


 Sign Out
Sign Out

Pharmacokinetics: Absorption and Distribution: The pharmacokinetics of gemcitabine were examined in 353 patients, with various solid tumors. Pharmacokinetic parameters were derived using data from patients treated for varying durations of therapy given weekly with periodic rest weeks and using both short infusions (<70 minutes) and long infusions (70 to 285 minutes). The total gemcitabine for injection dose varied from 500 to 3600 mg/m2.
The volume of distribution was increased with infusion length. Volume of distribution of gemcitabine was 50 L/m2 following infusions lasting <70 minutes. For long infusions, the volume of distribution rose to 370 L/m2. Gemcitabine pharmacokinetics are linear and are described by a 2-compartment model. Population pharmacokinetic analyses of combined single and multiple dose studies showed that the volume of distribution of gemcitabine was significantly influenced by duration of infusion and gender. Gemcitabine plasma protein binding is negligible.
Metabolism: Gemcitabine disposition was studied in 5 patients who received a single 1000 mg/m2/30 minute infusion of radiolabeled drug. Within one (1) week, 92% to 98% of the dose was recovered, almost entirely in the urine. Gemcitabine (<10%) and the inactive uracil metabolite, 2'-deoxy-2',2'-difluorouridine (dFdU), accounted for 99% of the excreted dose. The metabolite dFdU is also found in plasma.
The active metabolite, gemcitabine triphosphate, can be extracted from peripheral blood mononuclear cells. The half-life of the terminal phase for gemcitabine triphosphate from mononuclear cells ranges from 1.7 to 19.4 hours.
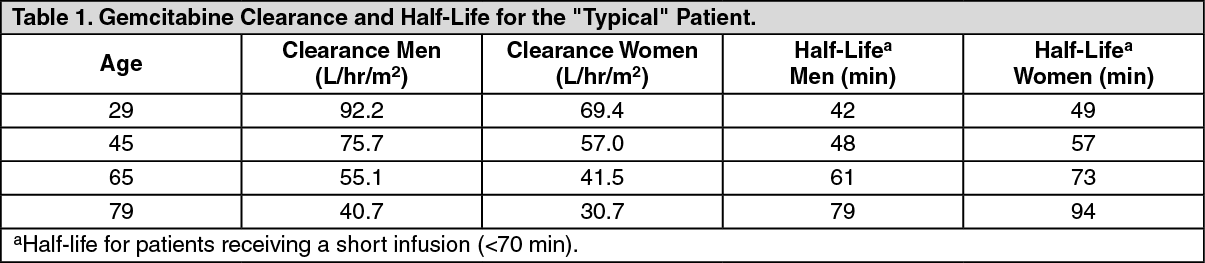
Excretion: Clearance of gemcitabine was affected by age and gender. The lower clearance in women and the elderly results in higher concentrations of gemcitabine for any given dose. Differences in either clearance or volume of distribution based on patient characteristics or the duration of infusion result in changes in half-life and plasma concentrations. Table 1 shows plasma clearance and half-life of gemcitabine following short infusions for typical patients by age and gender. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageGemcitabine half-life for short infusions ranged from 42 to 94 minutes, and the value for long infusions varied from 245 to 638 minutes, depending on age and gender, reflecting a greatly increased volume of distribution with longer infusions.
Drug Interactions: When gemcitabine for injection (1250 mg/m2 on Days 1 and 8) and cisplatin (75 mg/m2 on Day 1) were administered in NSCLC patients, the clearance of gemcitabine on Day 1 was 128 L/hr/m2 and on Day 8 was 107 L/hr/m2. The clearance of cisplatin in the same study was reported to be 3.94 mL/min/m2 with a corresponding half-life of 134 hours [see Interactions]. Analysis of data from metastatic breast cancer patients shows that, on average, gemcitabine for injection has little or no effect on the pharmacokinetics (clearance and half-life) of paclitaxel and paclitaxel has little or no effect on the pharmacokinetics of gemcitabine for injection. Data from NSCLC patients demonstrate that gemcitabine for injection and carboplatin given in combination does not alter the pharmacokinetics of gemcitabine for injection or carboplatin compared to administration of either single-agent. However, due to wide confidence intervals and small sample size, interpatient variability may be observed.