Adult: For cases characterised by sleep onset and/or sleep maintenance difficulties: 5 mg once daily taken immediately before bedtime, with at least 7 hours remaining prior to the planned time of awakening. May increase dose according to clinical response and tolerability. Max: 10 mg once daily. Use the lowest effective dose for the shortest duration.
Special Patient Group
Patients taking concomitant weak CYP3A inhibitors: Max: 5 mg once daily at night.
Hepatic Impairment
Moderate: Max: 5 mg once daily at night. Severe: Not recommended.
Administration
film-coated tab: Should be taken on an empty stomach. Take immediately before going to bed. Time to sleep onset may be delayed if taken w/ or soon after a meal.
Contraindications
Narcolepsy. Concomitant use with moderate or strong CYP3A inducers and inhibitors, and alcohol.
Special Precautions
Patient with depression, history of drug dependence or abuse; respiratory compromise, including COPD or moderate to severe obstructive sleep apnoea. Patients taking concomitant weak CYP3A inhibitors. Hepatic and severe renal impairment. Elderly (particularly with high doses). Lactation.
Adverse Reactions
Significant: CNS depression and daytime wakefulness impairment, worsening of depression, sleep paralysis, hypnagogic or hypnopompic hallucinations (including vivid and disturbing perceptions), mild cataplexy-like symptoms (e.g. transient leg weakness); complex sleep behaviours including sleep-walking, sleep-driving, and performing other activities while not fully awake (e.g. making phone calls, preparing and eating foods). Cardiac disorders: Palpitation. General disorders and administration site conditions: Fatigue. Nervous system disorders: Headache, somnolence. Psychiatric disorders: Abnormal dreams, nightmares. Potentially Fatal: Suicide, suicidal ideation and behaviour.
Patient Counseling Information
This drug may cause CNS depression (e.g. drowsiness, impaired daytime wakefulness), if affected, do not drive or operate machinery.
Monitoring Parameters
Carefully evaluate the potential causes of sleep disturbance before starting therapy; failure of insomnia resolution after 7-10 days of treatment may indicate psychiatric and/or medical illness. Monitor hepatic and renal function at baseline and as clinically indicated. Observe for worsening depression or suicidality, mental alertness.
Overdosage
Symptom: Increased frequency of somnolence (dose-dependent). Management: Supportive treatment with close monitoring and medical supervision.
Drug Interactions
May increase the risk of side effects with weak CYP3A inhibitors (e.g. ranitidine, chlorzoxazone). Increased risk of CNS depression with other CNS depressants (e.g. TCA, opioids, benzodiazepines). May reduce the efficacy of CYP2B6 substrates (e.g. bupropion, methadone). Potentially Fatal: Increased risk of adverse effects with moderate or strong CYP3A inhibitors (e.g. fluconazole, verapamil, itraconazole, clarithromycin). May reduce the efficacy with moderate or strong CYP3A inducers (e.g. bosentan, efavirenz, etravirine, modafinil, rifampicin, carbamazepine).
Food Interaction
Avoid concurrent use with St. John's wort as it may reduce the efficacy of lemborexant. Enhanced the CNS depressant effects with alcohol; avoid concomitant use. High-fat and high-calorie meal decreases the rate of absorption. Time to sleep onset may also be delayed if taken with or immediately after a meal.
Action
Description: Mechanism of Action: Lemborexant is a competitive oxerin receptor antagonist. It is thought to suppress the wake drive by inhibiting the binding of wake-promoting neuropeptides orexin A and orexin B to OX1R and OX2R receptors. Onset: Approx 15-20 minutes. Pharmacokinetics: Absorption: Rapidly absorbed. High-fat and high-calorie meal decreases the rate of absorption. Time to sleep onset may also be delayed if taken with or immediately after a meal. Time to peak plasma concentration: Approx 1-3 hours. Distribution: Volume of distribution: 1,970 L. Plasma protein binding: Approx 94% in vitro. Metabolism: Metabolised in the liver mainly by CYP3A4 and to a lesser extent by CYP3A5 into M10 (major circulating active metabolite). Excretion: Via faeces (57.4%); urine (29.1%; <1% as unchanged drug). Elimination half-life: 17-19 hours.
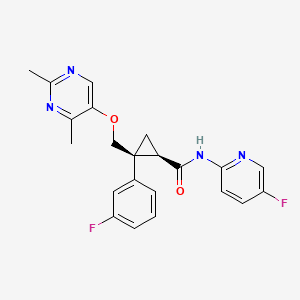
Chemical Structure
Lemborexant Source: National Center for Biotechnology Information. PubChem Compound Summary for CID 56944144, Lemborexant. https://pubchem.ncbi.nlm.nih.gov/compound/Lemborexant. Accessed Oct. 27, 2021.
Anon. Lemborexant. AHFS Clinical Drug Information [online]. Bethesda, MD. American Society of Health-System Pharmacists, Inc. https://www.ahfscdi.com. Accessed 01/09/2021.Anon. Lemborexant. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 01/09/2021.Dayvigo 5 mg, 10 mg Film-Coated Tablet (Eisai Hong Kong Co., Ltd.). MIMS Hong Kong. http://www.mims.com/hongkong. Accessed 01/09/2021.Dayvigo Tablet, Film Coated (Eisai Inc.). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed. Accessed 01/09/2021.



 Sign Out
Sign Out