Each PR tab contains 10 mg alfuzosin hydrochloride.
Excipients/Inactive Ingredients: Dibasic calcium phosphate dihydrate, hydroxypropyl methylcellulose, magnesium stearate, polyvinyl acetate phthalate, and yellow ferric oxide.
Pharmacotherapeutic Group: Alpha-Blockers. ATC code: G04CA01(G: genitourinary system and sex hormones).
Pharmacology: Pharmacodynamics: Alfuzosin is a quinazoline derivative, active by the oral route. It is an uroselective antagonist of post-synaptic α1-adrenoceptors located in the prostate, bladder base, bladder neck, prostatic capsule, and prostatic urethra.
Alfuzosin hydrochloride blocks α1-adrenoceptors leading to a relaxation of the smooth muscle in the bladder neck and prostate.
In animal studies, alfuzosin was shown to be functionally uroselective by preferentially decreasing urethral blood pressure over arterial blood pressure. In human tissue, in vitro, alfuzosin has induced preferential α1-adrenoceptor antagonist activity on prostatic cells relative to renal artery cells.
In placebo-controlled clinical studies in patients with BPH, alfuzosin hydrochloride was shown to: significantly increase urine peak flow rate (Qmax) by 30% which is observed after the first dose; significantly reduce detrusor pressure and increase bladder capacity; significantly reduce residual urine volume.
These favourable urodynamic effects lead to an improvement of lower tract irritative and obstructive symptoms without any deleterious effect on sexual function.
In the ALFAUR study, the effect of alfuzosin on return to voiding was assessed in 357 men over the age of 50 presenting a first painful episode of acute urinary retention (AUR) related to benign prostatic hypertrophy (BPH) with a residual urine volume of between 500 and 1500 ml following insertion of a catheter and for the first hour after catheterisation. In this multicentre, randomised, doubleblind study in two parallel groups comparing 10 mg/day alfuzosin LP with placebo, evaluation of return to voiding was conducted 24 hours after removal of the catheter, in the morning, after at least two days of alfuzosin treatment. Treatment with alfuzosin significantly increased (p = 0.012) the rate of return to voiding after catheter removal in patients having suffered a first episode of AUR, i.e. 146 returns to voiding (61.9%) in the alfuzosin group versus 58 (47.9%) in the placebo group.
Pharmacokinetics: Bioavailability is reduced when alfuzosin hydrochloride is administered under fasting conditions.
Alfuzosin hydrochloride is moderately bound to plasma proteins with the free fraction accounting for 13.3% in healthy volunteers.
Alfuzosin hydrochloride undergoes metabolism by the liver, with only 11% of the parent compound being excreted as unchanged in the urine. The metabolites which are all inactive are eliminated in the urine (15-30%) and feces (75-91%). Most of the metabolites (which are inactive) are excreted in the faeces (75 to 90%).
Following intravenous or oral administration, the elimination of alfuzosin hydrochloride is characterized, in healthy young subjects and in the target population, by a terminal half-life of about 4.8 hours and a total clearance of 0.3 L/h/kg.
The apparent half-life of alfuzosin hydrochloride is increased to 9.1 hours in healthy middle aged volunteers and to 10.1 hours in elderly volunteers.
Compared to healthy middle-aged volunteers, the pharmacokinetic parameters of alfuzosin hydrochloride (Cmax and AUC) are not increased in elderly patients.
The pharmacokinetic profile of alfuzosin is not modified in the event of chronic heart failure.
Compared to subjects with normal renal function, the mean Cmax and AUC values of alfuzosin hydrochloride are moderately increased (1.5 to 1.6 fold) in patients with various stages of renal impairment, with no change in the apparent elimination half-life. This change in the pharmacokinetic profile is not considered clinically relevant; and therefore, does not necessitate a dosing adjustment. Alfuzosin hydrochloride prolonged-release tablet has not been evaluated in patients with end-stage renal disease.
Treatment of the functional symptoms of benign prostatic hypertrophy (BPH). Adjuvant treatment to a catheter in first episode of acute urinary retention (AUR) related to benign prostatic hypertrophy (BPH).
Benign Prostatic Hyperplasia: The recommended dosage is one 10 mg APO-ALFUZOSIN (alfuzosin hydrochloride) tablet daily to be taken after the same meal each day.
Adjuvant treatment to a catheter in the first episode of acute urinary retention related to benign prostatic hypertrophy: The recommended dosage is one 10 mg APO-ALFUZOSIN tablet daily after a meal to be taken from the first day of catheterization onwards.
The treatment is administered for 3 to 4 days, i.e. 2 to 3 days while the catheter is in place and 1 day after it is removed.
Administration: The tablet must be swallowed whole with a glass of water (see Precautions). Any other mode of administration, such as crunching, crushing, chewing, grinding or pounding to powder should be prohibited. These actions may lead to an inappropriate release and absorption of the drug and therefore possible early adverse reactions.
Should overdose of APO-ALFUZOSIN (alfuzosin hydrochloride) lead to hypotension, support of the cardiovascular system is of first importance. Restoration of blood pressure and normalization of heart rate may be accomplished by keeping the patient in the supine position.
Alfuzosin hydrochloride is 87% (82 - 90%) protein-bound, therefore, dialysis may not be of benefit.
APO-ALFUZOSIN (alfuzosin hydrochloride) is contraindicated in: hypersensitivity to alfuzosin and/or any of the other ingredients, postural hypotension, liver failure, severe kidney failure (creatinine clearance <30 ml/min), in combination with potent CYP3A4 inhibitors such as ketoconazole, ritonavir and itraconazole.
As with all alpha-1 blockers, some patients, and in particular those treated with antihypertensives may experience postural hypotension within a few hours following administration, possibly with symptoms (dizzy sensations, fatigue, sweating). If this occurs, patient should remain lying down until the symptoms have completely subsided. These effects are usually transient, occur at the beginning of treatment and do not generally prevent continued treatment. Pronounced drop in blood pressure has been reported in post-marketing surveillance in patients with pre-existing risk factors (such as underlying cardiac diseases and/or concomitant treatment with anti-hypertensive medication). Patients should be warned of the possible occurrence of these events. The risk of developing hypotension and related adverse reactions may be greater in elderly patients.
Treatment should be initiated gradually in patients with hypersensitivity to alpha-1 blockers.
APO-ALFUZOSIN 10 mg tablets should be administered carefully to patients being treated with antihypertensives.
Blood pressure should be monitored regularly, especially at the beginning of the treatment.
Caution is recommended, particularly in the elderly.
Use with caution in patients with acquired or congenital QT prolongation or who are taking medications that prolong the QT interval.
Intraoperative Floppy Iris Syndrome (IFIS, a small pupil syndrome variant) has been observed during cataract surgery in some patients previously or currently treated with tamsulosin. Isolated cases have also been reported with other alpha-1 blockers, therefore a possible class effect cannot be ruled out. Considering that IFIS can be the cause of additional technical difficulties during cataract operations, the surgeons must be informed of any history of current use of alpha-1 blockers before the eye surgery.
Care should be taken when alfuzosin is administered to patients who have experienced marked hypotension following administration of another alpha-1 blocker.
In patients with coronary disease, alfuzosin should not be prescribed alone.
The specific coronary insufficiency treatment should be continued. If angina pectoris recurs or worsens, alfuzosin treatment should be discontinued.
Patients must be informed that the tablets must be swallowed whole. The tablets must not be crunched, chewed, crushed or ground into a powder.
Doing so could lead to inappropriate release and absorption of the medicinal product consequently causing unwanted effects which may be of early onset.
Effects on ability to drive and use machines: Caution is required when driving vehicles or using machines due to the risks of postural hypotension, dizziness, asthenia, visual disturbances, especially at the start of treatment with alfuzosin.
APO-ALFUZOSIN is not indicated nor recommended for use in women. The safety of alfuzosin during pregnancy and its passage into breast milk are unknown.
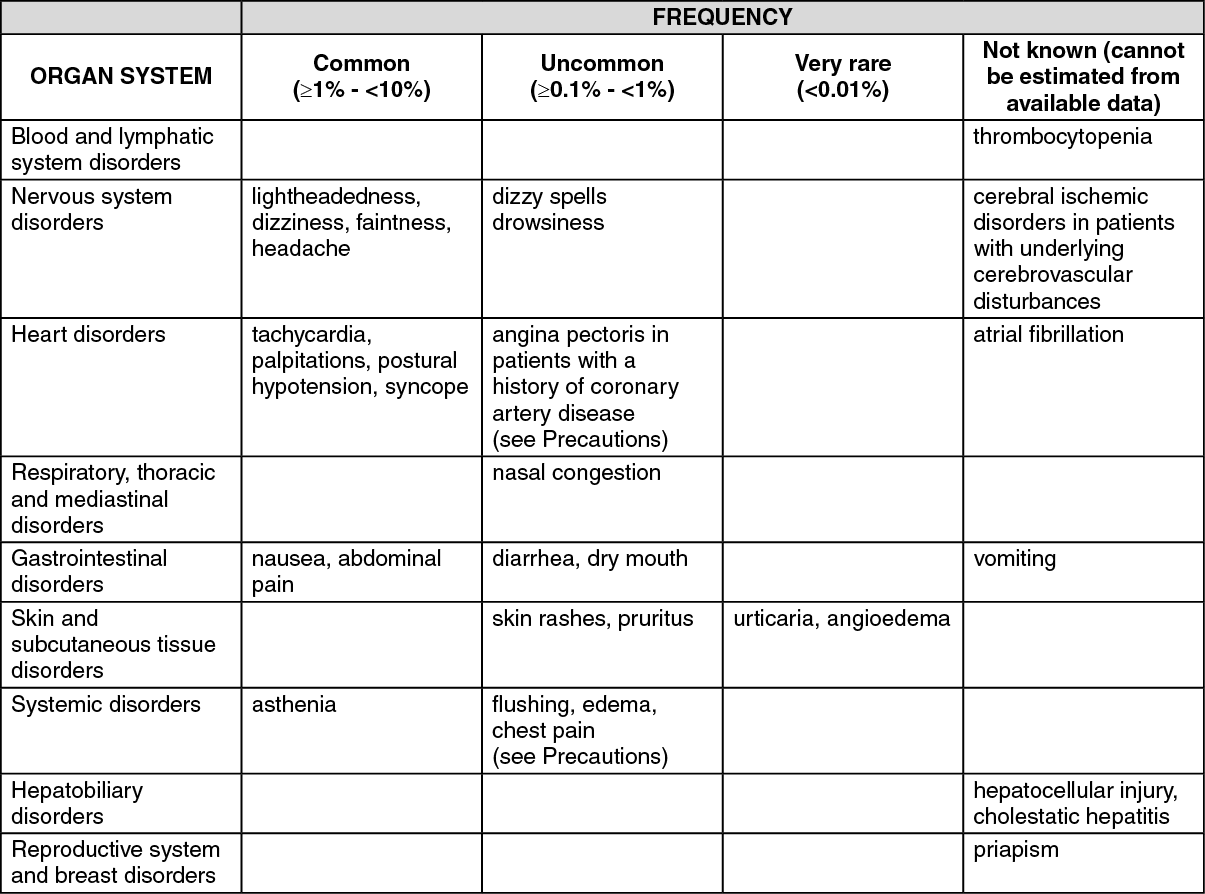
(See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
APO-ALFUZOSIN (alfuzosin hydrochloride) is not an inducer or an inhibitor of any of the principal hepatic enzymes involved in the metabolism of other drugs.
CYP3A4 is the principal hepatic enzyme iso-form involved in the metabolism of APO-ALFUZOSIN.
Potent CYP3A4 inhibitors, such as ketoconazole, itraconazole and ritonavir, increased alfuzosin hydrochloride blood levels and exposure (AUC).
Therefore, APO-ALFUZOSIN should not be co-administered with potent inhibitors of CYP3A4.
It is not known how combined exposure of any medications metabolized by the CYP3A4 hepatic enzyme isoform (such as modern alpha1-blockers), herbal remedies (particularly St. John's Wort, Milk thistle) and grapefruit juice may influence the overall efficacy and unwanted side effects of these medications, therefore, caution should be exercised.
Contraindicated combination: Ritonavir: Risk of increased plasma alfuzosin concentrations and increased undesirable effects.
Unadvised combination: Anti-hypertensive alpha-receptor blockers (prazosin, trimazosin, urapidil): Enhance hypotensive effect. Risk of severe postural hypotension.
Ketoconazole, itraconazole: Risk of increased plasma alfuzosin concentrations and increased undesirable effects.
Clarithromycin, erythromycin: Risk of increased plasma alfuzosin concentrations and increased undesirable effects.
Combination requiring precautions for use: Phosphodiesterase type 5 inhibitors (sildenafil, tadalafil, vardenafil): Risk of postural hypotension, particularly in elderly subjects. Treatment should be initiated at the lowest recommended dose and adjusted gradually if necessary.
Combination to be taken into consideration: Antihypertensives except alpha-receptor blockers: Enhanced hypotensive effect. Higher risk of postural hypotension.
Nitrates, nitrites and related drugs (isosorbide dinitrate, isosorbide, linsidomine, molsidomine, nicorandil, nitroglycerin): Increased risk of hypotension, particularly postural.
G04CA01 - alfuzosin ; Belongs to the class of alpha-adrenoreceptor antagonists. Used in the treatment of benign prostatic hypertrophy.
Apo-Alfuzosin PR tab 10 mg
100's




 Sign Out
Sign Out