Tablet: Adults: Treatment of Herpes Simplex: For treatment of herpes simplex infections, 200 mg Acyclovir (Zovirax) should be taken five times daily at approximately four-hourly intervals omitting the night time dose. Treatment should continue for five days but in severe initial infections may have to be extended.
In severely immune-compromised patients (e.g. after marrow transplant) or in patients with impaired absorption from the gut the dose can be doubled to 400 mg or, alternatively, intravenous dosing could be considered.
Dosing should begin as early as possible after the start of an infection; for recurrent episodes this should preferably be during the prodromal period or when lesions first appear.
Suppression of Herpes Simplex: For suppression of herpes simplex infections in immune-competent patients, 200 mg Acyclovir (Zovirax) should be taken four times daily at approximately six-hourly intervals.
Many patients may be conveniently managed on a regimen of 400 mg Acyclovir (Zovirax) taken twice daily at approximately twelve-hourly intervals.
Dosage titration down to 200 mg Acyclovir (Zovirax) taken thrice daily at approximately eight-hourly intervals or even twice daily at approximately twelve-hourly intervals, may prove effective.
Some patients may experience break-through infections on total daily doses of 800 mg Acyclovir (Zovirax).
Therapy should be interrupted periodically at intervals of six to twelve months in order to observe possible changes in the natural history of the disease.
Prophylaxis of Herpes Simplex: For prophylaxis of herpes simplex infections in immune-compromised patients, 200 mg Acyclovir (Zovirax) should be taken four times daily at approximately six-hourly intervals.
In severely immune-compromised patients (e.g. after marrow transplant) or in patients with impaired absorption from the gut the dose can be doubled to 400 mg or, alternatively, intravenous dosing could be considered.
The duration of prophylactic administration is determined by the duration of the period at risk.
Treatment of Varicella and Herpes Zoster: For treatment of varicella and herpes zoster infections, 800 mg Acyclovir (Zovirax) should be taken five times daily at approximately four-hourly intervals, omitting the night time dose. Treatment should continue for seven days.
In severely immune-compromised patients (e.g. after marrow transplant) or in patients with impaired absorption from the gut, consideration should be given to intravenous dosing.
Dosing should begin as early as possible after the start of an infection. Treatment yields better results if initiated as soon as possible after onset of the rash.
Management of Severely Immunocompromised Patients: For management of severely immunocompromised patients, 800 mg Acyclovir (Zovirax) should be taken four times daily at approximately six-hourly intervals.
In the management of bone marrow recipients this would normally be preceded by up to one month's therapy with intravenous Acyclovir (Zovirax) [see Acyclovir (Zovirax) IV for infusion prescribing information].
The duration of treatment studied in bone marrow transplant patients was 6 months (from 1 to 7 months post-transplant). In patients with advanced HIV disease, study treatment was 12 months, but it is likely that these patients would continue to benefit from a longer duration of treatment.
Infants and Children: For treatment of herpes simplex infections, and for prophylaxis of herpes simplex infections in the immune-compromised, children aged two years and over should be given adult dosages and infants and children below the age of two years should be given half the adult dose.
For treatment of varicella infections in children:
6 years and over: 800 mg Acyclovir (Zovirax) four times daily;
2-<6 years: 400 mg Acyclovir (Zovirax) four times daily;
Under 2 years: 200 mg Acyclovir (Zovirax) four times daily. Dosing may be more accurately calculated as 20 mg Acyclovir (Zovirax)/kg bodyweight (not to exceed 800 mg) four times daily. Treatment should continue for five days.
No specific data are available on the suppression of herpes simplex infections or the treatment of herpes zoster infections in immune-competent children.
Limited data suggest that for management of severely immunocompromised children, over two years of age, the adult dose may be given.
Elderly: The possibility of renal impairment in the elderly must be considered and the dosage should be adjusted accordingly (see Renal Impairment as follows).
Adequate hydration of elderly patients taking high oral doses of Acyclovir (Zovirax) should be maintained.
Renal Impairment: Caution is advised when administering Acyclovir (Zovirax) oral formulations to patients with impaired renal function. Adequate hydration should be maintained.
In the treatment and prophylaxis of herpes simplex infections in patients with impaired renal function, the recommended oral doses will not lead to accumulation of acyclovir above levels that have been established safe by intravenous infusion. However, for patients with severe renal impairment (creatinine clearance less than 10 ml/minute) an adjustment of dosage to 200 mg twice daily at approximately twelve-hourly intervals is recommended.
In the treatment of varicella and herpes zoster infections, and in the management of severely immunocompromised patients it is recommended to adjust the dosage to 800 mg twice daily, at approximately twelve-hourly intervals, for patients with severe renal impairment (creatinine clearance less than 10 mL/minute) and to 800 mg three times daily, at intervals of approximately eight hours, for patients with moderate renal impairment (creatinine clearance in the range 10 to 25 mL/minute).
Injection: To be gives as intravenous infusion over 1 hour.
A course of treatment with Acyclovir (Zovirax) IV for infusion usually lasts 5 days, but this may be adjusted according to the patient's condition and response to therapy. Treatment for herpes encephalitis usually lasts 10 days.
Treatment for neonatal herpes usually lasts 14-21 days.
The duration of prophylactic administration of Acyclovir (Zovirax) IV for infusion is determined by the duration of the period at risk.
Adults: Treatment of Herpes Simplex: Obese patients should be dosed at the recommended adult dose using ideal body weight, rather than actual body weight.
Patients with herpes simplex (except herpes encephalitis) should be given acyclovir IV for infusion in doses of 5 mg/kg bodyweight every eight hours if renal function is not impaired.
Patients with herpes encephalitis should be given acyclovir IV for infusion in doses of 10 mg/kg bodyweight every eight hours provided renal function is not impaired.
Prophylaxis of Herpes Simplex in Immune-compromised Patients: Obese patients should be dosed at the recommended adult dose using ideal body weight, rather than actual body weight.
Refer to adult dosing recommendations for the treatment of herpes simplex with Acyclovir (Zovirax) IV for infusion.
Treatment of Varicella and Herpes Zoster: Obese patients should be dosed at the recommended adult dose using ideal body weight, rather than actual body weight.
Patients with varicella zoster infections should be given acyclovir IV for infusion in doses of 5 mg/kg bodyweight every eight hours if renal function is not impaired.
Immune-compromised patients with varicella zoster infections should be given acyclovir IV for infusion in doses of 10 mg/kg bodyweight every eight hours provided renal function is not impaired.
Infants and Children: The dose of Acyclovir (Zovirax) IV for infusion for infants and children aged between 3 months and 12 years is calculated on the basis of body surface area. Infants and children 3 months of age or older with herpes simplex (except herpes encephalitis) or varicella zoster infections should be given Acyclovir (Zovirax) IV for infusion in doses of 250 mg per square metre body surface area every 8 hours if renal is not impaired.
In immune-compromised infants and children with varicella zoster infections or herpes encephalitis, Acyclovir (Zovirax) IV for infusion should be given in doses of 500 mg per square metre body surface area every 8 hours if renal function is not impaired.
Infants and children with impaired renal function require an appropriately modified dose, according to the degree of impairment.
Neonates: The dosage of Acyclovir (Zovirax) IV for infusion in neonates is calculated on the basis of bodyweight.
The recommended regimen for treatment for known or suspected neonatal herpes is Acyclovir (Zovirax) IV 20 mg/kg body weight IV every 8 hours for 21 days for disseminated and CNS disease, or for 14 days for disease limited to the skin and mucous membranes. Patients with impaired renal function require an appropriately modified dose, according to the degree of impairment (see Renal Impairment).
Elderly: The possibility of renal impairment in the elderly must be considered and the dosage should be adjusted accordingly (see Renal Impairment).
Adequate hydration should be maintained.
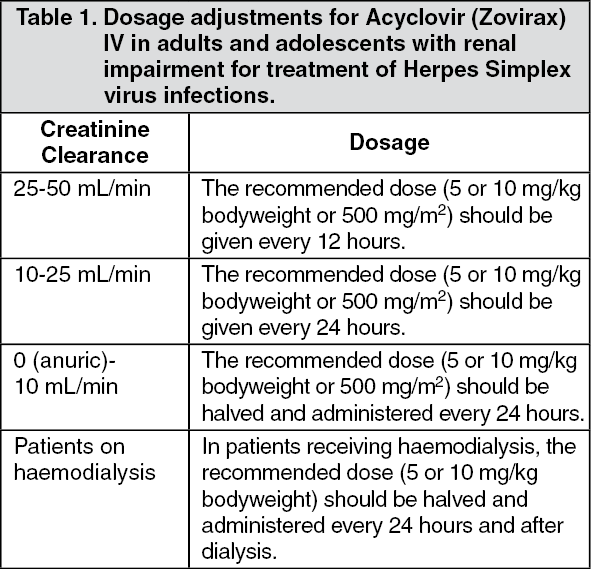
Renal Impairment: Caution is advised when administering Acyclovir (Zovirax) IV for infusion to patients with impaired renal function. Adequate hydration should be maintained.
Dosage adjustment for patients with renal impairment is based on creatinine clearance, in units of mL/min for adults and adolescents and in units of mL/min/1.73 m
2 for infants and children less than 13 years of age. The following adjustments in dosage are suggested: See Tables 1 and 2.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image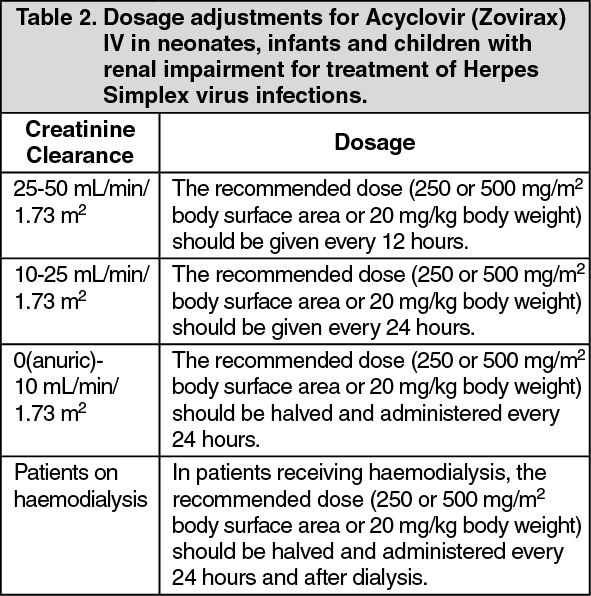 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image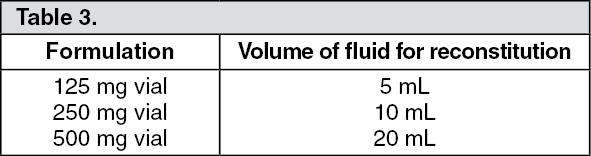 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out