


 Sign Out
Sign Out

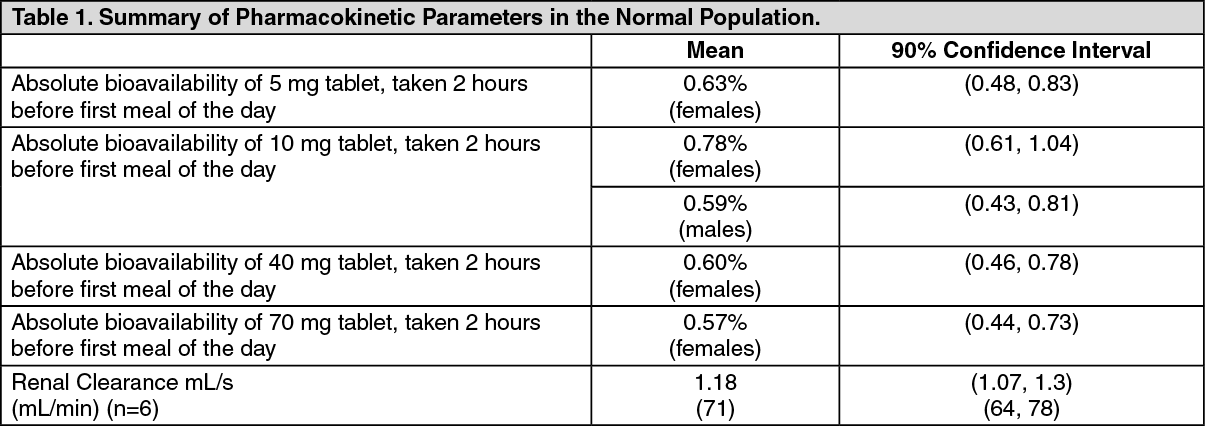
Pharmacokinetics: Absorption: Relative to an intravenous (IV) reference dose, the mean oral bioavailability of alendronate in women was 0.64% for doses ranging from 5 to 70 mg when administered after an overnight fast and two hours before a standardized breakfast. Oral bioavailability of the 10 mg tablet in men was 0.59%.
A study examining the effect of timing of a meal on the bioavailability of alendronate was performed in 49 postmenopausal women. Bioavailability was decreased (by approximately 40%) when 10 mg alendronate was administered either 0.5 or 1 hour before a standardized breakfast, when compared to dosing 2 hours before eating. In studies of treatment and prevention of osteoporosis, alendronate was effective when administered at least 30 minutes before breakfast.
Bioavailability was negligible whether alendronate was administered with or up to two hours after a standardized breakfast. Concomitant administration of alendronate with coffee or orange juice reduced bioavailability by approximately 60%.
In healthy subjects, oral prednisone (20 mg three times daily for five days) did not produce a clinically meaningful change in the oral bioavailability of alendronate (a mean increase ranging from 20 to 44%).
Distribution: Preclinical studies (in male rats) show that alendronate transiently distributes to soft tissues following 1 mg/kg IV administration but is then rapidly redistributed to bone or excreted in the urine. The mean steady-state volume of distribution, exclusive of bone, is at least 28 L in humans. Concentrations of drug in plasma following therapeutic oral doses are too low (less than 5 ng/mL) for analytical detection. Protein binding in human plasma is approximately 78%.
Metabolism: There is no evidence that alendronate is metabolized in animals or humans.
Excretion: Following a single IV dose of [14C]alendronate, approximately 50% of the radioactivity was excreted in the urine within 72 hours and little or no radioactivity was recovered in the feces. Following a single 10 mg IV dose, the renal clearance of alendronate was 71 mL/min and systemic clearance did not exceed 200 mL/min. Plasma concentrations fell by more than 95% within 6 hours following IV administration. The terminal half-life in humans is estimated to exceed 10 years, probably reflecting release of alendronate from the skeleton. Based on the previous text, it is estimated that after 10 years of oral treatment with alendronate (10 mg daily), the amount of alendronate released daily from the skeleton is approximately 25% of that absorbed from the gastrointestinal tract.
Special Populations: Pediatric: Alendronate pharmacokinetics have not been investigated in patients <18 years of age.
Gender: Bioavailability and the fraction of an IV dose excreted in urine were similar in men and women.
Geriatric: Bioavailability and disposition (urinary excretion) were similar in elderly (>65 years of age) and younger patients. No dosage adjustment is necessary (see DOSAGE & ADMINISTRATION).
Race: Pharmacokinetic differences due to race have not been studied.
Renal Insufficiency: Preclinical studies show that, in rats with kidney failure, increasing amounts of drug are present in plasma, kidney, spleen, and tibia. In healthy controls, drug that is not deposited in bone is rapidly excreted in the urine. No evidence of saturation of bone uptake was found after 3 weeks dosing with cumulative IV doses of 35 mg/kg in young male rats. Although no clinical information is available, it is likely that, as in animals, elimination of alendronate via the kidney will be reduced in patients with impaired renal function. Therefore, somewhat greater accumulation of alendronate in bone might be expected in patients with impaired renal function.
No dosage adjustment is necessary for patients with mild-to-moderate renal insufficiency [creatinine clearance 0.58 to 1 mL/s (35 to 60 mL/min)]. APO-ALENDRONATE is not recommended for patients with more severe renal insufficiency [creatinine clearance <0.58 mL/s (<35 mL/min)] due to lack of experience.
Hepatic Insufficiency: As there is evidence that alendronate is not metabolized or excreted in the bile, no studies were conducted in patients with hepatic insufficiency. No dosage adjustment is necessary.
Drug Interactions (see Interactions): Intravenous ranitidine was shown to double the bioavailability of oral alendronate. The clinical significance of this increased bioavailability and whether similar increases will occur in patients given oral H2-antagonists is unknown; no other specific drug interaction studies were performed.
Products containing calcium and other multivalent cations likely will interfere with absorption of alendronate. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacodynamics: Alendronate is a bisphosphonate that binds to bone hydroxyapatite and specifically inhibits the activity of osteoclasts, the bone resorbing cells. Alendronate reduces bone resorption with no direct effect on bone formation, although the latter process is ultimately reduced because bone resorption and formation are coupled during bone turnover.
Osteoporosis in Postmenopausal Women: Osteoporosis is characterized by low bone mass that leads to an increased risk of fracture. The diagnosis can be confirmed by the finding of low bone mass, evidence of fracture on x-ray, a history of osteoporotic fracture, or height loss or kyphosis, indicative of vertebral fracture. Osteoporosis occurs in both males and females but is most common among women following the menopause, when bone turnover increases and the rate of bone resorption exceeds that of bone formation. These changes result in progressive bone loss and lead to osteoporosis in a significant proportion of women over age 50. Fractures, usually of the spine, hip, and wrist, are the common consequences. From age 50 to age 90, the risk of hip fracture in white women increases 50-fold and the risk of vertebral fracture 15- to 30-fold. It is estimated that approximately 40% of 50-year-old women will sustain one or more osteoporosis-related fractures of the spine, hip, or wrist during their remaining lifetimes. Hip fractures, in particular, are associated with substantial morbidity, disability, and mortality.
Daily oral doses of alendronate (5, 20, and 40 mg for six weeks) in postmenopausal women produced biochemical changes indicative of dose-dependent inhibition of bone resorption, including decreases in urinary calcium and urinary markers of bone collagen degradation (such as deoxypyridinoline and cross-linked N-telopeptides of type I collagen). These biochemical changes tended to return toward baseline values as early as 3 weeks following the discontinuation of therapy with alendronate and did not differ from placebo after 7 months.
Long-term treatment of osteoporosis with alendronate 10 mg/day (for up to five years) reduced urinary excretion of markers of bone resorption, deoxypyridinoline and cross-linked N-telopeptides of type I collagen, by approximately 50% and 70%, respectively, to reach levels similar to those seen in healthy premenopausal women. Similar decreases were seen in patients in osteoporosis prevention studies who received alendronate 5 mg/day. The decrease in the rate of bone resorption indicated by these markers was evident as early as one month and at three to six months reached a plateau that was maintained for the entire duration of treatment with alendronate. In osteoporosis treatment studies, alendronate 10 mg/day decreased the markers of bone formation, osteocalcin and bone specific alkaline phosphatase by approximately 50%, and total serum alkaline phosphatase, by approximately 25 to 30%, to reach a plateau after 6 to 12 months. In osteoporosis prevention studies, alendronate 5 mg/day decreased osteocalcin and total serum alkaline phosphatase by approximately 40% and 15%, respectively. Similar reductions in the rate of bone turnover were observed in postmenopausal women during a one year study with alendronate 70 mg once weekly for the treatment of osteoporosis. These data indicate that the rate of bone turnover reached a new steady-state, despite the progressive increase in the total amount of alendronate deposited within bone.
As a result of inhibition of bone resorption, asymptomatic reductions in serum calcium and phosphate concentrations were also observed following treatment with alendronate. In the long term studies, reductions from baseline in serum calcium (approximately 2%) and phosphate (approximately 4 to 6%) were evident the first month after the initiation of alendronate 10 mg. No further decreases in serum calcium were observed for the five-year duration of treatment, however, serum phosphate returned toward prestudy levels during years three through five.
Similar reductions were observed with alendronate 5 mg/day. In a one-year study with alendronate 70 mg once weekly, similar reductions were observed at 6 and 12 months. The reduction in serum phosphate may reflect not only the positive bone mineral balance due to alendronate but also a decrease in renal phosphate reabsorption.
Osteoporosis in Men: Even though osteoporosis is less prevalent in men than in postmenopausal women, a significant proportion of osteoporotic fractures occur in men. The prevalence of vertebral deformities appears to be similar in men and women. Treatment of men with osteoporosis with alendronate 10 mg/day for two years reduced urinary excretion of cross-linked N-telopeptides of type I collagen by approximately 60% and bone-specific alkaline phosphatase by approximately 40%. Similar reductions were observed in a one-year study in men receiving alendronate 70 mg once weekly.
Glucocorticoid-Induced Osteoporosis: Sustained use of glucocorticoids is commonly associated with development of osteoporosis and resulting fractures (especially vertebral, hip, and rib). It occurs both in males and females of all ages. Osteoporosis occurs as a result of inhibited bone formation and increased bone resorption resulting in net bone loss. Alendronate decreases bone resorption without directly inhibiting bone formation.
In clinical studies of up to two years' duration, alendronate 5 and 10 mg/day reduced cross-linked N-telopeptides of type 1 collagen (a marker of bone resorption) by approximately 60% and reduced bone-specific alkaline phosphatase and total serum alkaline phosphatase (markers of bone formation) by approximately 15 to 30% and 8 to 18%, respectively. As a result of inhibition of bone resorption, alendronate 5 and 10 mg/day induced asymptomatic decreases in serum calcium (approximately 1 to 2%) and serum phosphate (approximately 1 to 8%).
Paget's Disease of Bone: Paget's disease of bone is a chronic, focal skeletal disorder characterized by greatly increased and disorderly bone remodeling. Excessive osteoclastic bone resorption is followed by osteoblastic new bone formation, leading to the replacement of the normal bone architecture by disorganized, enlarged, and weakened bone structure.
Clinical manifestations of Paget's disease range from no symptoms to severe morbidity due to bone pain, bone deformity, pathological fractures, and neurological and other complications. Serum alkaline phosphatase, the most frequently used biochemical index of disease activity, provides an objective measure of disease severity and response to therapy.
Alendronate decreases the rate of bone resorption directly, which leads to an indirect decrease in bone formation. In clinical trials, alendronate 40 mg once daily for six months produced significant decreases in serum alkaline phosphatase as well as in urinary markers of bone collagen degradation. As a result of the inhibition of bone resorption, alendronate induced generally mild, transient, and asymptomatic decreases in serum calcium and phosphate.