairment (creatinine clearance (CrC): <50-30 mL/min) the recommended dose is 15 mg once daily.
SPAF: Duration of treatment: Therapy should be continued as long as risk factors for stroke and systemic embolism persist.
SPAF: Method and frequency of administration: One 20 mg tablet of Rivaroxaban (Xarelto) should be taken once daily.
For patients with moderate renal impairment (CrC: <50-30 mL/min) one 15 mg tablet of Rivaroxaban (Xarelto) should be taken once daily.
Rivaroxaban (Xarelto) 15 mg tablets and Rivaroxaban (Xarelto) 20 mg tablets should be taken with food (see Pharmacology: Pharmacokinetics under Actions).
For patients who are unable to swallow whole tablets, Rivaroxaban (Xarelto) tablet may be crushed and mixed with water or soft foods such as applesauce immediately prior to use and administered orally. After the administration of crushed Rivaroxaban (Xarelto) 15 mg or Rivaroxaban (Xarelto) 20 mg tablets, the dose should be immediately followed by food.
The crushed Rivaroxaban (Xarelto) tablet may be given through gastric tubes. Gastric placement of the tube should be confirmed before administering Rivaroxaban (Xarelto). The crushed tablet should be administered in a small amount of water via a gastric tube after which it should be flushed with water. After the administration of crushed Rivaroxaban (Xarelto) 15 mg or 20 mg tablets, the dose should then be immediately followed by enteral feeding (see Pharmacology: Pharmacokinetics under Actions).
SPAF: Missed Dose: If a dose is missed the patient should take Rivaroxaban (Xarelto) immediately and continue with the once daily intake as recommended on the following day.
The dose should not be doubled to make up for a missed dose within the same day.
SPAF: Maximum daily dose: The recommended maximum daily dose is 20 mg.
SPAF: Additional information on special populations: SPAF: Patients with hepatic impairment: Rivaroxaban (Xarelto) is contraindicated in patients with hepatic disease which is associated with coagulopathy leading to a clinically relevant bleeding risk (see Contraindications).
No dose adjustment is necessary in patients with other hepatic diseases (see Pharmacology: Pharmacokinetics under Actions).
Limited clinical data in patients with moderate hepatic impairment (Child Pugh B) indicate a significant increase in the pharmacological activity. No clinical data are available for patients with severe hepatic impairment (Child Pugh C) (see Pharmacology: Pharmacokinetics under Actions and Contraindications).
SPAF: Patients with renal impairment: No dose adjustment is required if Rivaroxaban (Xarelto) is administered in patients with mild (creatinine clearance (CrC): ≤80-50 mL/min) renal impairment (see Pharmacology: Pharmacokinetics under Actions).
For patients with moderate (CrC: <50-30 mL/min) renal impairment the recommended dose is 15 mg once daily (see Pharmacology: Pharmacokinetics under Actions).
Limited clinical data for patients with severe renal impairment (CrC: <30-15 mL/min) indicate that rivaroxaban plasma levels are significantly increased in this patient population. Therefore, Rivaroxaban (Xarelto) 15 mg must be used with caution in these patients (see Pharmacology: Pharmacokinetics under Actions and Precautions).
Use of Rivaroxaban (Xarelto) is not recommended in patients with CrC <15 mL/min (see Pharmacology: Pharmacokinetics under Actions and Precautions).
SPAF: Converting from Vitamin K Antagonists (VKA) to Rivaroxaban (Xarelto): VKA treatment should be stopped and Rivaroxaban (Xarelto) therapy should be initiated when the INR is ≤ 3.0.
When converting patients from VKAs to Rivaroxaban (Xarelto), INR values will be falsely elevated after the intake of Rivaroxaban (Xarelto). The INR is not valid to measure the anticoagulant activity of Rivaroxaban (Xarelto), and therefore should not be used (see Interactions).
SPAF: Converting from Rivaroxaban (Xarelto) to Vitamin K antagonists (VKA): There is a potential for inadequate anticoagulation during the transition from Rivaroxaban (Xarelto) to VKA. Continuous adequate anticoagulation should be ensured during any transition to an alternate anticoagulant. It should be noted that Rivaroxaban (Xarelto) can contribute to an elevated INR.
In patients converting from Rivaroxaban (Xarelto) to VKA, VKA should be given concurrently until the INR is ≥2.0. For the first two days of the conversion period, standard VKA dosing should be used followed by VKA dosing guided by INR testing. While patients are on both Rivaroxaban (Xarelto) and VKA, the INR should not be tested earlier than 24 hours (after the previous dose but prior to the next dose of Rivaroxaban (Xarelto). Once Rivaroxaban (Xarelto) is discontinued INR testing may be done reliably 24 hours after the last dose (see Interactions).
SPAF: Converting from parenteral anti-coagulants to Rivaroxaban (Xarelto): For patients currently receiving a parenteral anticoagulant, start Rivaroxaban (Xarelto) 0 to 2 hours before the time of the next scheduled administration of the parenteral drug (e.g. LMWH) or at the time of discontinuation of a continuously administered parenteral drug (e.g. intravenous unfractionated heparin).
SPAF: Converting from Rivaroxaban (Xarelto) to parenteral anticoagulants: Discontinue Rivaroxaban (Xarelto) and give the first dose of parenteral anticoagulant at the time that the next Rivaroxaban (Xarelto) dose would be taken.
SPAF: Cardioversion: Rivaroxaban (Xarelto) can be initiated or continued in patients who may require cardioversion.
For transesophageal echocardiogram (TEE) guided cardioversion in patients not previously treated with anticoagulants, Rivaroxaban (Xarelto) treatment should be started at least 4 hours before cardioversion to ensure adequate anticoagulation (see Pharmacology: Pharmacodynamics and Pharmacokinetics under Actions).
SPAF: Patients who undergo PCI (percutaneous coronary intervention) with stent placement: Patients with non-valvular atrial fibrillation who undergo PCI with stent placement should receive reduced dose of 15 mg Rivaroxaban (Xarelto) once daily (or 10 mg Rivaroxaban (Xarelto) once daily for patients with moderate renal impairment [CrCl: <50-30 mL/min]) in addition to a P2Y12 inhibitor. This treatment regimen is recommended for a maximum of 12 months after PCI with stent placement (see Pharmacology: Pharmacodynamics under Actions and Precautions). After completion of the antiplatelet therapy, rivaroxaban dosage should be increased to the standard dose for patients with non-valvular atrial fibrillation.
SPAF: Children and adolescents (from birth to 16 or 18 years depending on local law): Safety and efficacy have not been established in children and adolescents below 18 years.
SPAF: Geriatric patients: No dose adjustment is required based on age (see Pharmacology: Pharmacokinetics under Actions).
SPAF: Gender: No dose adjustment is required based on gender (see Pharmacology: Pharmacokinetics under Actions).
SPAF: Body weight: No dose adjustment is required based on body weight (see Pharmacology: Pharmacokinetics under Actions).
SPAF: Ethnic differences: No dose adjustment is required based on ethnic differences (see Pharmacology: Pharmacokinetics under Actions).