


 Sign Out
Sign Out


Pharmacology: Pharmacodynamics: Mechanism of action: Acalabrutinib is a selective small-molecule inhibitor of Bruton tyrosine kinase (BTK). BTK is a signalling molecule of the B-cell antigen receptor (BCR) and cytokine receptor pathways. In B-cells, BTK signalling results in B-cell survival and proliferation, and is required for cellular adhesion, trafficking, and chemotaxis.
Acalabrutinib and its active metabolite, ACP-5862, form a covalent bond with a cysteine residue in the BTK active site, leading to irreversible inactivation of BTK (IC50 ≤5 nM) with minimal off-target interactions. In a screen of 380 mammalian wild-type kinases, the only additional kinase interactions at clinically relevant concentrations of acalabrutinib and ACP-5862 were with BMX and ERBB4, with 3- to 4-fold less potency than BTK.
In nonclinical studies, acalabrutinib inhibited BTK-mediated activation of downstream signalling proteins CD86 and CD69, inhibited malignant B-cell proliferation and survival, and had minimal activity on other immune cells (T cells and NK cells).
Pharmacodynamic effects: In patients with B-cell malignancies dosed with 100 mg twice daily, median steady state BTK occupancy of ≥95% in peripheral blood was maintained over 12 hours, resulting in inactivation of BTK throughout the recommended dosing interval.
Cardiac Electrophysiology: In a dedicated QT study, at a dose 4 times the maximum recommended dose, CALQUENCE does not prolong the QT/QTc interval to any clinically relevant extent (e.g., not greater than or equal to 10 ms).
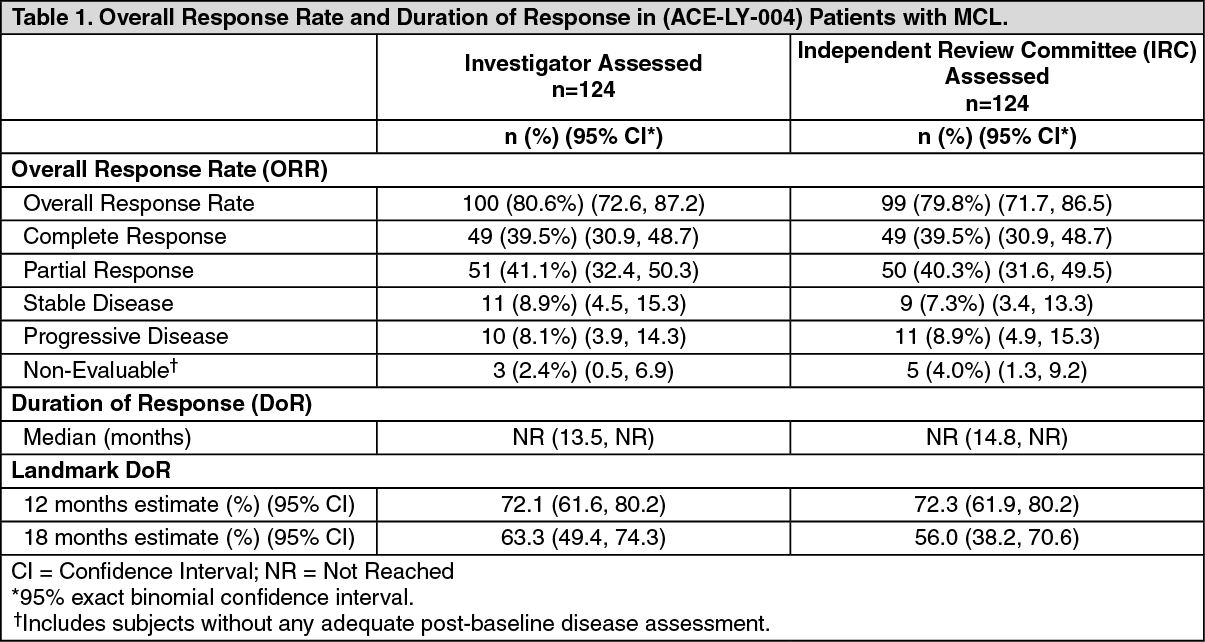
Clinical efficacy and safety in patients: MCL: The safety and efficacy of CALQUENCE in MCL were evaluated in an open-label, multi-centre, single-arm Phase 2 study (ACE-LY-004) of 124 previously treated patients. All patients received CALQUENCE 100 mg orally twice daily until disease progression or unacceptable toxicity. The trial did not include patients who received prior treatment with BTK inhibitors. The primary endpoint was investigator-assessed overall response rate (ORR) per the Lugano classification for non-Hodgkin's lymphoma (NHL). Duration of Response (DoR) was an additional outcome measure. Efficacy results are presented in Table 1.
The median age was 68 (range 42 to 90) years, 79.8% were male and 74.2% were Caucasian. At baseline, 92.8% of patients had an ECOG performance status of 0 or 1. The median time since diagnosis was 46.3 months and the median number of prior treatments was 2 (range 1 to 5), including 17.7% with prior stem cell transplant. The most common prior regimens were CHOP-based (51.6%) and ARA-C (33.9%). At baseline, 37.1% of patients had at least one tumour with a longest diameter ≥5 cm, 72.6% had extra nodal involvement including 50.8% with bone marrow involvement. The simplified MIPI score (which includes age, ECOG score, and baseline lactate dehydrogenase and white cell count) was intermediate in 43.5% and high in 16.9% of patients. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageBased on investigator assessment, 92% of responders achieved a response by cycle 2, with a median time to documented response of 1.9 months. The median DoR had not been reached at 15.2 months median follow-up from treatment initiation. Seventy two percent (72%) of patients had an ongoing response at 12 months per Kaplan-Meier estimate. The ORR was consistent across all pre-specified subgroups including age, performance status, disease stage, and number of prior therapies.
Lymphocytosis: Upon initiation of CALQUENCE, a temporary increase in lymphocyte counts (defined as absolute lymphocyte count increased ≥50% from baseline and a post baseline assessment ≥5 x 109) have been reported in 30.6% of patients in ACE-LY-004. The median time to onset of lymphocytosis was 1.1 weeks and the median duration of lymphocytosis was 5.6 weeks.
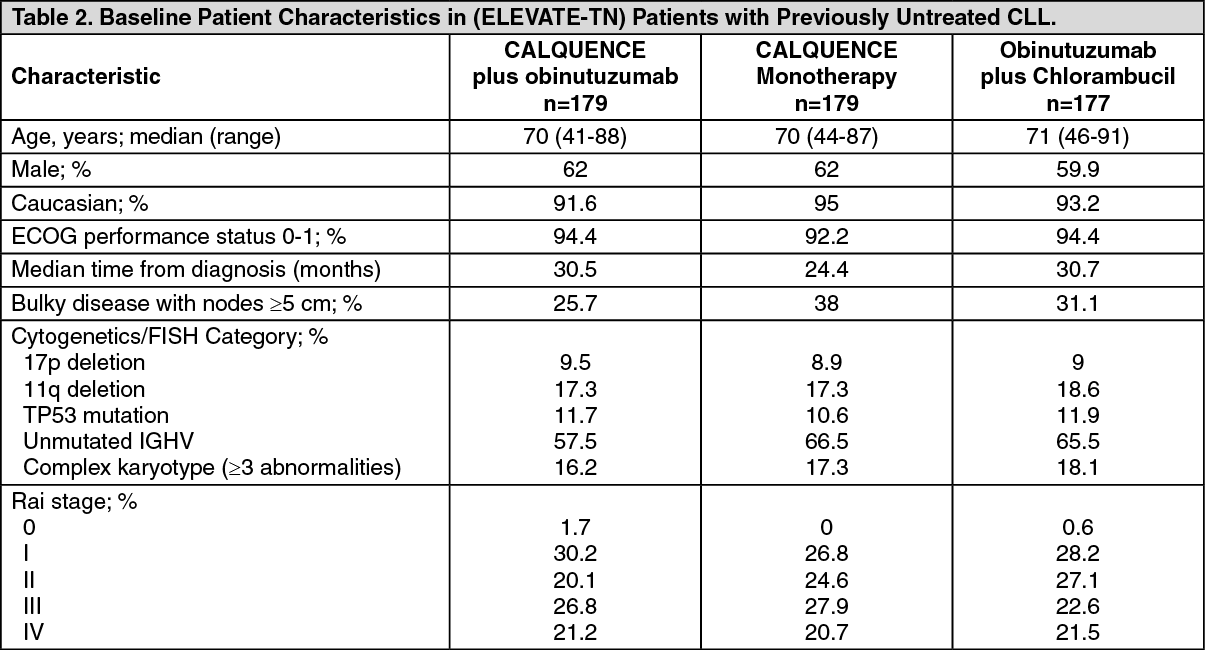
CLL: Patients with Previously Untreated CLL: The safety and efficacy of CALQUENCE in previously untreated CLL were evaluated in a randomised, multi-centre, open-label Phase 3 study (ELEVATE-TN) of 535 patients. Patients received CALQUENCE plus obinutuzumab, CALQUENCE monotherapy, or obinutuzumab plus chlorambucil. Patients 65 years of age or older or between 18 and 65 years of age with coexisting medical conditions were included in ELEVATE-TN. The trial also allowed patients to receive antithrombotic agents other than warfarin or equivalent vitamin K antagonists.
Patients were randomised in a 1:1:1 ratio into 3 arms to receive: CALQUENCE plus obinutuzumab (CALQUENCE+G): CALQUENCE 100 mg was administered twice daily starting on Cycle 1 Day 1 until disease progression or unacceptable toxicity. Obinutuzumab was administered starting on Cycle 2 Day 1 for a maximum of 6 treatment cycles. Obinutuzumab 1000 mg was administered on Days 1 and 2 (100 mg on Day 1 and 900 mg on Day 2), 8 and 15 of Cycle 2 followed by 1000 mg on Day 1 of Cycles 3 up to 7. Each cycle was 28 days.
CALQUENCE monotherapy: CALQUENCE 100 mg was administered twice daily until disease progression or unacceptable toxicity.
Obinutuzumab plus chlorambucil (GClb): Obinutuzumab and chlorambucil were administered for a maximum of 6 treatment cycles. Obinutuzumab 1000 mg was administered on Days 1 and 2 (100 mg on Day 1 and 900 mg on Day 2), 8 and 15 of Cycle 1 followed by 1000 mg on Day 1 of Cycles 2 up to 6. Chlorambucil 0.5 mg/kg was administered on Days 1 and 15 of Cycles 1 up to 6. Each cycle was 28 days.
Patients were stratified by 17p deletion mutation status (presence versus absence), ECOG performance status (0 or 1 versus 2) and geographic region (North America and Western Europe versus Other). After confirmed disease progression, 45 patients randomised on the GClb arm crossed over to CALQUENCE monotherapy. Table 2 summarizes the baseline demographics and disease characteristics of the study population. (See Table 2.)
 Click on icon to see table/diagram/image
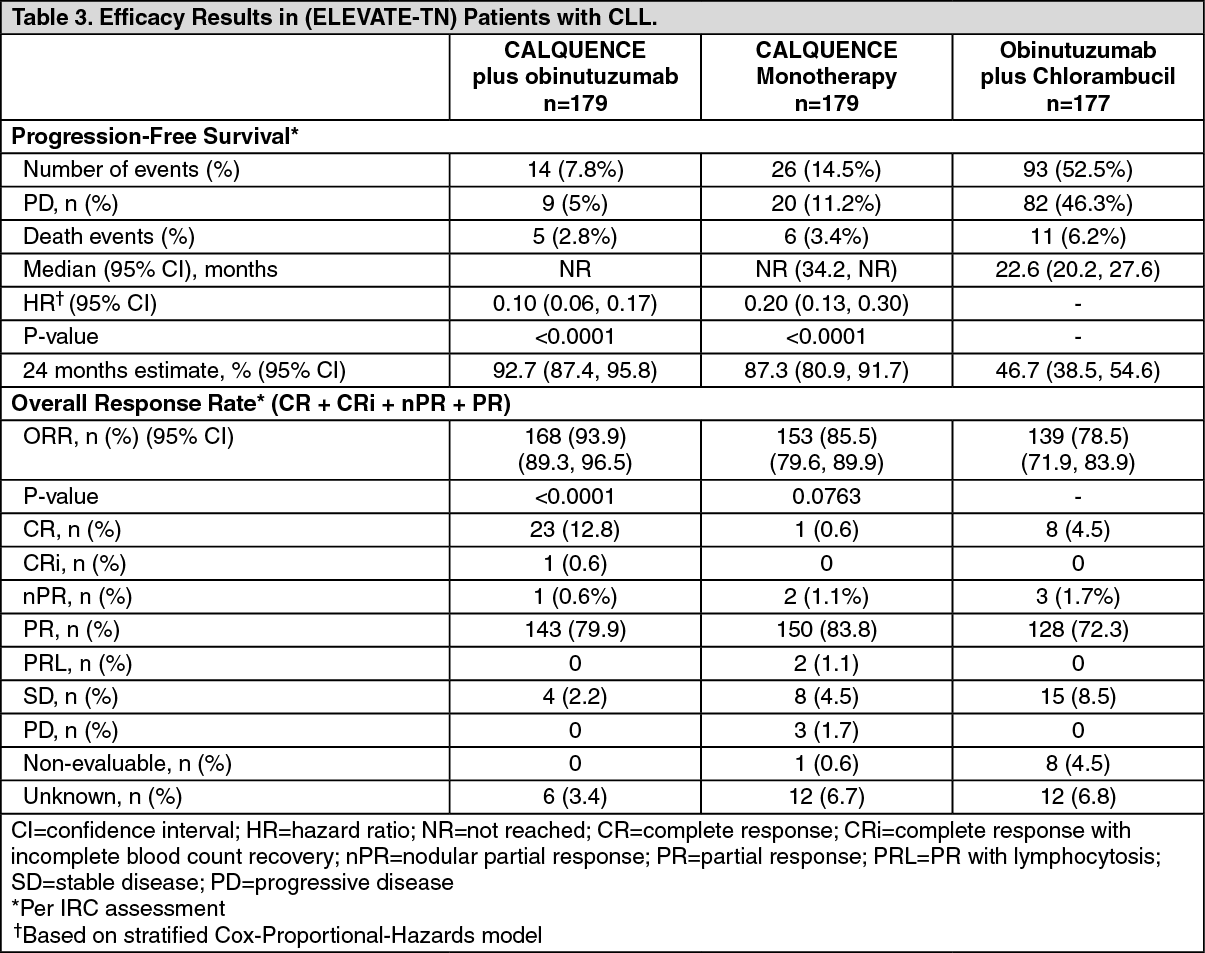
Click on icon to see table/diagram/imageThe primary endpoint was progression-free survival (PFS) as assessed by an Independent Review Committee (IRC) per International Workshop on Chronic Lymphocytic Leukaemia (IWCLL) 2008 criteria with incorporation of the clarification for treatment-related lymphocytosis (Cheson 2012). With a median follow-up of 28.3 months, PFS by IRC indicated a 90% statistically significant reduction in the risk of disease progression or death for previously untreated CLL patients in the CALQUENCE+G arm compared to the GClb arm. At the time of analysis, median overall survival had not been reached in any arm with a total of 37 deaths: 9 (5%) in the CALQUENCE+G arm, 11 (6.1%) in the CALQUENCE monotherapy arm, and 17 (9.6%) in the GClb arm. Efficacy results are presented in Table 3. The Kaplan-Meier curves for PFS are shown in Figure 1. (See Table 3 and Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image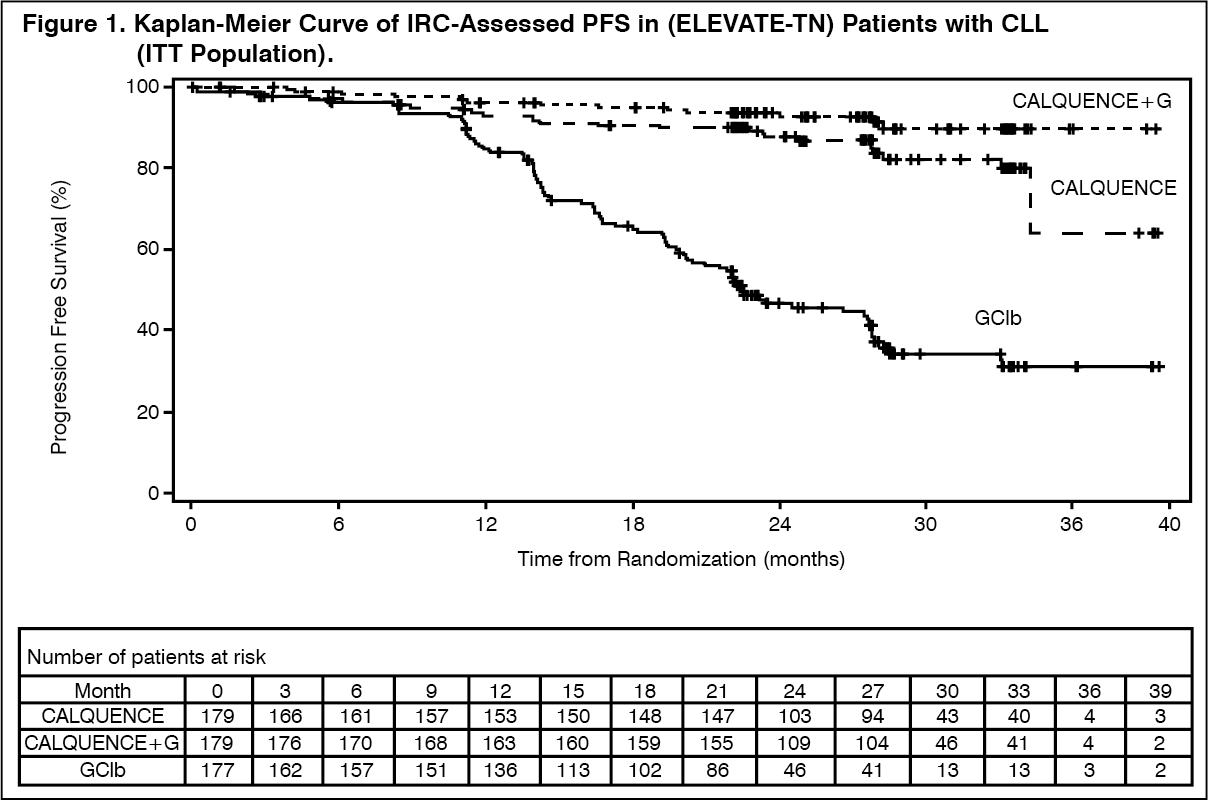 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePFS results for CALQUENCE with or without obinutuzumab were consistent across subgroups, including high risk features. In the high risk CLL population (17p deletion, 11q deletion, TP53 mutation, and unmutated IGHV), the PFS HRs of CALQUENCE with or without obinutuzumab versus obinutuzumab plus chlorambucil was 0.08 [95% CI (0.04, 0.15)] and 0.13 [95% CI (0.08, 0.21)], respectively.
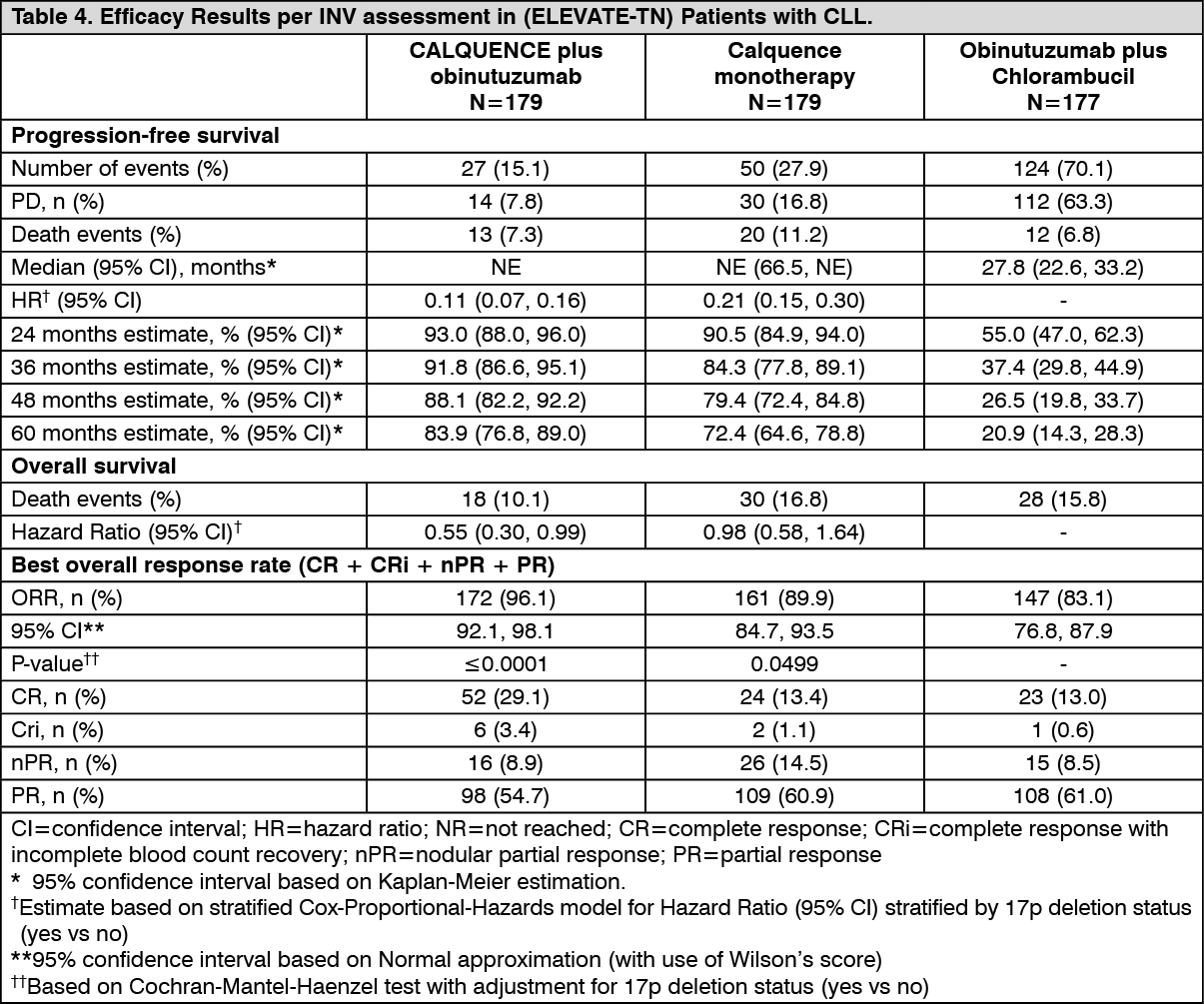
With long term data, the median follow-up was 58.2 months for CALQUENCE+G arm, 58.1 months for Calquence arm and 58.2 months for the GClb arm. The median investigator-assessed PFS for CALQUENCE+G and CALQUENCE monotherapy was not reached; and was 27.8 months in GClb arm. At the time of most recent data cut off, a total of 72 patients (40.7%) originally randomised to the GClb arm crossed over to CALQUENCE monotherapy. The median overall survival had not been reached in any arm with a total of 76 deaths: 18 (10.1%) in the CALQUENCE+G arm, 30 (16.8%) in the CALQUENCE monotherapy arm, and 28 (15.8%) in the GClb arm. The time to next treatment was prolonged for CALQUENCE+G arm (HR=0.14 [95% CI: 0.09, 0.21]; 0<0.0001) and Calquence only arm (HR=0.27 [95% CI: 0.19, 0.38]; 0<0.0001) compared to GClb arm. (See Table 4 and Figure 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image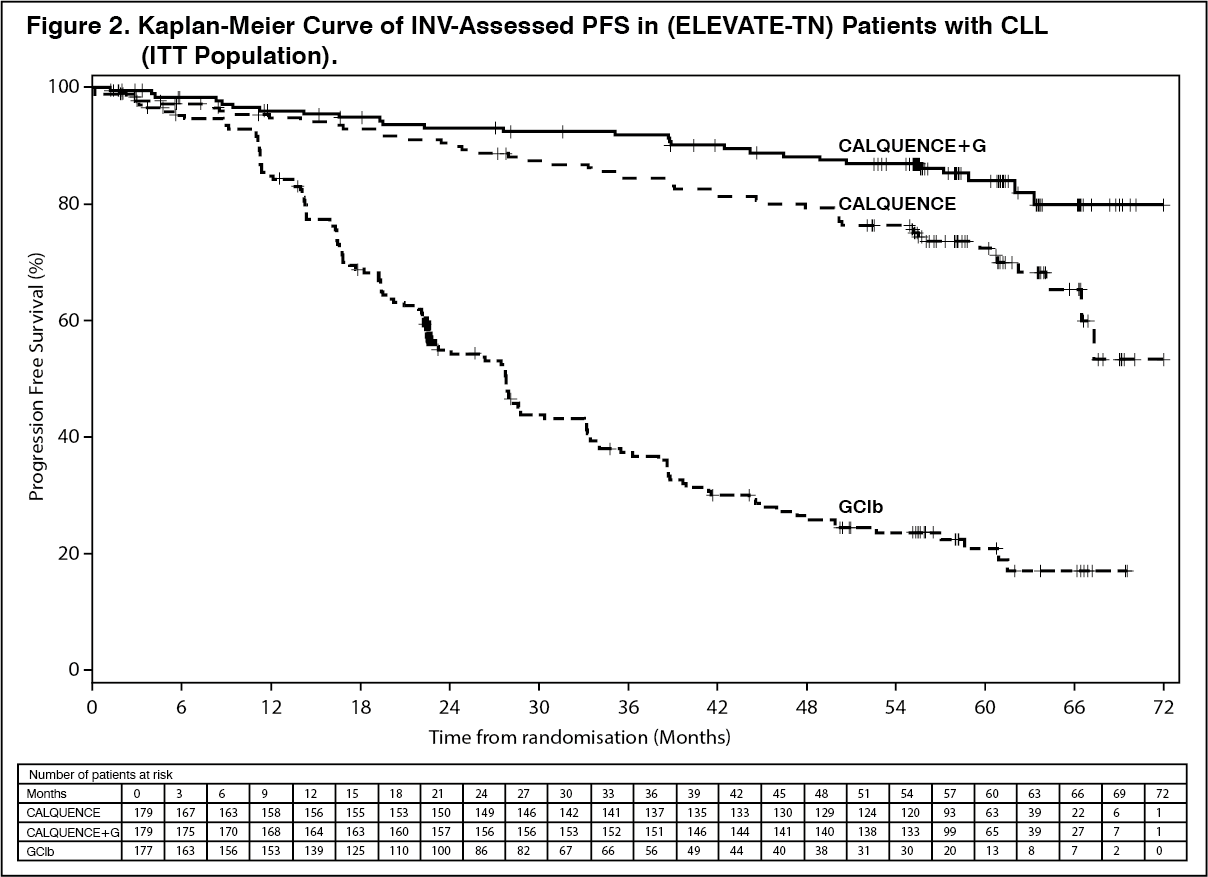 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePatients with CLL who received at least one prior therapy: The safety and efficacy of CALQUENCE in relapsed or refractory CLL were evaluated in a randomised, multi-centre, open-label phase 3 study (ASCEND) of 310 patients who received at least one prior therapy. Patients received CALQUENCE monotherapy or investigator's choice of either idelalisib plus rituximab or bendamustine plus rituximab. The trial allowed patients to receive antithrombotic agents other than warfarin or equivalent vitamin K antagonists.
Patients were randomised 1:1 to receive either: CALQUENCE 100 mg twice daily until disease progression or unacceptable toxicity, or; Investigator's choice: Idelalisib 150 mg twice daily until disease progression or unacceptable toxicity in combination with ≤8 infusions of rituximab (375 mg/m2/500 mg/m2) on Day 1 of each 28-day cycle for up to 6 cycles.
Bendamustine 70 mg/m2 (Day 1 and 2 of each 28-day cycle) in combination with rituximab (375 mg/m2/500 mg/m2) on Day 1 of each 28-day cycle for up to 6 cycles.
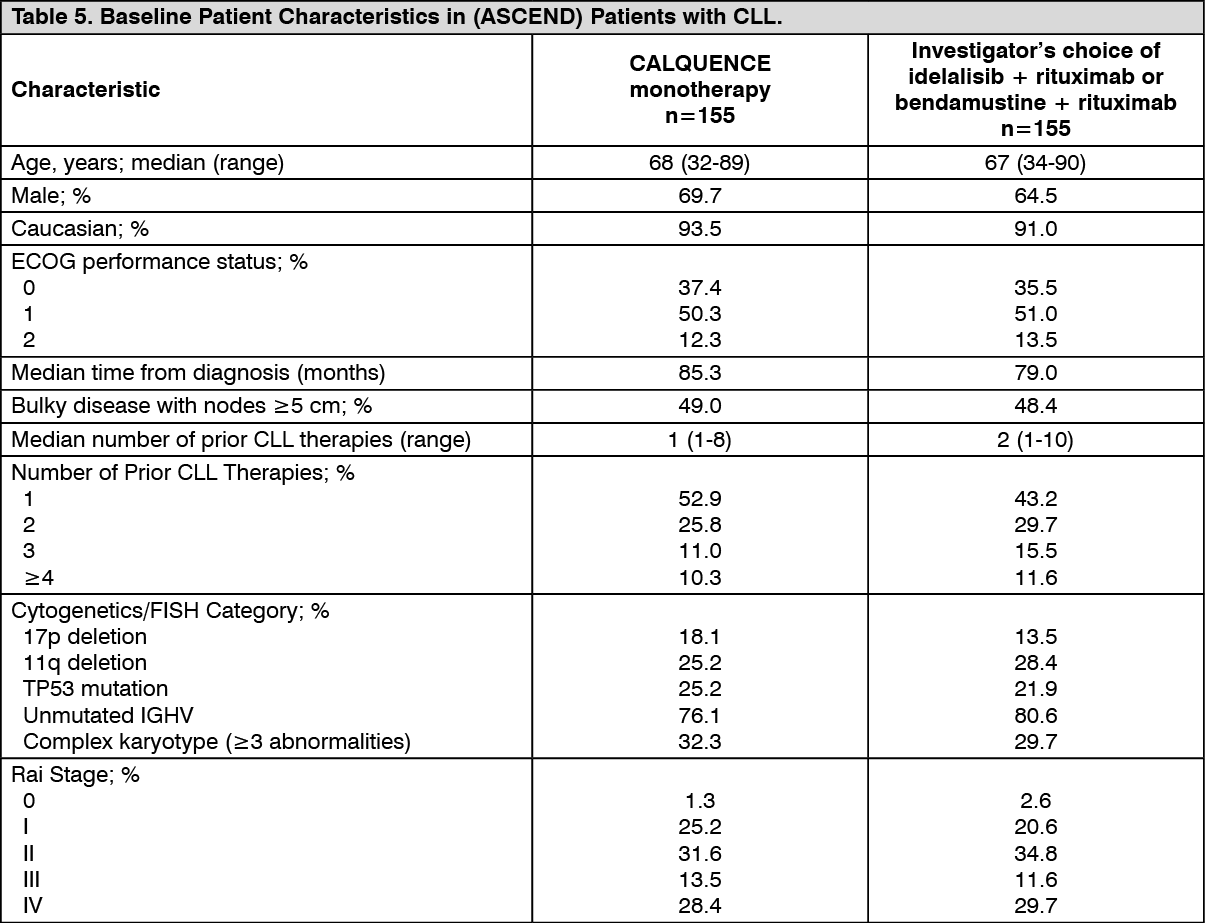
Patients were stratified by 17p deletion mutation status (presence versus absence), ECOG performance status (0 or 1 versus 2) and number of prior therapies (1 to 3 versus ≥4). After confirmed disease progression, 35 patients randomised on investigator's choice of either idelalisib plus rituximab or bendamustine plus rituximab crossed over to CALQUENCE. Table 5 summarizes the baseline demographics and disease characteristics of the study population. (See Table 5.)
 Click on icon to see table/diagram/image
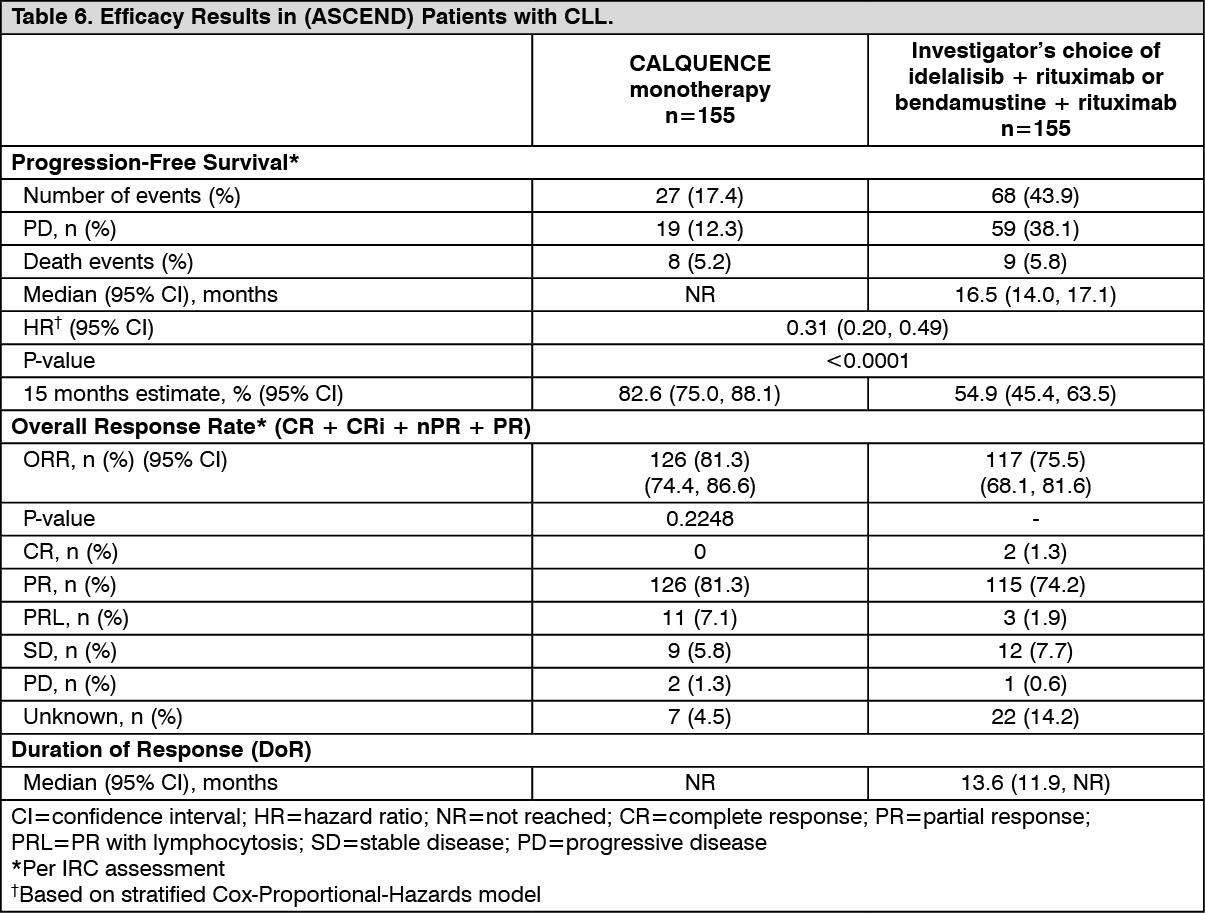
Click on icon to see table/diagram/imageThe primary endpoint was PFS as assessed by IRC IWCLL 2008 criteria with incorporation of the clarification for treatment-related lymphocytosis (Cheson 2012). With a median follow-up of 16.1 months, PFS indicated a 69% statistically significant reduction in the risk of death or progression for patients in the CALQUENCE Arm. At the time of analysis, median overall survival had not been reached in any arm with a total of 33 deaths: 15 (9.7%) in the CALQUENCE monotherapy arm and 18 (11.6%) in the investigator's choice of either idelalisib plus rituximab or bendamustine plus rituximab arm. Efficacy results are presented in Table 6. The Kaplan-Meier curve for PFS is shown in Figure 3. (See Table 6 and Figure 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image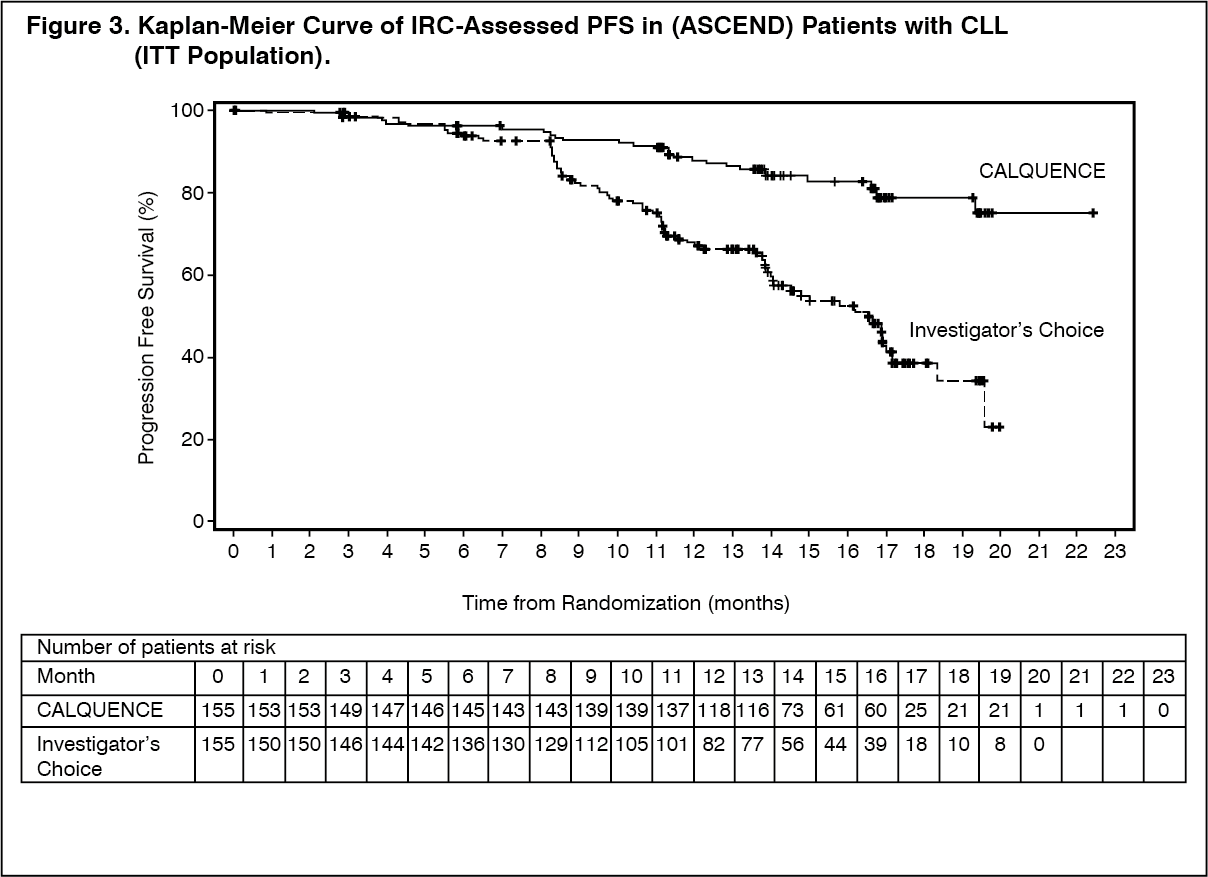 Click on icon to see table/diagram/image
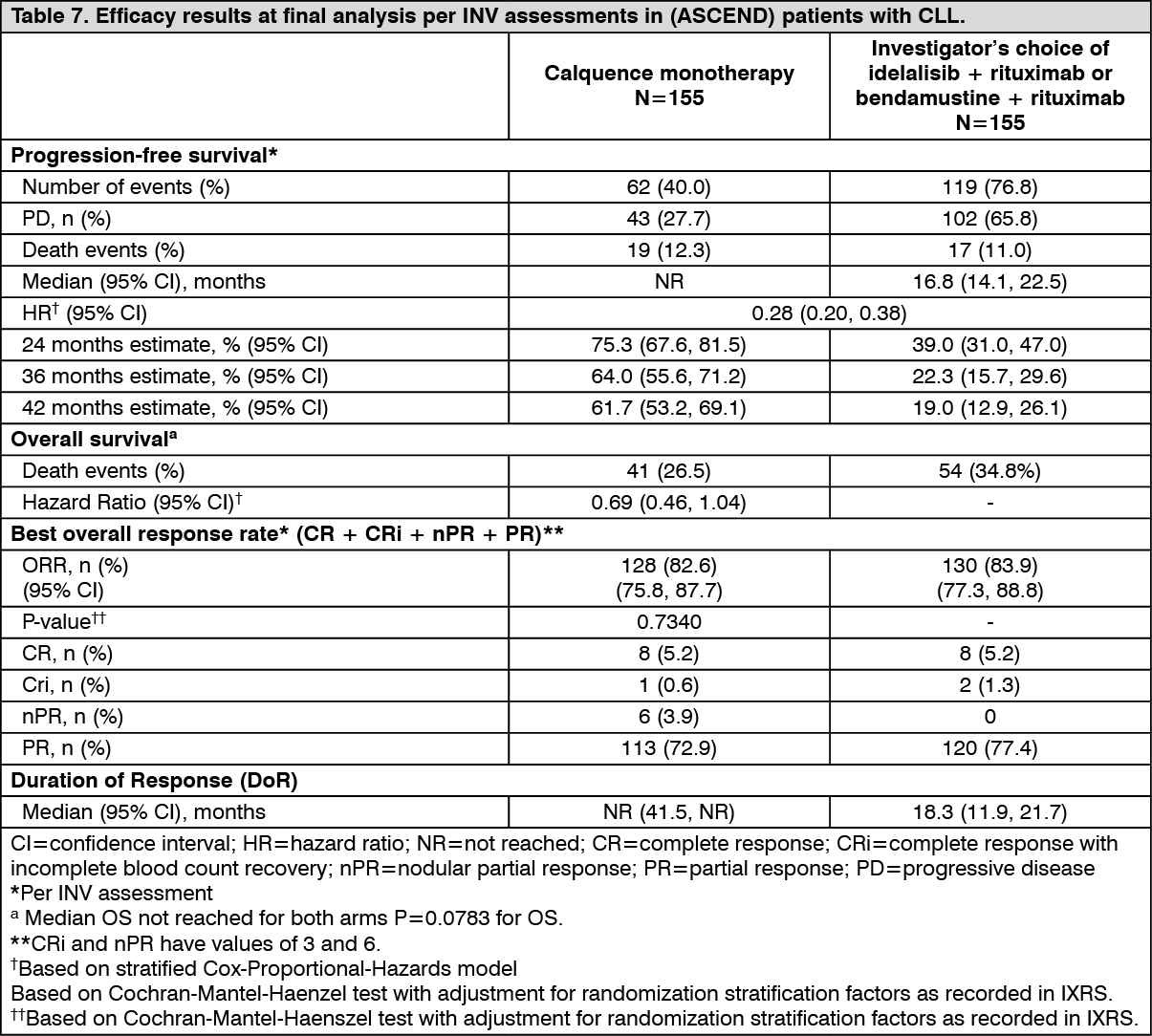
Click on icon to see table/diagram/imageAt the final analysis, with a median follow-up of 46.5 months for CALQUENCE and 45.3 months for the IR/BR, 72% reduction in risk of investigator-assessed disease progression or death was observed for patients in the CALQUENCE arm. The median investigator-assessed PFS was not reached in CALQUENCE and was 16.8 months in IR/BR. The median investigator-assessed PFS in patients with 17p deletion per IWCLL criteria was not reached in CALQUENCE arm and was 13.8 months in IR/BR arm.
At the time of final analysis, median overall survival had not been reached in any arm with a total of 95 deaths: 41 (26.5%) in the CALQUENCE monotherapy arm and 54 (34.8%) in the IR/BR arm. (See Table 7 and Figure 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image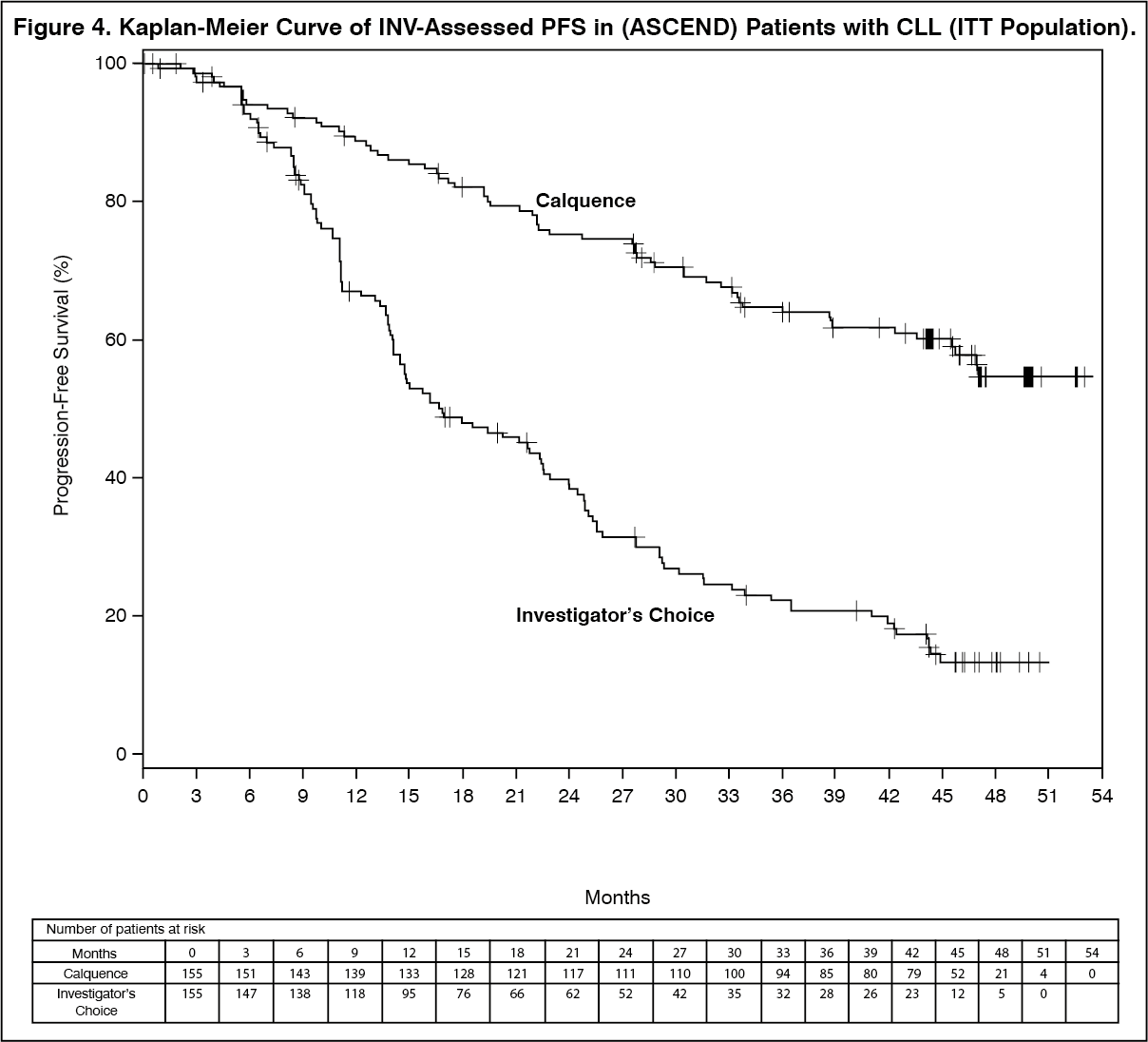 Click on icon to see table/diagram/image
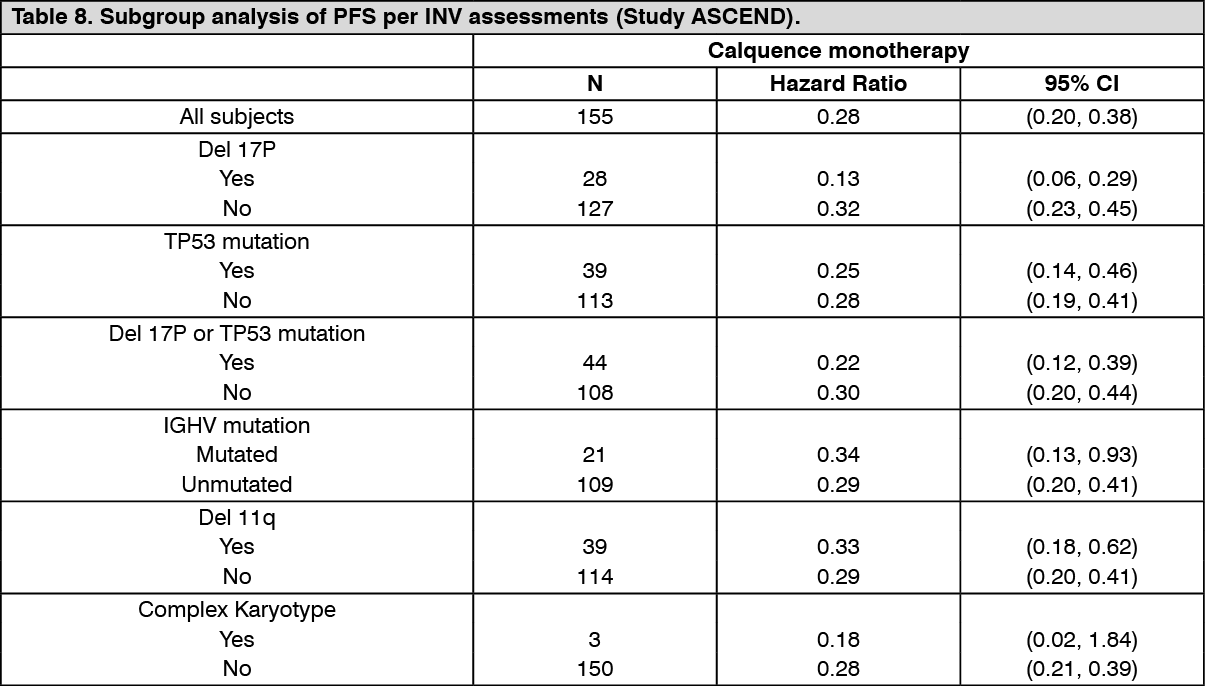
Click on icon to see table/diagram/imageInvestigator assessed PFS results for CALQUENCE at final analysis were consistent across subgroups, including high risk features and were consistent with the primary analysis. In the high risk CLL population (17p deletion, 11q deletion, TP53 mutation, and unmutated IGHV), the investigator assessed PFS HR was 0.26 [95% CI (0.19, 0.37)]. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: The pharmacokinetics (PK) of acalabrutinib and its active metabolite, ACP-5862, were studied in healthy subjects and patients with B-cell malignancies. Acalabrutinib exhibits dose-proportionality, and both acalabrutinib and ACP-5862 exhibit almost linear PK across a dose range of 75 to 250 mg. Population PK modelling suggests that the PK of acalabrutinib and ACP-5862 does not differ significantly in patients with different B-cell malignancies. At the recommended dose of 100 mg twice daily in patients with B-cell malignancies (including MCL and CLL), the geometric mean steady state, daily area under the plasma drug concentration over time curve (AUC24h) and maximum plasma concentration (Cmax) of acalabrutinib were 1893 ng·h/mL and 466 ng/mL, respectively, and for ACP-5862 were 4091 ng·h/mL and 420 ng/mL, respectively.
Absorption: The median time to peak plasma concentrations (Tmax) was 0.75 hours, and 1.0 hour for ACP-5862. The absolute bioavailability of CALQUENCE was 25%.
Distribution: Reversible binding to human plasma protein was 97.5% for acalabrutinib and 98.6% for ACP-5862. The in vitro mean blood-to-plasma ratio was 0.8 for acalabrutinib and 0.7 for ACP-5862. The mean steady state volume of distribution (Vss) was approximately 34 L for acalabrutinib.
Biotransformation/Metabolism: In vitro, acalabrutinib is predominantly metabolized by CYP3A enzymes, and to a minor extent by glutathione conjugation and amide hydrolysis. ACP-5862 was identified as the major metabolite in plasma with a geometric mean exposure (AUC) that was approximately 2- to 3-fold higher than the exposure of acalabrutinib. ACP-5862 is approximately 50% less potent than acalabrutinib with regard to BTK inhibition.
In vitro, acalabrutinib is a weak inhibitor of CYP3A4/5, CYP2C8 and CYP2C9, but does not inhibit CYP1A2, CYP2B6, CYP2C19, CYP2D6, UGT1A1, and UGT2B7. ACP-5862 is a weak inhibitor of CYP2C8, CYP2C9 and CYP2C19, but does not inhibit CYP1A2, CYP2B6, CYP2D6, CYP3A4/5, UGT1A1, and UGT2B7 in vitro. Acalabrutinib is a weak inducer of CYP1A2, CYP2B6 and CYP3A4 mRNA; ACP-5862 weakly induces CYP3A4.
Interactions with transport proteins: In vitro, acalabrutinib and its active metabolite, ACP-5862, are substrates of P-glycoprotein (P-gp) and breast cancer resistance protein (BCRP). Acalabrutinib is not a substrate of renal uptake transporters OAT1, OAT3, and OCT2, or hepatic transporters OATP1B1 and OATP1B3, in vitro. ACP-5862 is not a substrate of OATP1B1 or OATP1B3.
Acalabrutinib and ACP-5862 do not inhibit P-gp, OAT1, OAT3, OCT2, OATP1B1, OATP1B3, and MATE2-K at clinically relevant concentrations.
Acalabrutinib may inhibit intestinal BCRP substrates (see Interactions), while ACP-5862 may inhibit MATE1 (see Interactions) at clinically relevant concentrations. Acalabrutinib does not inhibit MATE1, while ACP-5862 does not inhibit BCRP at clinically relevant concentrations.
Elimination: Following a single oral dose of 100 mg acalabrutinib, the median terminal elimination half-life (t½) of acalabrutinib was 0.9 (range: 0.6 to 2.8) hours. The median t½ of the active metabolite, ACP-5862, was 6.9 (range 2.7 to 9.1) hours.
The mean apparent oral clearance (CL/F) was 70 L/hr for acalabrutinib and 13 L/hr for ACP-5862, with similar PK between patients and healthy subjects based on population PK analysis.
Following administration of a single 100 mg radiolabelled [14C]-acalabrutinib dose in healthy subjects, 84% of the dose was recovered in the faeces and 12% of the dose was recovered in the urine, with less than 2% of the dose excreted as unchanged acalabrutinib in urine and faeces.
Pharmacokinetics in Special Populations: Based on population PK analysis, age, sex, race (Caucasian, African American), and body weight did not have clinically meaningful effects on the PK of acalabrutinib and its active metabolite, ACP-5862.
Renal Impairment: Acalabrutinib undergoes minimal renal elimination. A pharmacokinetic study in patients with renal impairment has not been conducted.
Based on population PK analysis, no clinically relevant PK difference was observed in 433 patients with mild renal impairment (eGFR between 60 and 89 mL/min/1.73m2 as estimated by MDRD), 110 patients with moderate renal impairment (eGFR between 30 and 59 mL/min/1.73m2) relative to 204 patients with normal renal function (eGFR greater than or equal to 90 mL/min/1.73m2). The pharmacokinetics of acalabrutinib has not been characterised in patients with severe renal impairment (eGFR less than 29 mL/min/1.73m2) or renal impairment requiring dialysis. Patients with creatinine levels greater than 2.5 times the institutional ULN were not included in the clinical trials (see Dosage & Administration).
Hepatic Impairment: Acalabrutinib is metabolized in the liver. In dedicated hepatic impairment studies, compared to subjects with normal liver function (n=6), acalabrutinib exposure (AUC) was increased by 1.9-fold, 1.5-fold, and 5.3-fold in subjects with mild (n=6) (Child-Pugh A), moderate (n=6) (Child-Pugh B), and severe (n=8) (Child-Pugh C) hepatic impairment, respectively. Based on a population PK analysis, no clinically relevant difference was observed between subjects with mild (n=79) or moderate (n=6) hepatic impairment (total bilirubin between 1.5 to 3 times ULN and any AST) relative to subjects with normal (n=651) hepatic function (total bilirubin and AST within ULN).
Toxicology: Preclinical safety data: Carcinogenicity: Carcinogenicity studies have not been conducted with acalabrutinib.
Genotoxicity/Mutagenicity: Acalabrutinib was not mutagenic in a bacterial reverse mutation assay, in an in vitro chromosome aberration assay, or in an in vivo mouse bone marrow micronucleus assay.
Repeat-dose toxicity: Daily oral administration of acalabrutinib for up to 6 months duration in rats and 9 months in dogs was tolerated at exposure levels that exceed human therapeutic exposures at the recommended dose (2.5-fold in rats, 8.2-fold in dogs, based on AUC).
In rats, renal effects including tubular degeneration were observed at exposures 4.2 times or greater than that of the recommended human dose. Renal effects were reversible with complete recovery in rats exposed at levels 4.2 times the recommended human dose and partial recovery in rats at the higher exposures (6.8-fold or greater).
In rats, dose-responsive reversible liver findings including individual hepatocyte necrosis were observed after exposures 4.2 times or greater than that of the recommended human dose.
Cardiac toxicities (myocardial haemorrhage, inflammation, necrosis) were observed in rats that died during the study and at exposures equivalent to 6.8 times or greater than that of the human recommended dose. Reversibility for the heart findings could not be assessed as these findings were only observed at doses above the maximum tolerated dose (MTD). At exposures representing 4.2 times the human recommended dose, no cardiac toxicities were observed.
Reproductive toxicology: No effects on fertility were observed in male or female rats at exposures 10 or 9 times the human AUC exposure at the recommended dose, respectively.
In a combined fertility and embryofoetal development study in female rats, acalabrutinib was administered orally at doses up to 200 mg/kg/day starting 14 days prior to mating through gestational day [GD] 17. No effects on embryofoetal development and survival were observed. The AUC at 200 mg/kg/day in pregnant rats was approximately 9-times the AUC in patients at the recommended dose of 100 mg twice daily. The presence of acalabrutinib and its active metabolite were confirmed in foetal rat plasma.
In an embryofoetal study in pregnant rabbits, acalabrutinib was administered orally at doses up to 200 mg/kg/day during the period of organogenesis (from GD 6-18). Acalabrutinib produced no maternal toxicity and no evidence of teratogenicity or foetal development, growth, or survival at doses of 50 mg/kg/day (approximately equivalent to the human AUC exposure at the recommended dose). Decreased foetal body weight and delayed ossification were observed at exposure levels that produced maternal toxicity (doses ≥100 mg/kg/day), which were 2.4-times greater than the human exposure levels at the recommended dose.
In a rat reproductive study, dystocia (prolonged /difficult labour) was observed at exposures >2.3-times the clinical exposure at 100 mg twice daily.