


 Sign Out
Sign Out




Clinical Studies Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety population described in Precautions reflect exposure to Abemaciclib (Yulareb) in 3691 patients from four clinical trials: monarchE, MONARCH 1, MONARCH 2, and MONARCH 3. The safety population includes exposure to Abemaciclib (Yulareb) as a single agent at 200 mg twice daily in 132 patients in MONARCH 1 and to Abemaciclib (Yulareb) at 150 mg twice daily in 3559 patients administered in combination with fulvestrant, tamoxifen, or an aromatase inhibitor in monarchE, MONARCH 2, and MONARCH 3. The median duration of exposure ranged from 4.5 months in MONARCH 1 to 24 months in monarchE. The most common adverse reactions (incidence ≥20%) across clinical trials were: diarrhea, neutropenia, nausea, abdominal pain, infections, fatigue, anemia, leukopenia, decreased appetite, vomiting, headache, alopecia, and thrombocytopenia.
Early Breast Cancer: monarchE: Abemaciclib (Yulareb) in Combination with Tamoxifen or an Aromatase Inhibitor as Adjuvant Treatment: Adult patients with HR-positive, HER2-negative, node-positive early breast cancer at a high risk of recurrence: The safety of Abemaciclib (Yulareb) was evaluated in monarchE, a study of 5591 adult patients receiving Abemaciclib (Yulareb) plus endocrine therapy (tamoxifen or an aromatase inhibitor) or endocrine therapy (tamoxifen or an aromatase inhibitor) alone [see Clinical Studies]. Patients were randomly assigned to receive 150 mg of Abemaciclib (Yulareb) orally, twice daily, plus tamoxifen or an aromatase inhibitor, or tamoxifen or an aromatase inhibitor, for two years or until discontinuation criteria were met. The median duration of Abemaciclib (Yulareb) treatment was 24 months.
The most frequently reported (≥5%) Grade 3 or 4 adverse reactions were neutropenia, leukopenia, diarrhea, and lymphopenia.
Fatal adverse reactions occurred in 0.8% of patients who received Abemaciclib (Yulareb) plus endocrine therapy (tamoxifen or an aromatase inhibitor), including: cardiac failure (0.1%), cardiac arrest, myocardial infarction, ventricular fibrillation, cerebral hemorrhage, cerebrovascular accident, pneumonitis, hypoxia, diarrhea and mesenteric artery thrombosis (0.03% each).
Permanent Abemaciclib (Yulareb) treatment discontinuation due to an adverse reaction was reported in 19% of patients receiving Abemaciclib (Yulareb), plus tamoxifen or an aromatase inhibitor. Of the patients receiving tamoxifen or an aromatase inhibitor, 1% permanently discontinued due to an adverse reaction. The most common adverse reactions leading to Abemaciclib (Yulareb) discontinuations were diarrhea (5%), fatigue (2%), and neutropenia (0.9%).
Dose interruption of Abemaciclib (Yulareb) due to an adverse reaction occurred in 62% of patients receiving Abemaciclib (Yulareb) plus tamoxifen or aromatase inhibitors. Adverse reactions leading to Abemaciclib (Yulareb) dose interruptions in ≥5% of patients were diarrhea (20%), neutropenia (16%), leukopenia (7%), and fatigue (5%).
Dose reductions of Abemaciclib (Yulareb) due to an adverse reaction occurred in 44% of patients receiving Abemaciclib (Yulareb) plus endocrine therapy (tamoxifen or an aromatase inhibitor). Adverse reactions leading to Abemaciclib (Yulareb) dose reductions in ≥5% were diarrhea (17%), neutropenia (8%), and fatigue (5%).
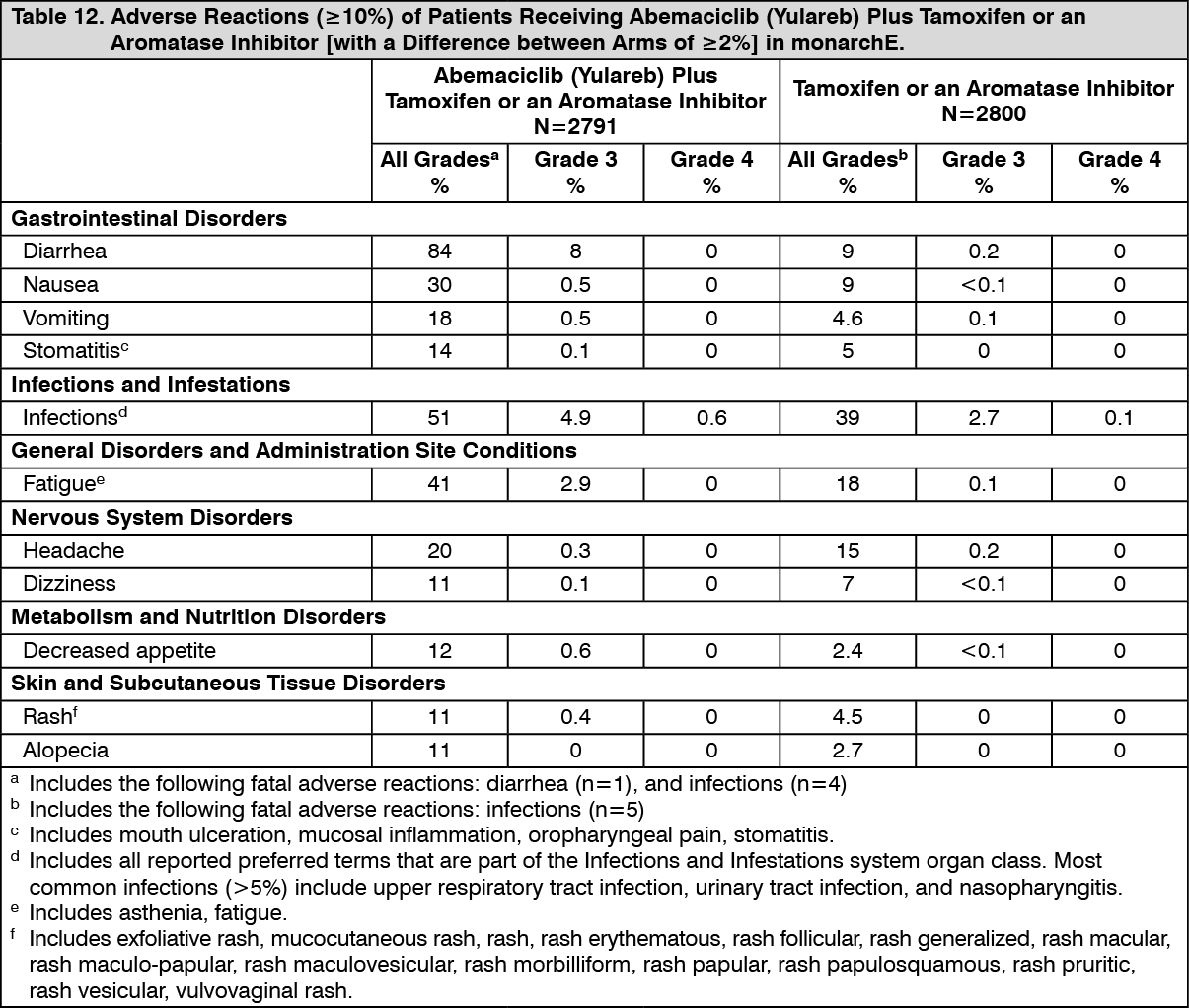
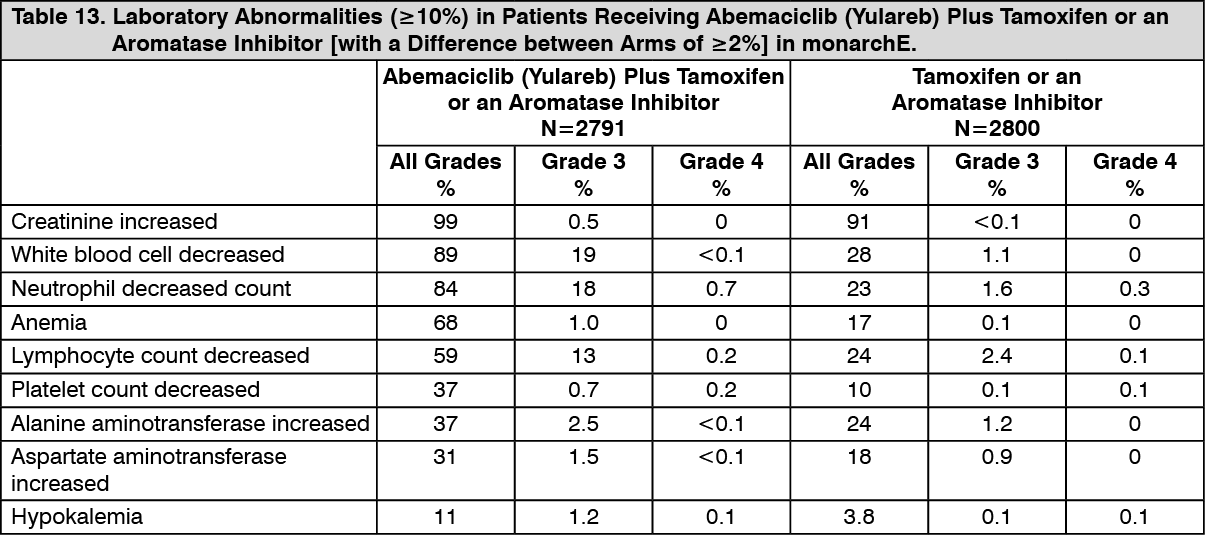
The most common adverse reactions reported (≥20%) in the Abemaciclib (Yulareb), plus tamoxifen or an aromatase inhibitor, arm and ≥2% higher than the tamoxifen or an aromatase inhibitor arm were: diarrhea, infections, neutropenia, fatigue, leukopenia, nausea, anemia, and headache. Adverse reactions are shown in Table 12 and laboratory abnormalities are shown in Table 13. (See Tables 12 and 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageClinically relevant adverse reactions in <10% of patients who received Abemaciclib (Yulareb) in combination with tamoxifen or an aromatase inhibitor in monarchE include: Pruritus-9%; Dyspepsia-8%; Nail disorder-6% (includes nail bed disorder, nail bed inflammation, nail discoloration, nail disorder, nail dystrophy, nail pigmentation, nail ridging, nail toxicity, onychalgia, onychoclasis, onycholysis, onychomadesis); Lacrimation increased-6%; Dysgeusia-5%; Interstitial lung disease (ILD)/pneumonitis-3% (includes pneumonitis, radiation pneumonitis, interstitial lung disease, pulmonary fibrosis, organizing pneumonia, radiation fibrosis-lung, lung opacity, sarcoidosis); Venous thromboembolic events (VTEs)-3% (includes catheter site thrombosis, cerebral venous thrombosis, deep vein thrombosis, device related thrombosis, embolism, hepatic vein thrombosis, jugular vein occlusion, jugular vein thrombosis, ovarian vein thrombosis, portal vein thrombosis, pulmonary embolism, subclavian vein thrombosis, venous thrombosis limb).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdvanced or Metastatic Breast Cancer: MONARCH 3: Abemaciclib (Yulareb) in Combination with an Aromatase Inhibitor (Anastrozole or Letrozole) as Initial Endocrine-Based Therapy: Postmenopausal Women with HR-positive, HER2-negative locoregionally recurrent or metastatic breast cancer with no prior systemic therapy in this disease setting: The safety of Abemaciclib (Yulareb) was evaluated in MONARCH 3, a study of 488 women receiving Abemaciclib (Yulareb) plus an aromatase inhibitor or placebo plus an aromatase inhibitor [see Pharmacology: Clinical Studies under Actions]. Patients were randomly assigned to receive 150 mg of Abemaciclib (Yulareb) or placebo orally twice daily, plus physician's choice of anastrozole or letrozole once daily. Median duration of treatment was 15.1 months for the Abemaciclib (Yulareb) arm and 13.9 months for the placebo arm.
The most frequently reported (≥5%) Grade 3 or 4 adverse reactions were neutropenia, diarrhea, leukopenia, increased ALT, and anemia.
Deaths during treatment or during the 30-day follow up, regardless of causality, were reported in 11 cases (3%) of Abemaciclib (Yulareb) plus an aromatase inhibitor treated patients versus 3 cases (2%) of placebo plus an aromatase inhibitor treated patients. Causes of death for patients receiving Abemaciclib (Yulareb) plus an aromatase inhibitor included: 3 (0.9%) patient deaths due to underlying disease, 3 (0.9%) due to lung infection, 3 (0.9%) due to VTE, 1 (0.3%) due to pneumonitis, and 1 (0.3%) due to cerebral infarction.
Permanent treatment discontinuation due to an adverse event was reported in 13% of patients receiving Abemaciclib (Yulareb) plus an aromatase inhibitor and in 3% of patients receiving placebo plus an aromatase inhibitor. Adverse reactions leading to permanent discontinuation for patients receiving Abemaciclib (Yulareb) plus an aromatase inhibitor were diarrhea (2%), ALT increased (2%), infection (1%), venous thromboembolic events (VTE) (1%), neutropenia (0.9%), renal impairment (0.9%), AST increased (0.6%), dyspnea (0.6%), pulmonary fibrosis (0.6%) and anemia, rash, weight decreased and thrombocytopenia (each 0.3%).
Dose interruption of Abemaciclib (Yulareb) due to an adverse reaction occurred in 56% of patients receiving Abemaciclib (Yulareb) plus anastrazole or letrozole. Adverse reactions leading to Abemaciclib (Yulareb) dose interruptions in ≥5% of patients were neutropenia (16%) and diarrhea (15%).
Dose reductions due to an adverse reaction occurred in 43% of patients receiving Abemaciclib (Yulareb) plus anastrozole or letrozole. Adverse reactions leading to dose reductions in ≥5% of patients were diarrhea and neutropenia. Abemaciclib (Yulareb) dose reductions due to diarrhea of any grade occurred in 13% of patients receiving Abemaciclib (Yulareb) plus an aromatase inhibitor compared to 2% of patients receiving placebo plus an aromatase inhibitor. Abemaciclib (Yulareb) dose reductions due to neutropenia of any grade occurred in 11% of patients receiving Abemaciclib (Yulareb) plus an aromatase inhibitor compared to 0.6% of patients receiving placebo plus an aromatase inhibitor.
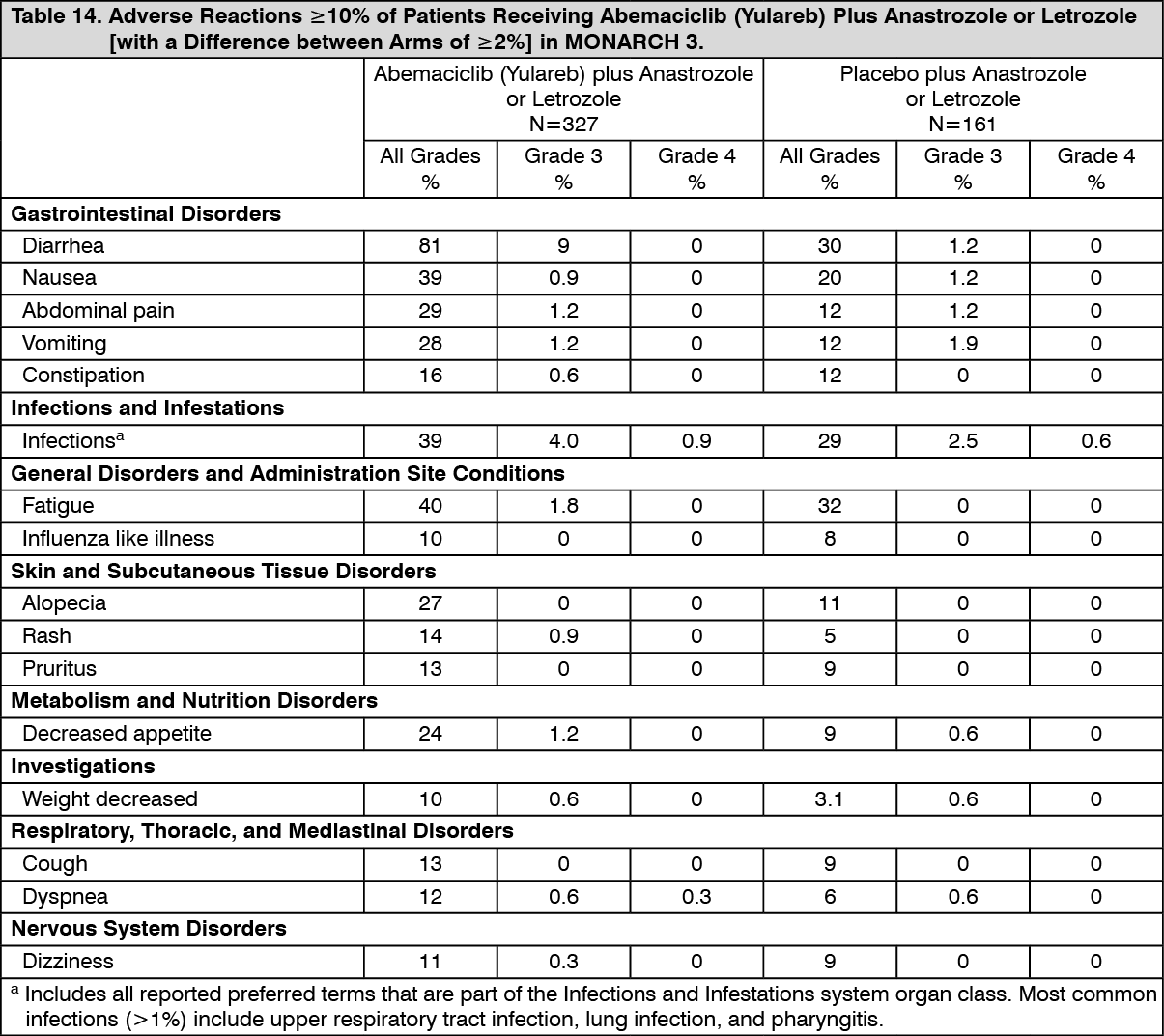
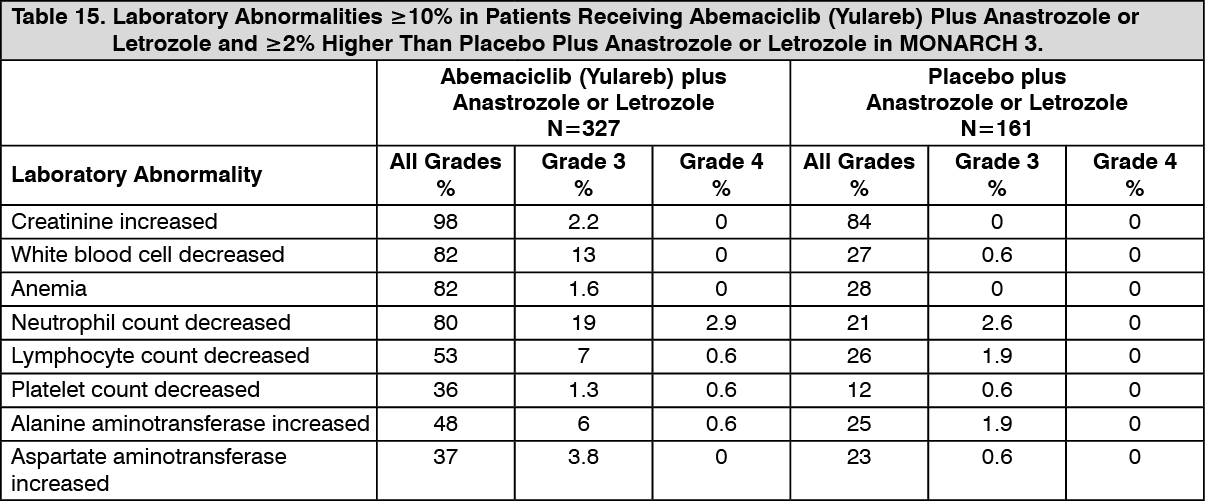
The most common adverse reactions reported (≥20%) in the Abemaciclib (Yulareb) arm and ≥2% than the placebo arm were diarrhea, neutropenia, fatigue, infections, nausea, abdominal pain, anemia, vomiting, alopecia, decreased appetite, and leukopenia. Adverse reactions are shown in Table 14 and laboratory abnormalities in Table 15. Diarrhea incidence was greatest during the first month of Abemaciclib (Yulareb) dosing. The median time to onset of the first diarrhea event was 8 days, and the median durations of diarrhea for Grades 2 and for Grade 3 were 11 days and 8 days, respectively. Most diarrhea events recovered or resolved (88%) with supportive treatment and/or dose reductions [see Dosage & Administration]. Nineteen percent of patients with diarrhea required a dose omission and 13% required a dose reduction. The median time to the first dose reduction due to diarrhea was 38 days. (See Table 14.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional adverse reactions in MONARCH 3 include venous thromboembolic events (deep vein thrombosis, pulmonary embolism, and pelvic venous thrombosis), which were reported in 5% of patients treated with Abemaciclib (Yulareb) plus anastrozole or letrozole as compared to 0.6% of patients treated with anastrozole or letrozole plus placebo. (See Table 15.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageCreatinine Increased: Abemaciclib has been shown to increase serum creatinine due to inhibition of renal tubular secretion transporters, without affecting glomerular function [see Pharmacology: Pharmacokinetics under Actions]. Across the clinical studies, increases in serum creatinine (mean increase, 0.2-0.3 mg/dL) occurred within the first 28-day cycle of Abemaciclib (Yulareb) dosing, remained elevated but stable through the treatment period, and were reversible upon treatment discontinuation. Alternative markers such as BUN, cystatin C, or calculated GFR, which are not based on creatinine, may be considered to determine whether renal function is impaired.
MONARCH 2: Abemaciclib (Yulareb) in Combination with Fulvestrant: Women with HR-positive, HER2-negative advanced or metastatic breast cancer with disease progression on or after prior adjuvant or metastatic endocrine therapy: The safety of Abemaciclib (Yulareb) (150 mg twice daily) plus fulvestrant (500 mg) versus placebo plus fulvestrant was evaluated in MONARCH 2 [see Pharmacology: Clinical Studies under Actions]. The data described as follows reflect exposure to Abemaciclib (Yulareb) in 441 patients with HR-positive, HER2-negative advanced breast cancer who received at least one dose of Abemaciclib (Yulareb) plus fulvestrant in MONARCH 2.
Median duration of treatment was 12 months for patients receiving Abemaciclib (Yulareb) plus fulvestrant and 8 months for patients receiving placebo plus fulvestrant.
The most frequently reported (≥5%) Grade 3 or 4 adverse reactions were neutropenia, diarrhea, leukopenia, anemia, and infections.
Deaths during treatment or during the 30-day follow up, regardless of causality, were reported in 18 cases (4%) of Abemaciclib (Yulareb) plus fulvestrant treated patients versus 10 cases (5%) of placebo plus fulvestrant treated patients. Causes of death for patients receiving Abemaciclib (Yulareb) plus fulvestrant included: 7 (2%) patient deaths due to underlying disease, 4 (0.9%) due to sepsis, 2 (0.5%) due to pneumonitis, 2 (0.5%) due to hepatotoxicity, and one (0.2%) due to cerebral infarction.
Permanent study treatment discontinuation due to an adverse event were reported in 9% of patients receiving Abemaciclib (Yulareb) plus fulvestrant and in 3% of patients receiving placebo plus fulvestrant. Adverse reactions leading to permanent discontinuation for patients receiving Abemaciclib (Yulareb) plus fulvestrant were infection (2%), diarrhea (1%), hepatotoxicity (1%), fatigue (0.7%), nausea (0.2%), abdominal pain (0.2%), acute kidney injury (0.2%), and cerebral infarction (0.2%).
Dose interruption of Abemaciclib (Yulareb) due to an adverse reaction occurred in 52% of patients receiving Abemaciclib (Yulareb) plus fulvestrant. Adverse reactions leading to Abemaciclib (Yulareb) dose interruptions in ≥5% of patients were diarrhea (19%) and neutropenia (16%).
Dose reductions due to an adverse reaction occurred in 43% of patients receiving Abemaciclib (Yulareb) plus fulvestrant. Adverse reactions leading to dose reductions in ≥5% of patients were diarrhea and neutropenia. Abemaciclib (Yulareb) dose reductions due to diarrhea of any grade occurred in 19% of patients receiving Abemaciclib (Yulareb) plus fulvestrant compared to 0.4% of patients receiving placebo and fulvestrant. Abemaciclib (Yulareb) dose reductions due to neutropenia of any grade occurred in 10% of patients receiving Abemaciclib (Yulareb) plus fulvestrant compared to no patients receiving placebo plus fulvestrant.
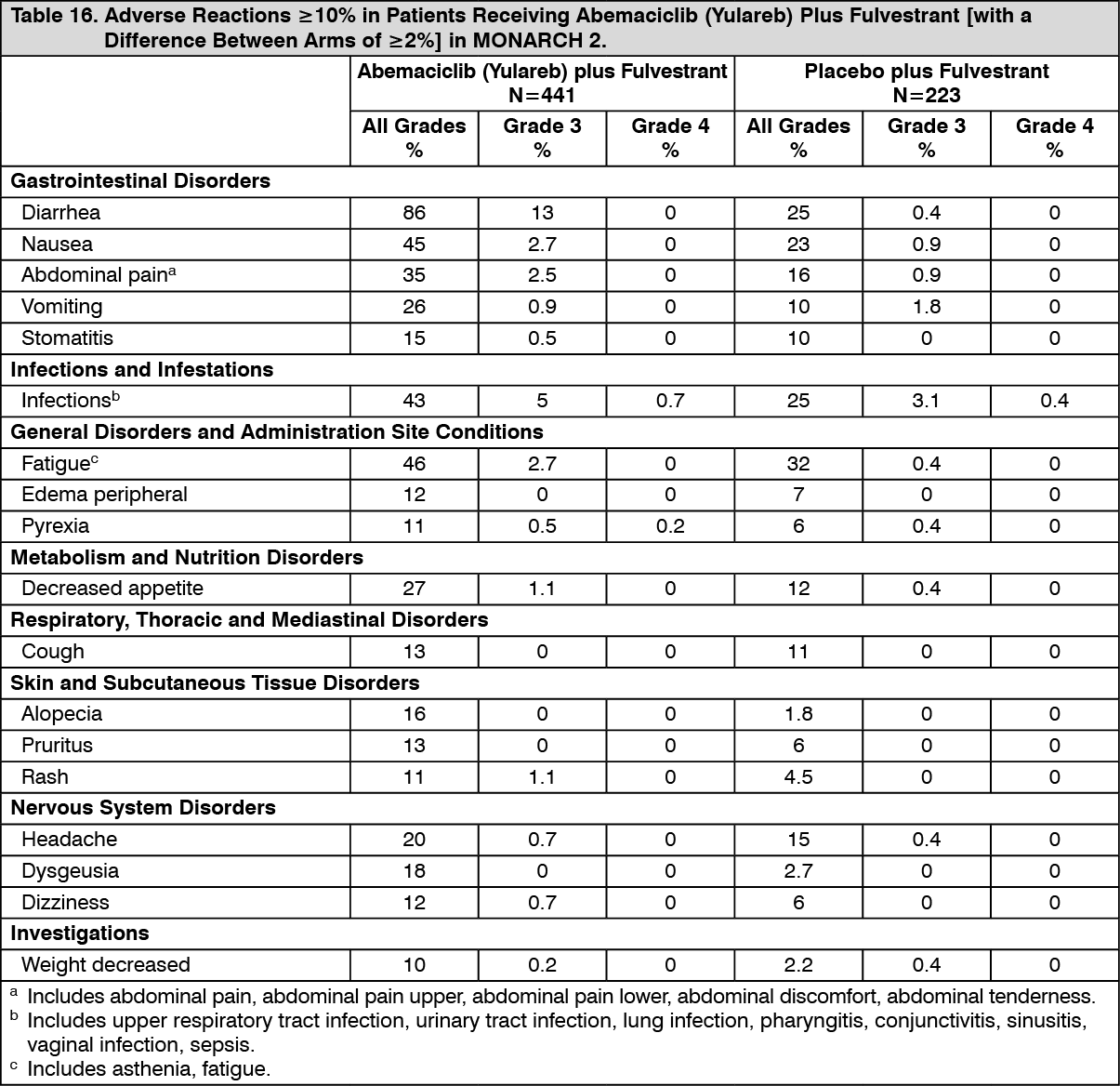
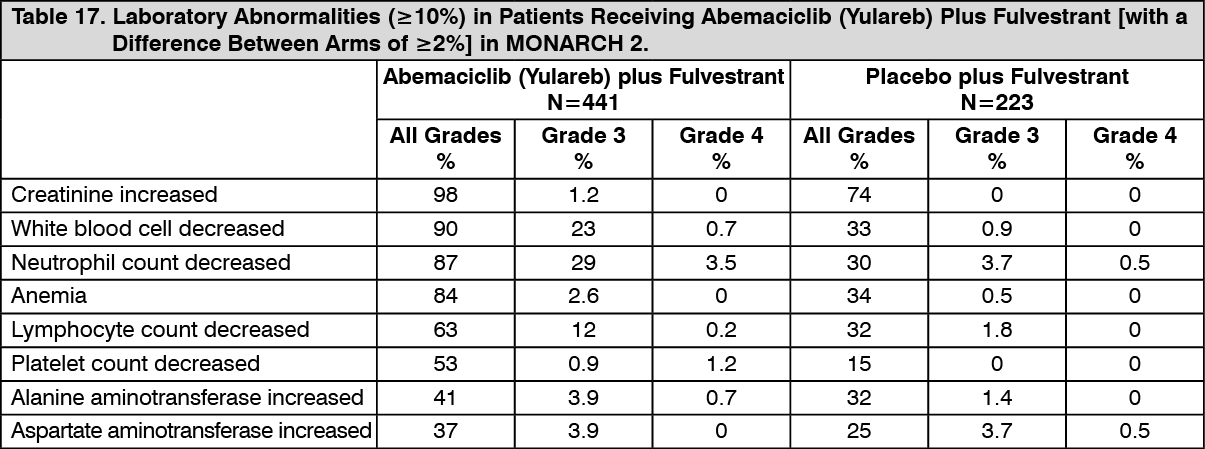
The most common adverse reactions reported (≥20%) in the Abemaciclib (Yulareb) arm were diarrhea, fatigue, neutropenia, nausea, infections, abdominal pain, anemia, leukopenia, decreased appetite, vomiting, and headache. Adverse reactions are shown in Table 16 and laboratory abnormalities in Table 17. (See Table 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional adverse reactions in MONARCH 2 include venous thromboembolic events (deep vein thrombosis, pulmonary embolism, cerebral venous sinus thrombosis, subclavian vein thrombosis, axillary vein thrombosis, and DVT inferior vena cava), which were reported in 5% of patients treated with Abemaciclib (Yulareb) plus fulvestrant as compared to 0.9% of patients treated with fulvestrant plus placebo. (See Table 17.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageCreatinine Increased: Abemaciclib has been shown to increase serum creatinine due to inhibition of renal tubular secretion transporters, without affecting glomerular function [see Pharmacology: Pharmacokinetics under Actions]. In clinical studies, increases in serum creatinine (mean increase, 0.2-0.3 mg/dL) occurred within the first 28-day cycle of Abemaciclib (Yulareb) dosing, remained elevated but stable through the treatment period, and were reversible upon treatment discontinuation. Alternative markers such as BUN, cystatin C, or calculated glomerular filtration rate (GFR), which are not based on creatinine, may be considered to determine whether renal function is impaired.
Monarch 1: Abemaciclib (Yulareb) Administered as a Monotherapy in Metastatic Breast Cancer: Patients with HR-positive, HER2-negative breast cancer who received prior endocrine therapy and 1-2 chemotherapy regimens in the metastatic setting: The safety of Abemaciclib (Yulareb) was evaluated in MONARCH 1, a single-arm, open-label, multicenter study in 132 women with measurable HR-positive, HER2-negative metastatic breast cancer [see Pharmacology: Clinical Studies under Actions]. Patients received 200 mg Abemaciclib (Yulareb) orally twice daily until development of progressive disease or unmanageable toxicity. Median duration of treatment was 4.5 months.
The most frequently reported (≥5%) Grade 3 or 4 adverse reactions were diarrhea, neutropenia, fatigue, and leukopenia.
Deaths due to adverse events during treatment or during the 30-day follow up were reported in 2% of patients. Cause of death in these patients was due to infection (2 patients) or pneumonitis (1 patient).
Ten patients (8%) discontinued study treatment from adverse reactions due to (1 patient each) abdominal pain, arterial thrombosis, aspartate aminotransferase (AST) increased, blood creatinine increased, chronic kidney disease, diarrhea, ECG QT prolonged, fatigue, hip fracture, and lymphopenia.
Dose interruption of Abemaciclib (Yulareb) due to an adverse reaction occurred in 58% of patients. The most frequent (≥5%) adverse reactions leading to dose interruptions were diarrhea (24%), neutropenia (16%), fatigue (10%), vomiting (6%),and nausea (5%).
Forty-nine percent of patients had dose reductions due to an adverse reaction. The most frequent adverse reactions that led to dose reductions were diarrhea (20%), neutropenia (11%), and fatigue (9%).
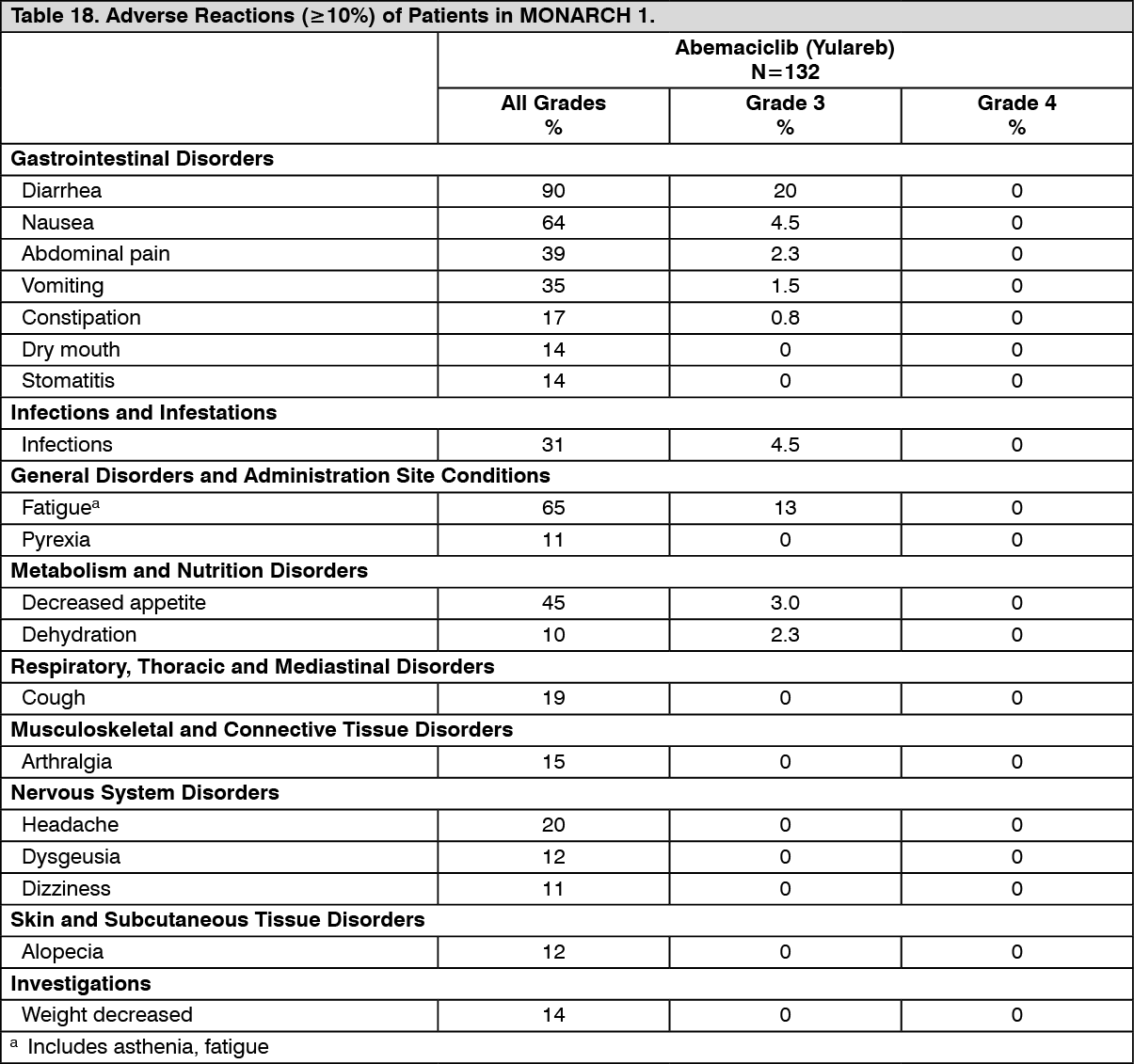
The most common reported adverse reactions (≥20%) were diarrhea, fatigue, nausea, decreased appetite, abdominal pain, neutropenia, vomiting, infections, anemia, headache, and thrombocytopenia. Adverse reactions are shown in Table 18 and laboratory abnormalities in Table 19. (See Tables 18 and 19.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image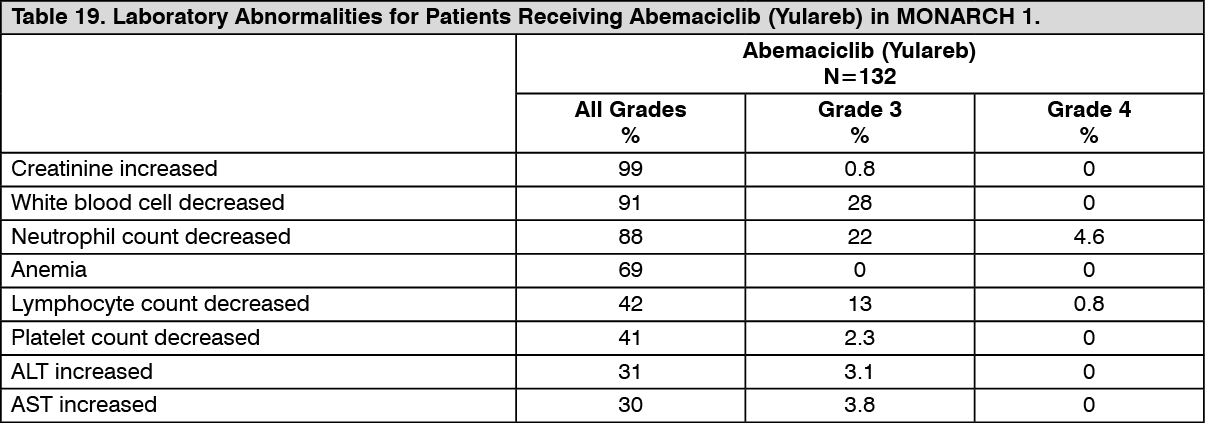 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageCreatinine Increased: Abemaciclib has been shown to increase serum creatinine due to inhibition of renal tubular secretion transporters, without affecting glomerular function [see Pharmacology: Pharmacokinetics under Actions]. In clinical studies, increases in serum creatinine (mean increase, 0.2-0.3 mg/dL) occurred within the first 28-day cycle of Abemaciclib (Yulareb) dosing, remained elevated but stable through the treatment period, and were reversible upon treatment discontinuation. Alternative markers such as BUN, cystatin C, or calculated GFR, which are not based on creatinine, may be considered to determine whether renal function is impaired.
Postmarketing Experience: The following adverse reactions have been identified during post-approval use of Abemaciclib (Yulareb). Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Respiratory disorders: Interstitial lung disease (ILD)/pneumonitis [see Interstitial Lung Disease (ILD)/Pneumonitis under Precautions].
View ADR Monitoring Form