


 Sign Out
Sign Out


Pharmacology: Pharmacodynamics: Mechanism of action: Sugammadex is a modified gamma cyclodextrin which is a Selective Relaxant Binding Agent. It forms a complex with the neuromuscular blocking agents rocuronium or vecuronium in plasma and thereby reduces the amount of neuromuscular blocking agent available to bind to nicotinic receptors in the neuromuscular junction. This results in the reversal of neuromuscular blockade induced by rocuronium or vecuronium.
Pharmacodynamic effects: Sugammadex has been administered in doses ranging from 0.5 mg/kg to 16 mg/kg in dose response studies of rocuronium induced blockade (0.6, 0.9, 1.0 and 1.2 mg/kg rocuronium bromide with and without maintenance doses) and vecuronium induced blockade (0.1 mg/kg vecuronium bromide with or without maintenance doses) at different time points/depths of blockade. In these studies a clear dose-response relationship was observed.
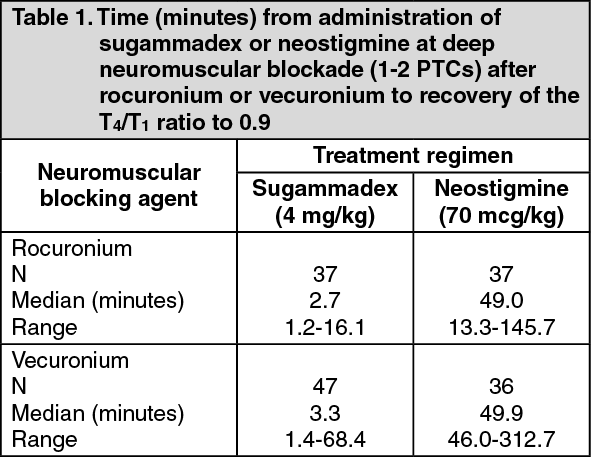
Clinical efficacy and safety: Sugammadex can be administered at several time points after administration of rocuronium or vecuronium bromide: Routine reversal - deep neuromuscular blockade: In a pivotal study patients were randomly assigned to the rocuronium or vecuronium group. After the last dose of rocuronium or vecuronium, at 1-2 PTCs, 4 mg/kg sugammadex or 70 mcg/kg neostigmine was administered in a randomised order. The time from start of administration of sugammadex or neostigmine to recovery of the T4/T1 ratio to 0.9 was: (See Table 1.)
 Click on icon to see table/diagram/image
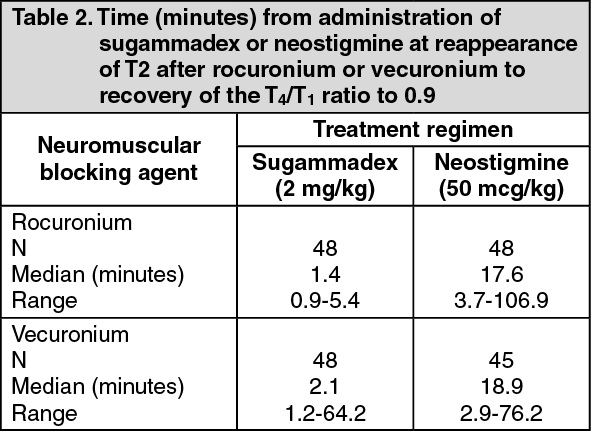
Click on icon to see table/diagram/imageRoutine reversal - moderate neuromuscular blockade: In another pivotal study patients were randomly assigned to the rocuronium or vecuronium group. After the last dose of rocuronium or vecuronium, at the reappearance of T2, 2 mg/kg sugammadex or 50 mcg/kg neostigmine was administered in a randomised order. The time from start of administration of sugammadex or neostigmine to recovery of the T4/T1 ratio to 0.9 was: (See Table 2.)
 Click on icon to see table/diagram/image
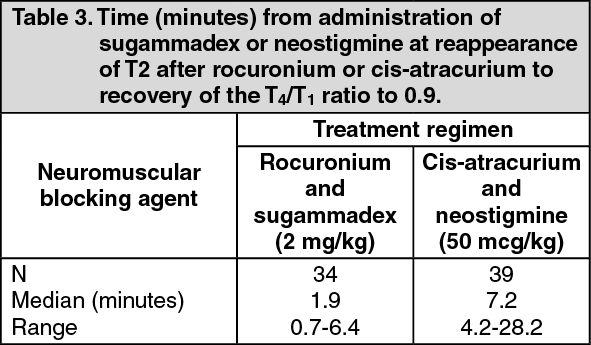
Click on icon to see table/diagram/imageReversal by sugammadex of the neuromuscular blockade induced by rocuronium was compared to the reversal by neostigmine of the neuromuscular blockade induced by cis-atracurium. At the reappearance of T2 a dose of 2 mg/kg sugammadex or 50 mcg/kg neostigmine was administered. Sugammadex provided faster reversal of neuromuscular blockade induced by rocuronium compared to neostigmine reversal of neuromuscular blockade induced by cis-atracurium: (See Table 3.)
 Click on icon to see table/diagram/image
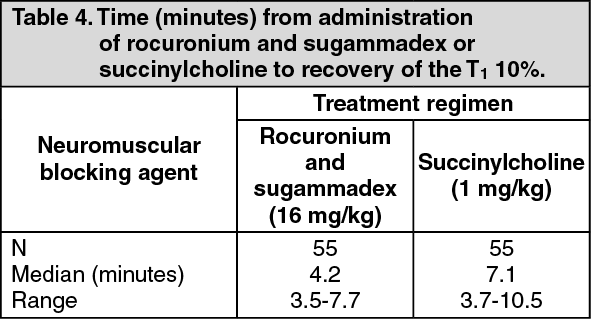
Click on icon to see table/diagram/imageFor immediate reversal: The time to recovery from succinylcholine-induced neuromuscular blockade (1 mg/kg) was compared with sugammadex (16 mg/kg, 3 minutes later) - induced recovery from rocuronium-induced neuromuscular blockade (1.2 mg/kg). (See Table 4.)
 Click on icon to see table/diagram/image
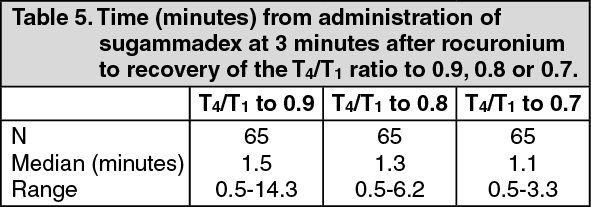
Click on icon to see table/diagram/imageIn a pooled analysis the following recovery times for 16 mg/kg sugammadex after 1.2 mg/kg rocuronium bromide were reported: (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageEffects on QTc-interval: In three dedicated clinical studies (N=287) sugammadex alone, sugammadex in combination with rocuronium or vecuronium and sugammadex in combination with propofol or sevoflurane was not associated with clinically relevant QT/QTc prolongation. The integrated ECG and adverse event results of Phase 2-3 studies support this conclusion.
Morbidly obese patients: A trial of 188 patients who were diagnosed as morbidly obese (body mass index ≥ 40 kg/m2) investigated the time to recovery from moderate or deep neuromuscular blockade induced by rocuronium or vecuronium. Patients received 2 mg/kg or 4 mg/kg sugammadex, as appropriate for level of block, dosed according to either actual body weight or ideal body weight in random, double-blinded fashion. Pooled across depth of block and neuromuscular blocking agent, the median time to recover to a train-of-four (TOF) ratio ≥ 0.9 in patients dosed by actual body weight (1.8 minutes) was statistically significantly faster (p < 0.0001) compared to patients dosed by ideal body weight (3.3 minutes).
Patients with severe systemic disease: A trial of 331 patients who were assessed as ASA Class 3 or 4 investigated the incidence of treatment-emergent arrhythmias (sinus bradycardia, sinus tachycardia, or other cardiac arrhythmias) after administration of sugammadex.
In patients receiving sugammadex (2 mg/kg, 4 mg/kg, or 16 mg/kg), the incidence of treatment-emergent arrhythmias was generally similar to neostigmine (50 µg/kg up to 5 mg maximum dose) + glycopyrrolate (10 µg/kg up to 1 mg maximum dose). The percentage of patients with treatment-emergent sinus bradycardia was significantly lower (p=0.026) in the sugammadex 2 mg/kg group compared with the neostigmine group. The percentage of patients with treatment-emergent sinus tachycardia was significantly lower in the sugammadex 2 mg/kg and 4 mg/kg groups compared with the neostigmine group (p=0.007 and 0.036, respectively). The safety profile in ASA Class 3 and 4 patients was generally similar to that of adult patients in pooled Phase 1 to 3 studies; therefore, no dosage adjustment is necessary. See Adverse Reactions.
Pediatric Population: A trial of 288 patients aged 2 to < 17 years of age, of which 276 patients received treatment (153 boys and 123 girls; ASA class 1, 2, and 3; 89.5% were Caucasian; median weight was 25 kg; median age was 7 years) investigated the safety and efficacy of sugammadex versus neostigmine as a reversal agent for neuromuscular blockade induced by rocuronium or vecuronium. Recovery from moderate block to a TOF ratio of ≥ 0.9 was significantly faster in the sugammadex 2 mg/kg group compared with the neostigmine group (geometric mean of 1.6 minutes for sugammadex 2 mg/kg and 7.5 minutes for neostigmine, ratio of geometric means 0.22, 95% CI (0.16, 0.32), (p<0.0001)). Sugammadex 4 mg/kg achieved reversal from deep block with a geometric mean of 2.0 minutes, similar to results observed in adults. These effects were consistent for all age cohorts studied (2 to < 6; 6 to < 12; 12 to < 17 years of age) and for both rocuronium and vecuronium. See Dosage & Administration.
Pharmacokinetics: The sugammadex pharmacokinetic parameters were calculated from the total sum of non-complex-bound and complex-bound concentrations of sugammadex. Pharmacokinetic parameters as clearance and volume of distribution are assumed to be the same for non-complex-bound and complex-bound sugammadex in anesthetized subjects.
Distribution: The observed steady-state volume of distribution of sugammadex is approximately 11 to 14 litres in adult patients with normal renal function (based on conventional, non-compartmental pharmacokinetic analysis). Neither sugammadex nor the complex of sugammadex and rocuronium binds to plasma proteins or erythrocytes, as was shown in vitro using male human plasma and whole blood. Sugammadex exhibits linear kinetics in the dosage range of 1 to 16 mg/kg when administered as an IV bolus dose.
Metabolism: In preclinical and clinical studies no metabolites of sugammadex have been observed and only renal excretion of the unchanged product was observed as the route of elimination.
Elimination: In adult anesthetized patients with normal renal function the elimination half-life (t1/2) of sugammadex is about 2 hours and the estimated plasma clearance is about 88 ml/min. A mass balance study demonstrated that > 90% of the dose was excreted within 24 hours. 96% of the dose was excreted in urine, of which at least 95% could be attributed to unchanged sugammadex. Excretion via feces or expired air was less than 0.02% of the dose. Administration of sugammadex to healthy volunteers resulted in increased renal elimination of rocuronium in complex.
Special populations: Renal impairment and age: In a pharmacokinetic study comparing patients with severe renal impairment to patients with normal renal function, sugammadex levels in plasma were similar during the first hour after dosing and thereafter the levels decreased faster in the control group. Total exposure to sugammadex was prolonged, leading to 17-fold higher exposure in patients with severe renal impairment. Low concentrations of sugammadex are detectable for at least 48 hours post-dose in patients with severe renal insufficiency.
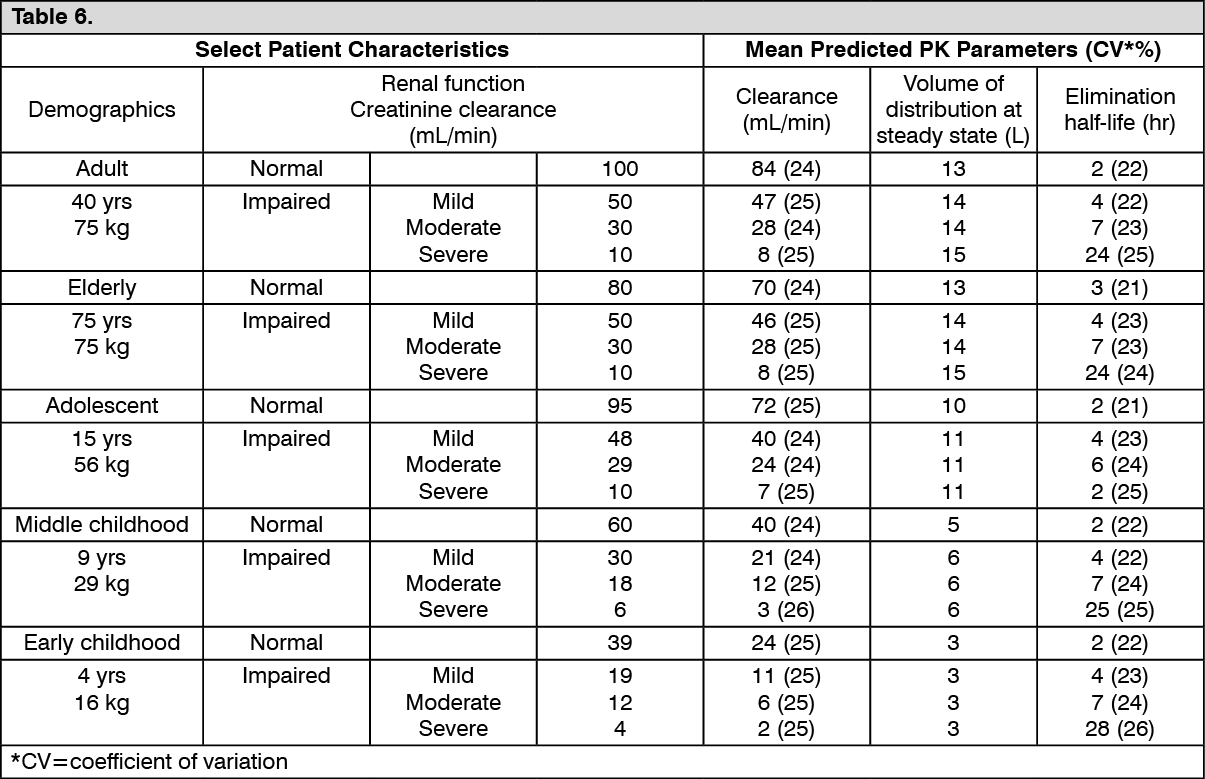
In a second study comparing subjects with moderate or severe renal impairment to subjects with normal renal function, sugammadex clearance progressively decreased and t1/2 was progressively prolonged with declining renal function. Exposure was 2-fold and 5-fold higher in subjects with moderate and severe renal impairment, respectively. Sugammadex concentrations were no longer detectable beyond 7 days post-dose in subjects with severe renal insufficiency.
A summary of sugammadex pharmacokinetic parameters stratified by age and renal function is presented as follows: (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePediatric Patients: Sugammadex pharmacokinetic parameters were estimated in pediatric patients 2 to <17 years of age with patients enrolled into 3 age groups (2 to <6, 6 to <12 and 12 to <17 years of age) and intravenous doses of 2 or 4 mg/kg sugammadex administered for reversal of moderate or deep neuromuscular blockade, respectively. Both clearance and volume of distribution increase with increasing age in pediatric patients.
Sugammadex exposure (AUC0-inf and Cmax) increased in a dose-dependent, linear manner following administration of 2 and 4 mg/kg across patients 2 to <17 years of age. Sugammadex exposure was approximately 40% lower in patients 2 to <6 years of age following administration of 2 or 4 mg/kg sugammadex compared to older pediatric patients (6 to <17 years) and adults; however, this difference was not clinically relevant [see Pharmacodynamics as previously mentioned].
The observed steady-state volume of distribution of sugammadex is approximately 3 to 10 liters and clearance is approximately 38 to 95 mL/min resulting in a half-life of approximately 1-2 hours in pediatric patients 2 to <17 years of age.
Gender: No gender differences were observed.
Race: In a study in healthy Japanese and Caucasian subjects no clinically relevant differences in pharmacokinetic parameters were observed. Limited data do not indicate differences in pharmacokinetic parameters in Black or African Americans.
Body weight: Population pharmacokinetic analysis of adult and elderly patients showed no clinically relevant relationship of clearance and volume of distribution with body weight.
Obesity: In one clinical study in morbidly obese patients, sugammadex 2 mg/kg and 4 mg/kg was dosed according to actual body weight (n=76) or ideal body weight (n=74). Sugammadex exposure increased in a dose-dependent, linear manner following administration according to actual body weight or ideal body weight. No clinically relevant differences in pharmacokinetic parameters were observed between morbidly obese patients and the general population.
Toxicology: Preclinical safety data: Carcinogenicity studies were not done given the intended single-dose use of sugammadex and given the absence of genotoxic potential.
Sugammadex did not impair male or female fertility in rats at 500 mg/kg/day representing approximately 6- to 50-fold greater systemic exposures as compared to human exposures at recommended dose levels. Further, no morphological alterations of male and female reproductive organs were noted in 4-week toxicity studies in rats and dogs. Sugammadex was not teratogenic in rat or rabbit.
Sugammadex is rapidly cleared in preclinical species, although residual sugammadex was observed in bone and teeth of juvenile rats. Preclinical studies in young adult and mature rats demonstrate that sugammadex does not adversely affect tooth color or bone quality, bone structure, or bone metabolism. Sugammadex has no effects on fracture repair and remodeling of bone.