Pharmacology: Pharmacodynamics: Zonisamide, like phenytoin and carbamazepine, selectively prevents tonic extensor convulsions induced by maximal electroshock in mice, rats, rabbits and dogs, and also those induced by pentylenetetrazol in mice.
Zonisamide strongly suppresses cortical focal seizures induced by electrical stimulation of the visual cortex as well as spike and wave discharges induced by cortical application of conjugated estrogen in cats.
Furthermore, zonisamide markedly suppresses both spike activities and secondarily generalized seizures induced by cortical application of tungstic acid gel in rats and by cortical freezing in cats.
Zonisamide reduces the duration of after-discharge and increases the threshold current for generalized convulsions in cortical and hippocampal-kindled rats.
Although the exact mechanism of action of zonisamide remains unclear, it is suggested that the drug exerts its anticonvulsant effects by blocking the spread or propagation of seizure discharges and by suppressing epileptogenic focus activity.
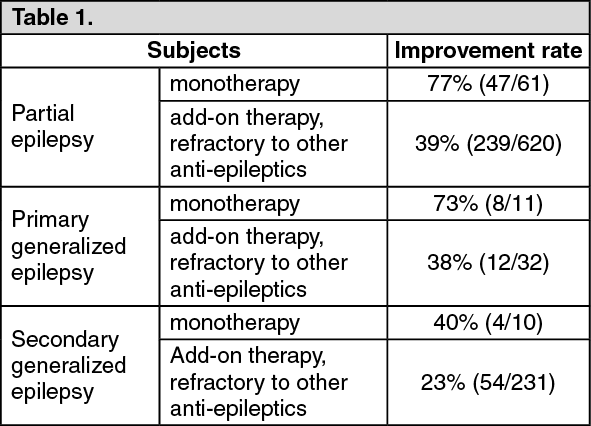
Clinical Studies: The results of clinical studies on the sum of 965 cases including double blind comparative study and comparative study are as shown as follows. (See Table 1.)
 Click on icon to see table/diagram/image
Pharmacokinetics: Plasma concentration:
Click on icon to see table/diagram/image
Pharmacokinetics: Plasma concentration: (Healthy adults, single administration of 200 mg): See Table 2.
Click on icon to see table/diagram/image
Plasma protein binding rate: 48.6% (
in vitro, human serum, centrifugal ultrafiltration method).
Main metabolites and metabolic pathway: Zonisamide is mainly metabolized in the liver and undergoes glucuronidation etc. after cleavage of isoxazole ring.
Excretion route and excretion rate: Excretion route: Mainly into urine.
Excretion rate: Excretion rate in urine 2 weeks after the administration was 28.9%-47.8% as unchanged compound and 12.4-18.7% as main metabolites which were glucuronides of isoxazole ring cleavage compound. Those were 47.6-60.2% of administered dose. (Healthy adults, 200 mg administration once or twice, and 400 mg administration twice).
Effective blood concentration: Though it depends on severity or individual case of epilepsy, about 20 μg/mL is indicated as a standard in general.
Metabolic enzyme: Subtypes of cytochrome P450: mainly CYP3A.
Pharmacokinetics in patients with renal dysfunction: (Foreign data, single administration of 300 mg). (See Table 3.)
Click on icon to see table/diagram/image
A difference was found between patients with renal dysfunction and those with normal renal function in renal clearance and excretion rate into urine.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image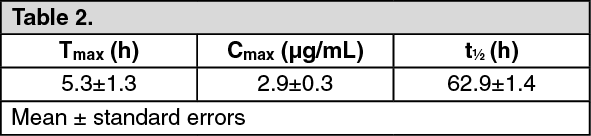 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image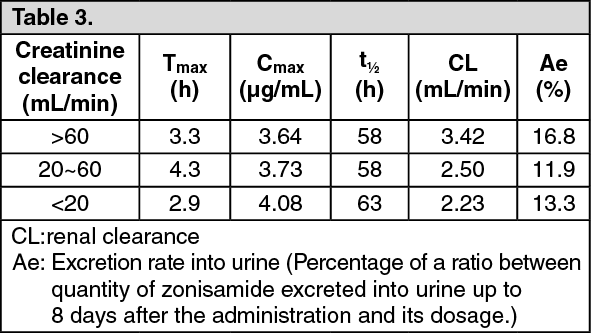 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out