Oral Mild dementia in Alzheimer's disease, Moderate dementia in Alzheimer's disease, Severe dementia in Alzheimer's disease
Adult: As oral solution and 5 mg or 10 mg conventional/orodispersible tab: Initially, 5 mg once daily, may increase dose to 10 mg once daily after 4-6 weeks. Max: 10 mg daily. Alternative dosing in severe cases: Initially, 5 mg once daily, may increase dose to 10 mg once daily after 4-6 weeks (using 5 mg or 10 mg conventional or orodispersible tab). If well tolerated and stabilised on a 10 mg daily dose for at least 3 months, the dose may be further increased to 23 mg once daily (using 23 mg conventional tab). All doses are taken preferably in the evening, just before bedtime. Clinical benefit must be re-assessed regularly. Dosing and treatment recommendations may vary among individual products and between countries (refer to detailed product guidelines).
Hepatic Impairment
Mild to moderate: Dose escalation must be done according to individual tolerability.
Administration
May be taken with or without food. Take in the evening just prior to retiring. 23-mg tab: Swallow whole, do not split/crush/chew. ODT: Allow to dissolve on the tongue & follow w/ water.
Special Precautions
Patient with history of cardiac disease (e.g. uncompensated heart failure, recent MI, bradyarrhythmias), pre-existing or family history of QTc prolongation, sick sinus syndrome, cardiac conduction abnormalities (e.g. sinoatrial or AV block), electrolyte disturbances (e.g. hypokalaemia, hypomagnesaemia); history of asthma or COPD; history of seizure disorders; bladder outlet obstruction, risk factors for peptic ulcer disease (e.g. history of ulcer disease, concurrent NSAID use); risk factors for rhabdomyolysis (e.g. history of muscular disorders, uncontrolled hypothyroidism, receiving agents that may cause rhabdomyolysis). Renal and hepatic impairment. Pregnancy and lactation.
Adverse Reactions
Significant: Cardiac effects (e.g. hypertension, syncope, bradycardia, sinoatrial or AV block, QTc interval prolongation, torsades de pointes); gastrointestinal effects (e.g. nausea, vomiting, diarrhoea), may increase gastric acid secretion; weight loss and/or anorexia, bladder outflow obstruction; generalised seizures, may exacerbate or induce extrapyramidal symptoms. Rarely, rhabdomyolysis (including acute renal failure). Gastrointestinal disorders: Abdominal pain or disturbance. General disorders and administration site conditions: Fatigue, pain, asthenia. Infections and infestations: Common cold. Injury, poisoning and procedural complications: Accidental injury, including falls. Investigations: Increased creatine phosphokinase. Musculoskeletal and connective tissue disorders: Muscle cramps. Nervous system disorders: Headache, dizziness, somnolence. Psychiatric disorders: Insomnia, agitation, abnormal dreams, nightmares, hallucination, aggressive behaviour. Renal and urinary disorders: Urinary incontinence, frequent urination. Skin and subcutaneous tissue disorders: Rash, pruritus, ecchymosis. Potentially Fatal: Rarely, neuroleptic malignant syndrome (NMS).
This drug may cause dizziness, somnolence, muscle cramps, and fatigue, if affected, do not drive or operate machinery.
Monitoring Parameters
Evaluate bladder adequacy before treatment initiation. Monitor mental status, weight, and pulse. Close monitor for signs and symptoms of rhabdomyolysis, active or occult gastrointestinal bleeding, and gastrointestinal intolerance (e.g. nausea, vomiting).
Overdosage
Symptoms: Cholinergic crisis characterised by severe nausea, vomiting, salivation, sweating, hypotension, bradycardia, convulsion, respiratory depression, collapse, and increasing muscle weakness. Management: Supportive treatment. May administer 1-2 mg IV atropine initial dose, then subsequent doses are titrated according to the effect and clinical response.
Drug Interactions
May increase the risk of QTc prolongation and torsades de pointes with other agents known to prolong the QTc interval, such as class IA antiarrhythmics (e.g. quinidine), class III antiarrhythmics (e.g. sotalol, amiodarone), certain antidepressants (e.g. escitalopram, amitriptyline), some antipsychotics (e.g. pimozide, sertindole, phenothiazine derivatives), and certain antibiotics (e.g. clarithromycin, levofloxacin). May exaggerate the effects certain muscle relaxants (e.g. suxamethonium chloride) during anaesthesia. May result in a synergistic effect with suxamethonium chloride, similar neuromuscular blockers, and cholinergic agonists (e.g. bethanechol). Plasma concentrations may be increased with CYP3A4 inhibitors (e.g. ketoconazole, itraconazole, erythromycin) and CYP2D6 inhibitors (e.g. fluoxetine, quinidine). Plasma levels may be decreased with enzyme inducers (e.g. rifampicin, phenytoin, carbamazepine). Potentially Fatal: Increased risk of NMS with antipsychotics.
Action
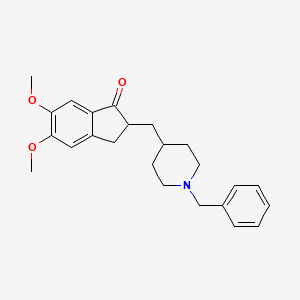
Description: Mechanism of Action: Donepezil, a piperidine derivative, is a reversible and selective acetylcholinesterase inhibitor. It reversibly and non-competitively blocks the centrally active anticholinesterase (an enzyme responsible for acetylcholine hydrolysis). This action increases acetylcholine concentrations available for synaptic transmission in the central nervous system (CNS). Pharmacokinetics: Absorption: Well absorbed from the gastrointestinal tract. Time to peak plasma concentration: 3-4 hours (5-10 mg conventional or orodispersible tab); approx 8 hours (23 mg conventional tab). Distribution: Protein binding: Approx 96%, mainly to albumin (75%) and α1-acid glycoprotein (21%). Metabolism: Extensively metabolised in the liver mainly by CYP3A4 isoenzyme and to a lesser extent by CYP2D6 to form 4 major metabolites (2 are active metabolites). Excretion: Via urine (57%; 17% as unchanged drug); faeces (15%). Elimination half-life: Approx 70 hours.
Chemical Structure
Source: National Center for Biotechnology Information. PubChem Compound Summary for CID 3152, Donepezil. https://pubchem.ncbi.nlm.nih.gov/compound/Donepezil. Accessed May 30, 2024.



 Sign Out
Sign Out