


 Sign Out
Sign Out
Pharmacology: Pharmacodynamics: Mode of action: Azithromycin is an azalide, a sub-class of the macrolide antibiotics. By binding to the 50S-ribosomal sub-unit, azithromycin avoids the translocation of peptide chains from one side of the ribosome to the other. Azithromycin acts as a bacteriostatic.
PK/PD relationship: The efficacy of azithromycin is best described by the relationship AUC/MIC, where AUC describes the area under the curve and MIC represents the mean inhibitory concentration of the microbe concerned.
Mechanism of resistance: Resistance to azithromycin may be natural or acquired. There are 3 main mechanisms of resistance affecting azithromycin: Efflux: resistance may be due to an increase in the number of efflux pumps on the cell membrane. In particular, 14- and 15-link macrolides are affected. (M-phenotype).
Alterations of the cell structure: methylisation of the 23s rRNS may reduce the affinity of the ribosomal binding sites, which can result in microbial resistance to macrolides, lincosamides and group B streptogramins (SB) (MLSB-phenotype).
Enzymatic deactivation of macrolides is only of limited clinical significance.
In the presence of the M-phenotype, complete cross resistance exists between azithromycin and clarithromycin, erythromycin and roxithromycin. With the MLSB-phenotype, additional cross resistance exists with clindamycin and streptogramin B. A partial cross resistance exists with spiramycin.
Breakpoints: Testing of azithromycin is done by using the usual dilution series. The following minimum inhibitory concentrations for susceptible and resistant germs were determined: See Table 1.
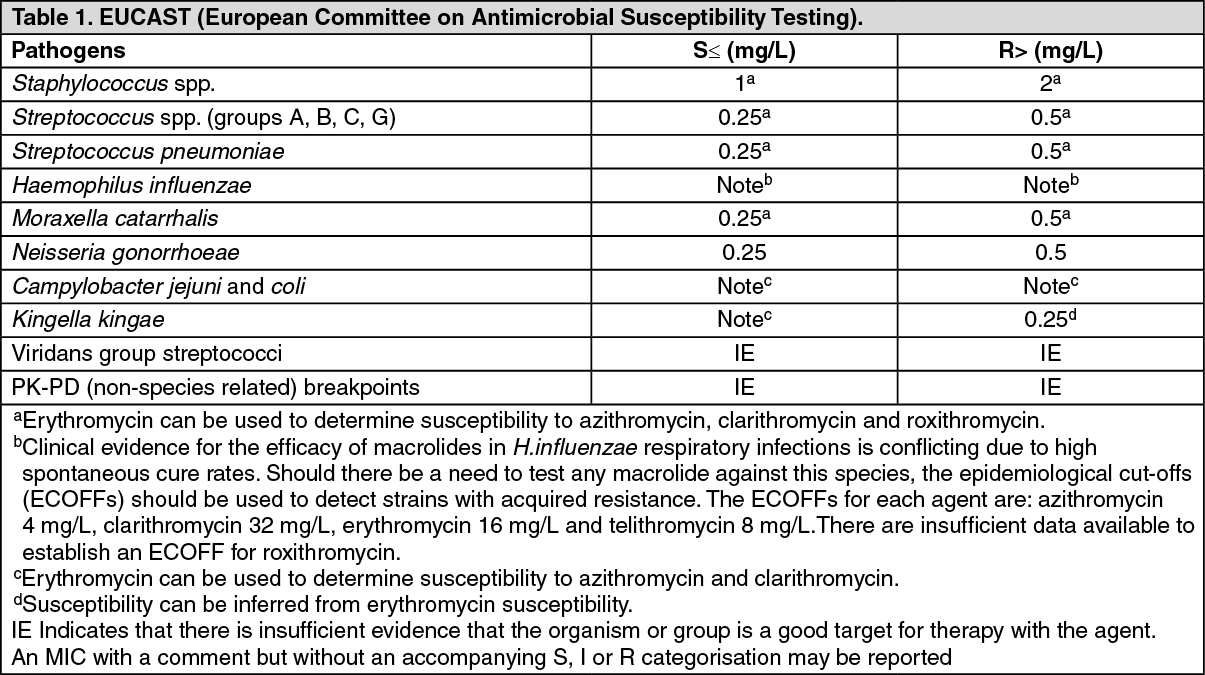 Click on icon to see table/diagram/image
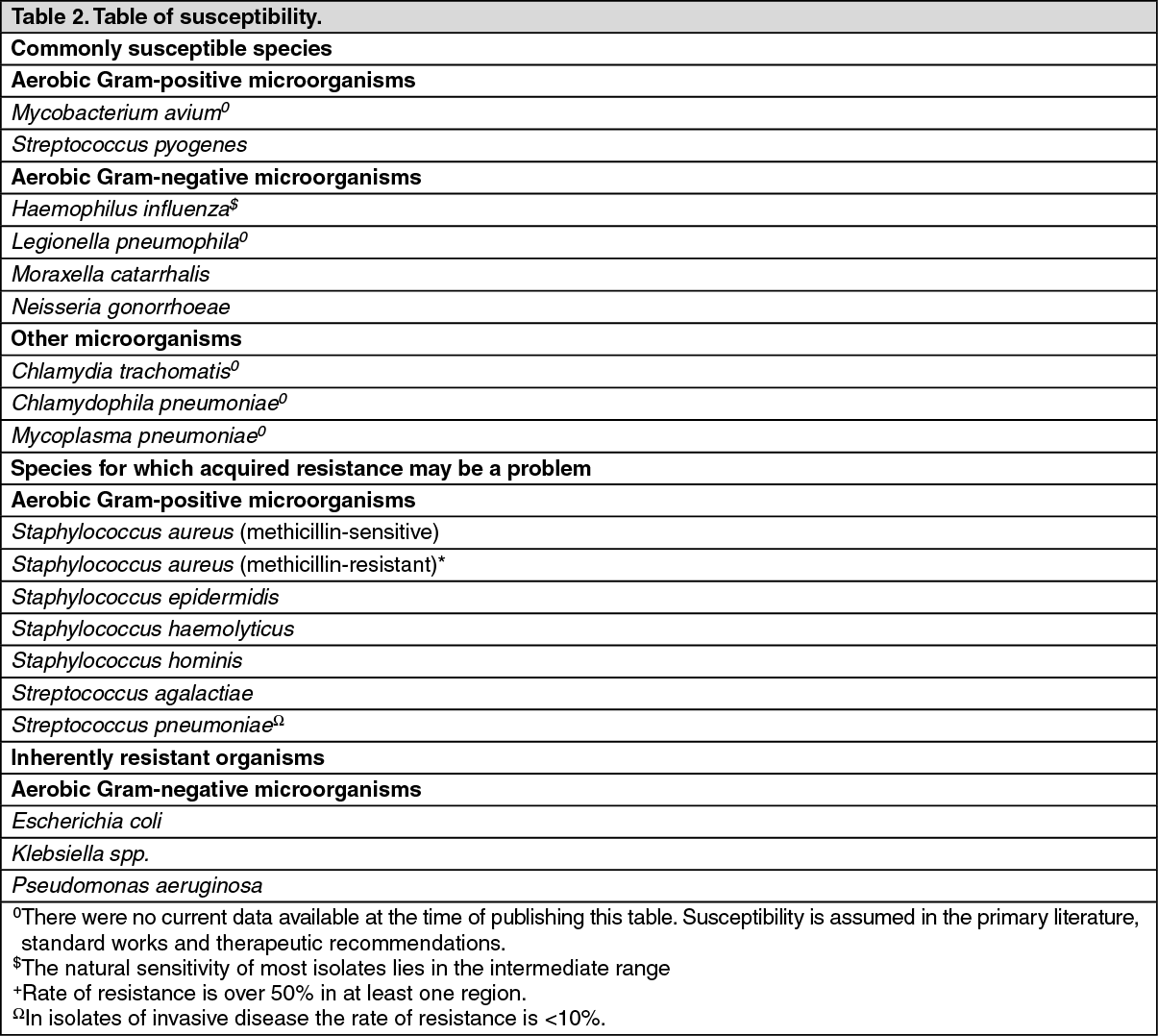
Click on icon to see table/diagram/imageSusceptibility: The prevalence of acquired resistance may vary geographically and with time for selected species and local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence of resistance is such that the utility of the agent in at least some types of infections is questionable.
Microbiological diagnosis with detection of the pathogen and its susceptibility to azithromycin should be attempted, particularly in the case of serious infections or treatment failures. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Absorption: After oral administration, peak plasma levels are reached after 2 to 3 hours; plasma terminal elimination half-life closely reflects the tissue depletion half-life of 2 to 4 days. After a 5 day treatment, slightly higher AUC values were seen in the elderly patients (>65 years of age) compared to the younger patients (<40 years of age). However these differences are not regarded as clinically relevant; therefore a dose adjustment is not recommended.
In animal tests, high concentrations of azithromycin have been found in phagocytes. It has also been established that during active phagocytosis higher concentrations of azithromycin are released from inactive phagocytes. In animal models, this results in high concentrations of azithromycin being delivered to the site of infection.
Non-linearity: Study data suggest non-linear pharmacokinetics of azithromycin in the therapeutic range.
Distribution: It has been demonstrated that the concentrations of azithromycin measured in tissues are noticeably higher (as much as 50 times) than those measured in plasma which indicates that the agent strongly binds to tissues. Concentrations in target tissues such as lung, tonsil, and prostate exceed the MIC90 for likely pathogens after a single dose of 500 mg.
Binding to serum proteins varies according to plasma concentration and ranges from 12% at 0.5μg/mL up to 52% at 0.05 μg azithromycin/mL serum. The mean volume of distribution at steady state (VVss) has been calculated to be 31.1 L/kg.
Elimination: About 12% of an intravenously administered dose is excreted unchanged within 3 days; the majority is excreted in the first 24 hours. Particularly high concentrations of unchanged azithromycin have been found in human bile. Also in bile, 10 metabolites were detected, which were formed through N- and O-demethylation, hydroxylation of desosamine and aglycone rings and cleavage of cladinose conjugate. Corresponding studies indicate that the metabolites of azithromycin are not microbiologically active.
Pharmacokinetics in special populations: Renal insufficiency: Following a single oral dose of azithromycin 1 g, pharmacokinetics were unchanged in subjects with a glomerular filtration rate <10 mL/min, there were statistically significant differences compared with subjects with normal renal function (GFR >80 mL/min) in AUC0-120 (8.8 μg x h/mL vs. 11.7 μg x h/mL), Cmax (1.0 μg/mL vs. 1.6 μg/mL) and CLr (2.3 mL/min/kg vs.0.2 mL/min/kg).
Hepatic insufficiency: In patients with mild to moderate hepatic impairment, there is no evidence of a marked change in serum pharmacokinetics of azithromycin compared to normal hepatic function. In these patients, urinary recovery of azithromycin appears to increase perhaps to compensate for reduced hepatic clearance.
Toxicology: Preclinical safety data: Phospholipidosis (intracellular phospholipid accumulation) has been observed in several tissues (e.g. eye, dorsal root ganglia, liver, gallbladder, kidney, spleen, and/or pancreas) of mice, rats, and dogs given multiple doses of azithromycin. Phospholipidosis has been observed to a similar extent in the tissues of neonatal rats and dogs. The effect has been shown to be reversible after cessation of azithromycin treatment. The significance of the finding for animals and humans is unknown.
Electrophysiological studies have shown that azithromycin prolongs the QT interval.
There was no evidence of a potential for genetic and chromosome mutations in in-vivo and in-vitro test models.
Long-term studies in animals have not been performed to evaluate carcinogenic potential as the medicinal product is indicated for short-term treatment only and there were no signs indicative of carcinogenic activity.
No teratogenic effects were observed in animal studies of embryotoxicity in mice and rats. In rats, azithromycin doses of 100 and 200 mg/kg bodyweight/day led to mild retardations in fetal ossification and in maternal weight gain. In peri-/postnatal studies in rats, mild retardations following treatment with 50 mg/kg/day azithromycin and above were observed (retardation in physical development and reflex behaviour).
In neonatal studies, rats and dogs did not show higher sensitivity to azithromycin than adult animals of the respective species.