Pharmacotherapeutic group: Antiepileptics. Other antiepileptics.
ATC code: N03AX15.
Pharmacology: Pharmacodynamics: Zonisamide is a benzisoxazole derivative. It is an anti-epileptic medicine with weak carbonic anhydrase activity
in-vitro. It is chemically unrelated to other anti-epileptic agents.
The mechanism of action of zonisamide is not fully elucidated, but it appears to act on voltage-sensitive sodium and calcium channels, thereby disrupting synchronised neuronal firing, reducing the spread of seizure discharges and disrupting subsequent epileptic activity. Zonisamide also has a modulatory effect on GABA-mediated neuronal inhibition.
Pharmacodynamic effects: The anticonvulsant activity of zonisamide has been evaluated in a variety of models, in several species with induced or innate seizures, and zonisamide appears to act as a broad-spectrum anti-epileptic in these models. Zonisamide prevents maximal electroshock seizures and restricts seizure spread, including the propagation of seizures from cortex to sub-cortical structures and suppresses epileptogenic focus activity. Unlike phenytoin and carbamazepine however, zonisamide acts preferentially on seizures originating in the cortex.
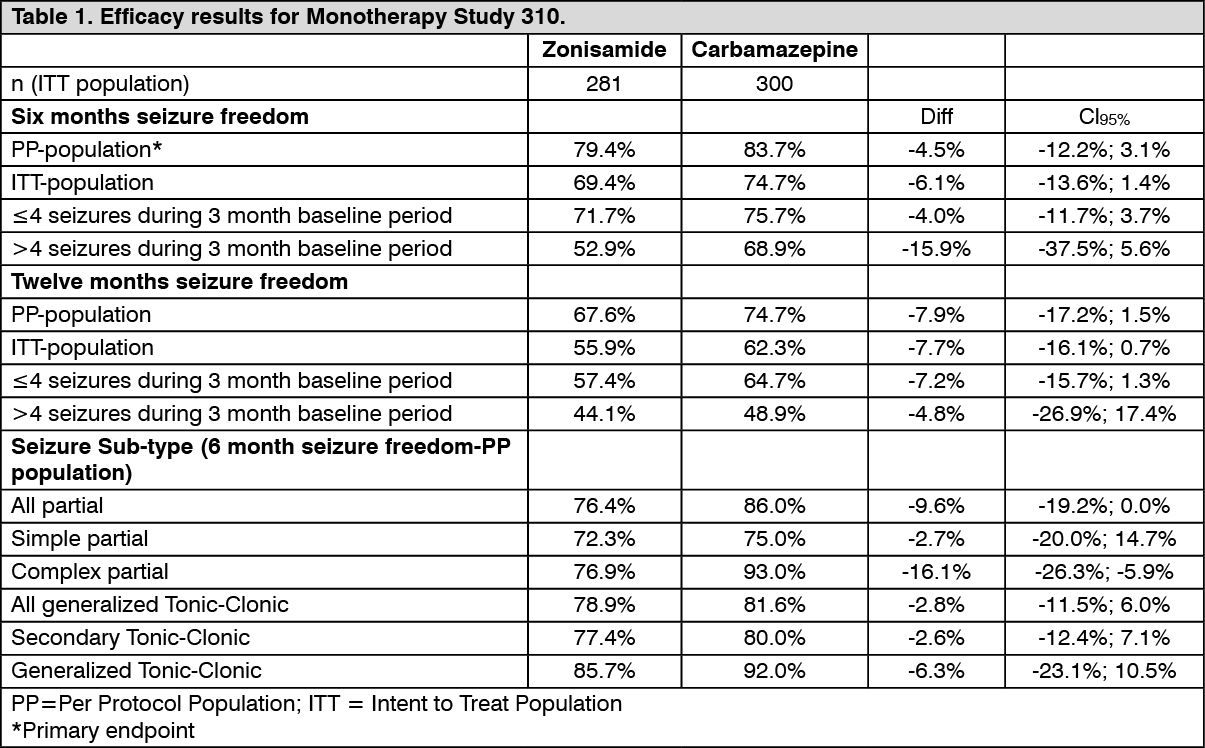
Clinical efficacy and safety: Monotherapy in partial seizures, with or without secondary generalisation: Efficacy of zonisamide as monotherapy was established in a double-blind, parallel group, non-inferiority comparison to carbamazepine prolonged release (PR) in 583 adult subjects with newly diagnosed partial seizures with or without secondary generalised tonic-clonic seizures. Subjects were randomised to carbamazepine and zonisamide received treatment for a duration of up to 24 months depending on response. Subjects were titrated to the initial target dose of 600 mg carbamazepine or 300 mg of zonisamide. Subjects who experienced a seizure were titrated to the next target dose i.e. 800 mg carbamazepine or 400 mg of zonisamide. Subjects who experienced a further seizure were titrated to the maximal target dose of 1200 mg carbamazepine or 500 mg zonisamide. Subjects who were seizure-free for 26 weeks at a target dose level continued on this dose for another 26 weeks.
Main outcomes of this study are presented in this table: See Table 1.
 Click on icon to see table/diagram/image
Paediatric population:
Click on icon to see table/diagram/image
Paediatric population: Adjunctive therapy in the treatment of partial seizures, with or without secondary generalization, in adolescent and paediatric patients (aged 6 years and above): In paediatric patients (aged 6 years and above), efficacy has been demonstrated with zonisamide in a double-blind, placebo-controlled study, which included 207 subjects and had a treatment duration of up to 24 weeks. A 50% or greater reduction from baseline in seizure frequency during the 12-week stable dose period was seen in 50% of the zonisamide-treated subjects and 31% of the patients on placebo.
Specific safety issues that were encountered in the paediatric studies were: decreased appetite and weight loss, decreased bicarbonate levels, increased risk of kidney stones and dehydration. All these effects and specifically weight loss may have deleterious implications for growth and development, and may lead to general deterioration of health. Altogether, data on effects on long-term growth and development are limited.
Pharmacokinetics: Absorption: Zonisamide is almost completely absorbed after oral administration, generally reaching peak serum or plasma concentrations within 2 to 5 hours of dosing. The first-pass metabolism is believed to be negligible. Absolute bioavailability is estimated to be approximately 100%. Oral bioavailability is not affected by food, although peak plasma and serum concentrations may be delayed.
Zonisamide AUC and C
max values increased almost linearly after single dose over the dose range of 100-800 mg and after multiple max doses over the dose range of 100-400 mg once daily. The increase at steady state was slightly more than expected on the basis of dose, probably due to the saturable binding of zonisamide to erythrocytes. Steady state was achieved within 13 days. Slightly greater than expected accumulation occurs relative to single dosing.
Distribution: Zonisamide is 40-50% bound to human plasma proteins, with
in vitro studies showing that this is unaffected by the presence of various antiepileptic medicinal products (i.e., phenytoin, phenobarbitone, carbamazepine, and sodium valproate). The apparent volume of distribution is about 1.1-1.7 L/kg in adults indicating that zonisamide is extensively distributed to tissues. Erythrocyte/plasma ratios are about 15 at low concentrations and about 3 at higher concentrations.
Biotransformation: Zonisamide is metabolised primarily through reductive cleavage of the benzisoxazole ring of the parent drug by CYP3A4 to form 2-sulphamoylacetylphenol (SMAP) and also by N-acetylation. Parent drug and SMAP can additionally be glucuronidated. The metabolites, which could not be detected in plasma, are devoid of anticonvulsant activity. There is no evidence that zonisamide induces its own metabolism.
Elimination: Apparent clearance of zonisamide at steady-state after oral administration is about 0.70 L/h and the terminal elimination half-life is about 60 hours in the absence of CYP3A4 inducers. The elimination half-life was independent of dose and not affected by repeat administration. Fluctuation in serum or plasma concentrations over a dosing interval is low (<30%). The main route of excretion of zonisamide metabolites and unchanged drug is via the urine. Renal clearance of unchanged zonisamide is relatively low (approximately 3.5 mL/min); about 15-30% of the dose is eliminated unchanged.
Linearity/non-linearity: Zonisamide exposure increases with time until steady state is achieved by approximately 8 weeks. When comparing the same dose level, subjects of higher total body weight appear to have lower steady-state serum concentrations, but this effect appears to be relatively modest. Age (≥ 12 years) and gender, after adjustment for body weight effects, have no apparent effect on zonisamide exposure in epileptic patients during steady-state dosing. There is no need for dose adjustment with any of the AEDs including CYP3A4 inducers.
Pharmacokinetic/pharmacodynamic relationship: Zonisamide lowers the 28-day average seizure frequency and the decrease is proportional (log-linear) to zonisamide average concentration.
Special patient groups: In subjects with renal impairment, renal clearance of single doses of zonisamide was positively correlated with creatinine clearance.
The plasma AUC of zonisamide was increased by 35% in subjects with creatinine clearance <20 mL/min.
Patients with an impaired liver function: The pharmacokinetics of zonisamide in patients with impaired liver function have not been adequately studied.
Elderly: No clinically significant differences were observed in the pharmacokinetics between young (aged 21-40 years) and elderly (65-75 years).
Children and adolescents (5-18 years): Limited data indicate that pharmacokinetics in children and adolescents dosed to steady state at 1, 7 or 12 mg/kg daily, in divided doses, are similar to those observed in adults, after adjustment for bodyweight.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image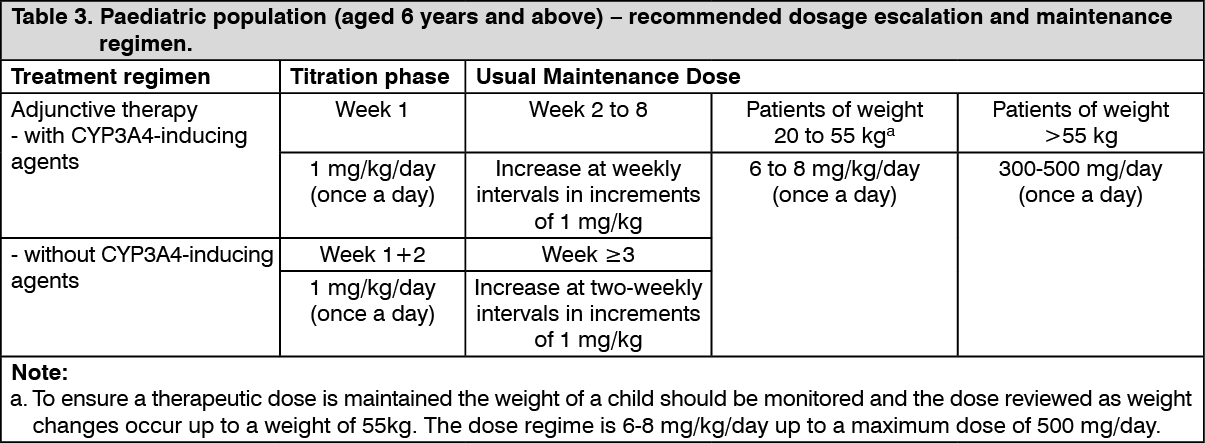 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image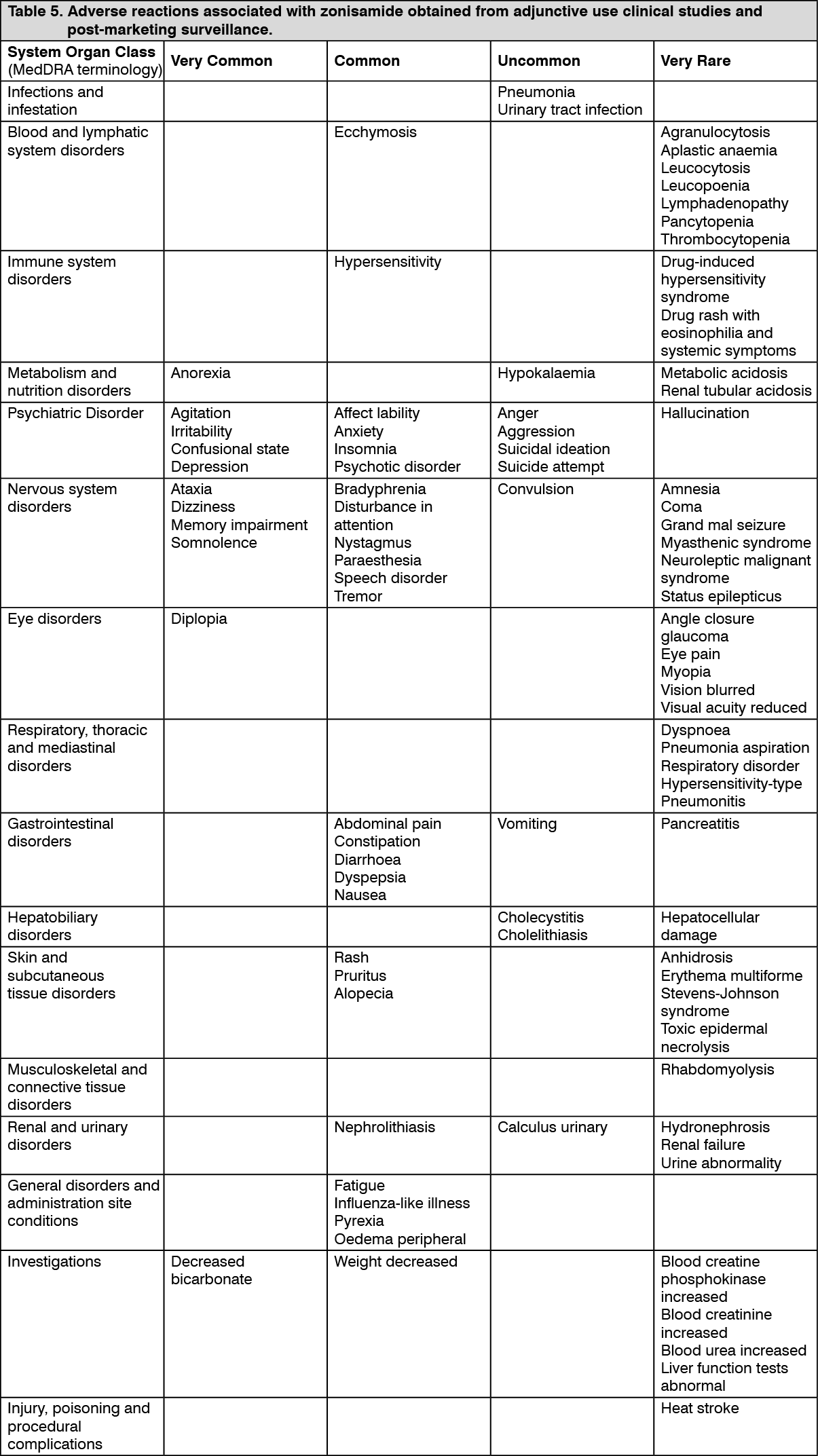 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image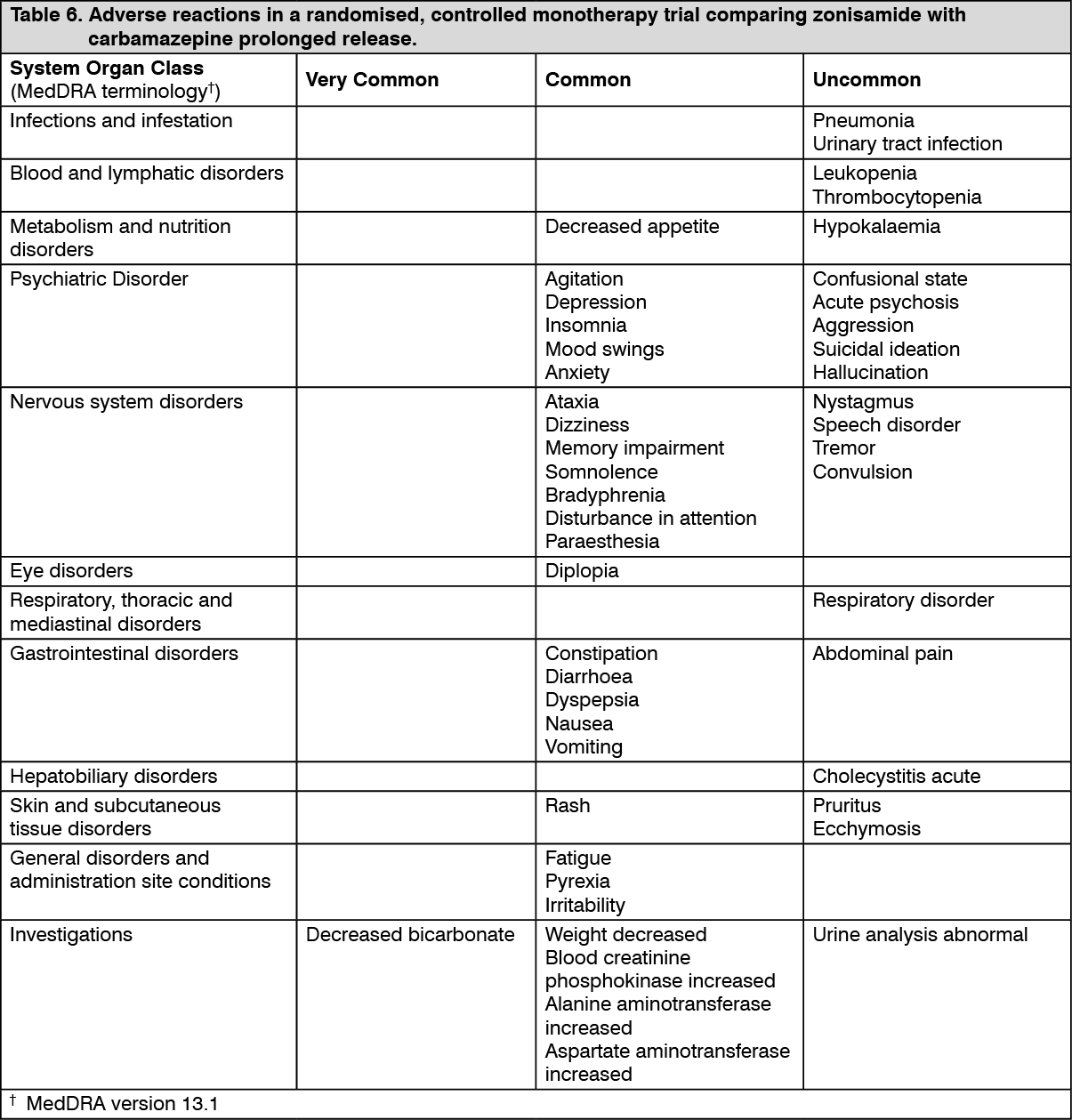 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out