


 Sign Out
Sign Out



Pharmacology: Pharmacodynamics: Mechanism of Action: Anti-capsular meningococcal antibodies protect against meningococcal disease via complement mediated bactericidal killing. Nimenrix induces the production of bactericidal antibodies against capsular polysaccharides of Neisseria meningitidis groups A, C, W-135 and Y when measured by assays using either rSBA or hSBA. By conjugating capsular polysaccharide to a protein carrier that contains T-cell epitopes, meningococcal conjugate vaccines like Nimenrix change the nature of immune response to capsular polysaccharide from T-cell independent to T-cell dependent.
Vaccine efficacy was inferred from the demonstration of immunologic non inferiority (based mainly on comparing proportions with rSBA titres at least 1:8) to licensed meningococcal vaccines. Immunogenicity was measured by using rSBA or hSBA which are biomarkers for protective efficacy against meningococcal groups A, C, W-135 and Y.
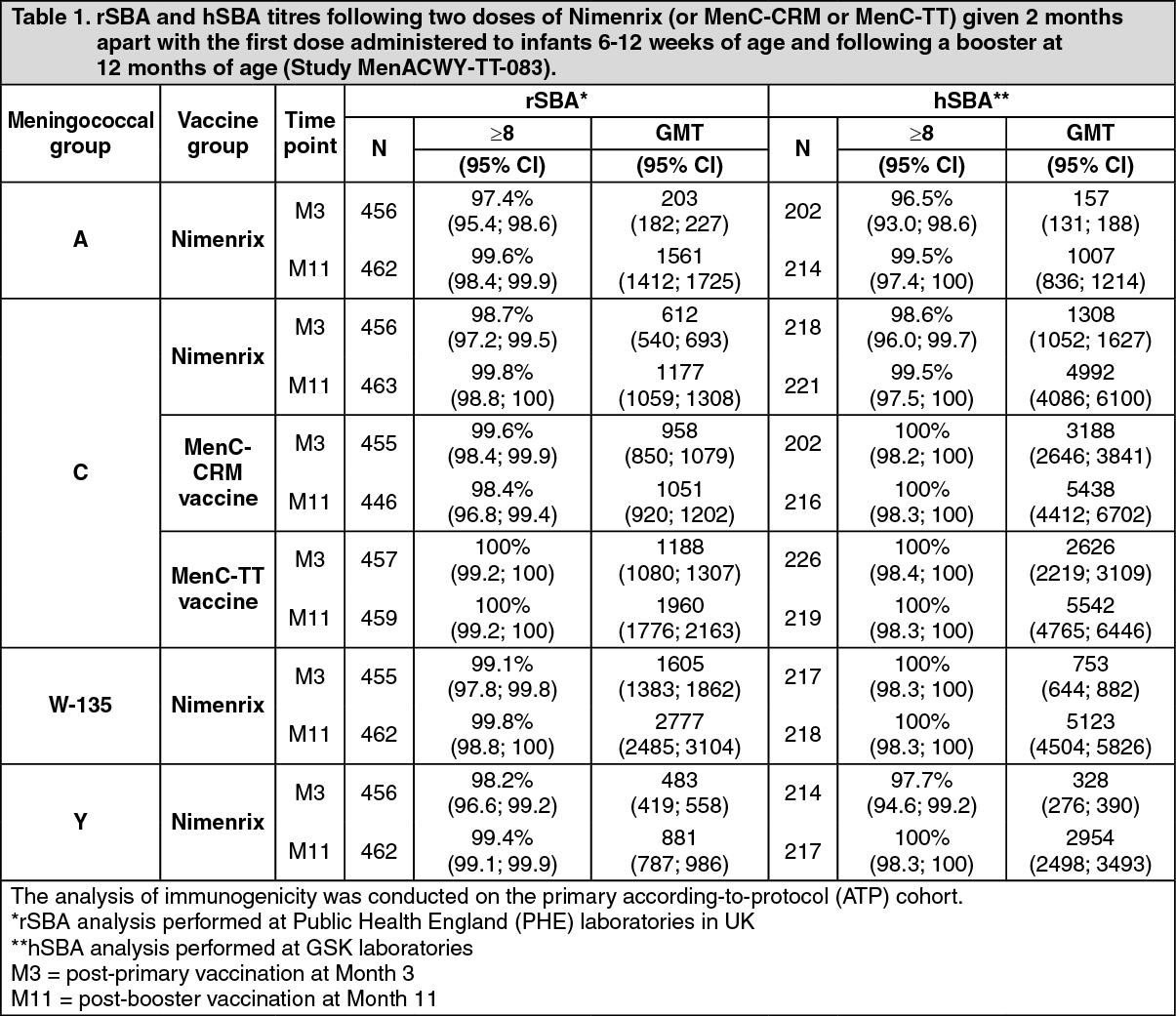
Immunogenicity in infants: In Study MenACWY-TT-083, the immunogenicity of a 2-dose primary vaccination schedule administered at 2 and 4 months of age was evaluated. Routinely used infant vaccines DTaP/IPV/Hib/HepB and a 10-valent pneumococcal vaccine were co-administered. For group C, rSBA and hSBA titres elicited by Nimenrix were compared to a 2-dose priming with licensed monovalent meningococcal conjugate group C vaccines, MenC-CRM and MenC-TT vaccines. Nimenrix elicited rSBA and hSBA titres against the four meningococcal groups. The response against group C was non-inferior to the one elicited by the licensed MenC-CRM and MenC-TT vaccines in terms of the percentage of subjects with rSBA titres ≥8 at 1 month after the second dose.
For subjects initially vaccinated in infancy with Nimenrix at 2 and 4 months of age and receiving a Nimenrix booster dose at 12 months of age, the increase in rSBA and hSBA titres 1 month post-booster dose ranged between 15 and 80-fold for all groups and more than 99.0% of all infants achieved post-booster titres above 8 for both assays. The observed booster response for group C was similar to that observed in subjects primed and boosted with a monovalent MenC conjugate vaccine (TT or CRM conjugated). Results are shown in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
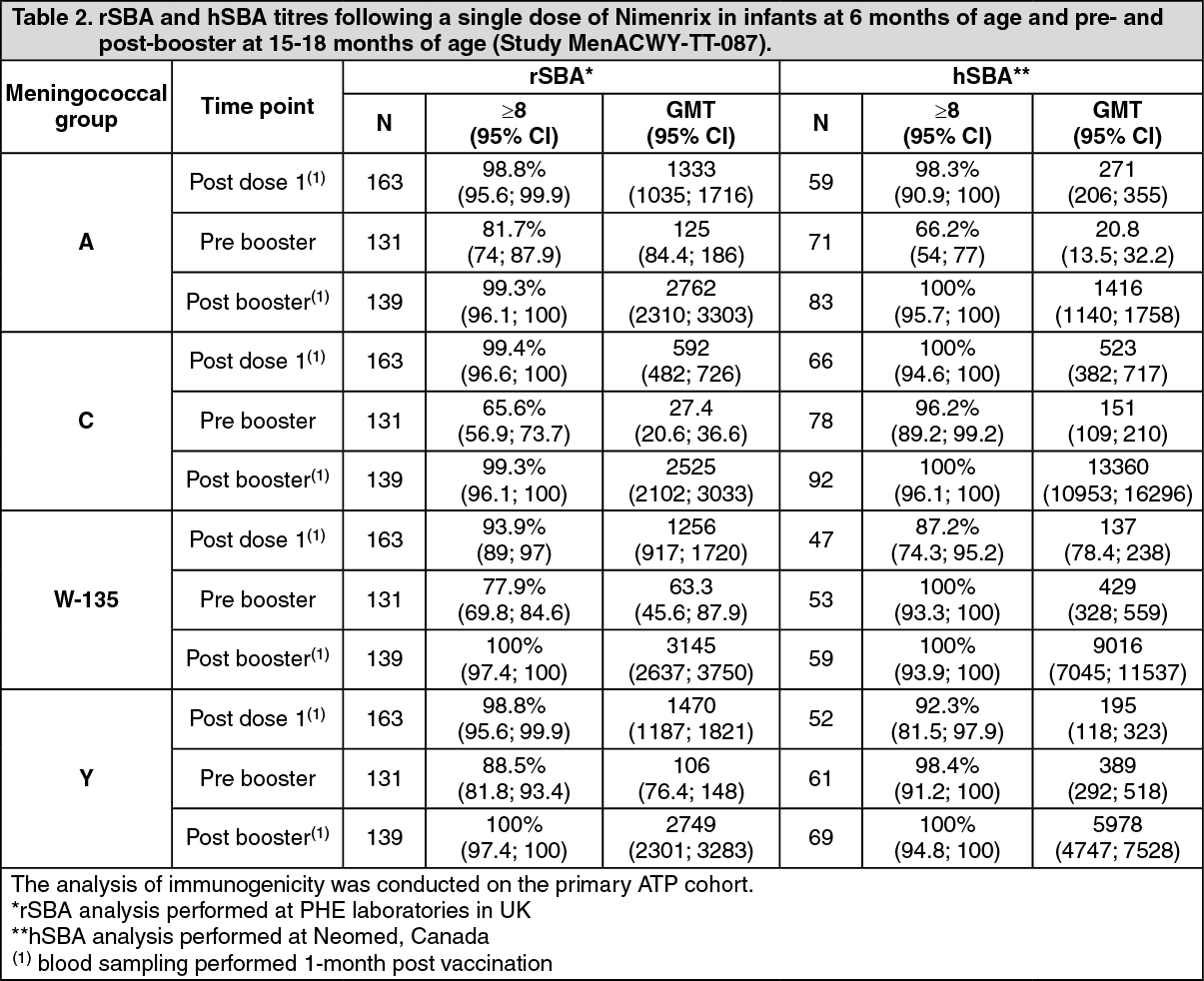
Click on icon to see table/diagram/imageIn Study MenACWY-TT-087, infants received either a single primary dose at 6 months followed by a booster dose at 15-18 months or three primary doses at 2, 4, and 6 months followed by a booster dose at 15-18 months. All subjects also received DTaP-IPV/Hib and 10-valent pneumococcal conjugate vaccines at all time points. A single primary dose administered at 6 months of age elicited robust rSBA titres to the four meningococcal groups, as measured by the percentage of subjects with rSBA titres ≥8, that were comparable to responses after the last dose of a three-dose primary series. A booster dose produced robust responses, comparable between the two dosing groups, against all four meningococcal groups. Results are shown in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMeasurement of hSBA titres was a secondary endpoint in Study MenACWY-TT-087. Although similar responses to groups A and C were observed with both dosing schedules, a single primary dose in infants at 6 months was associated with lower hSBA titres to groups W-135 and Y as measured by the percentage of subjects with hSBA titres ≥8 [87.2% (95% CI: 74.3; 95.2) and 92.3% (95% CI: 81.5; 97.9), respectively] compared with three primary doses at 2, 4, and 6 months of age [100% (95% CI: 96.6; 100) and 100% (95% CI: 97.1; 100), respectively] (see Precautions). After a booster dose, hSBA titres to all four meningococcal groups were comparable between the two dosing schedules (Table 2).
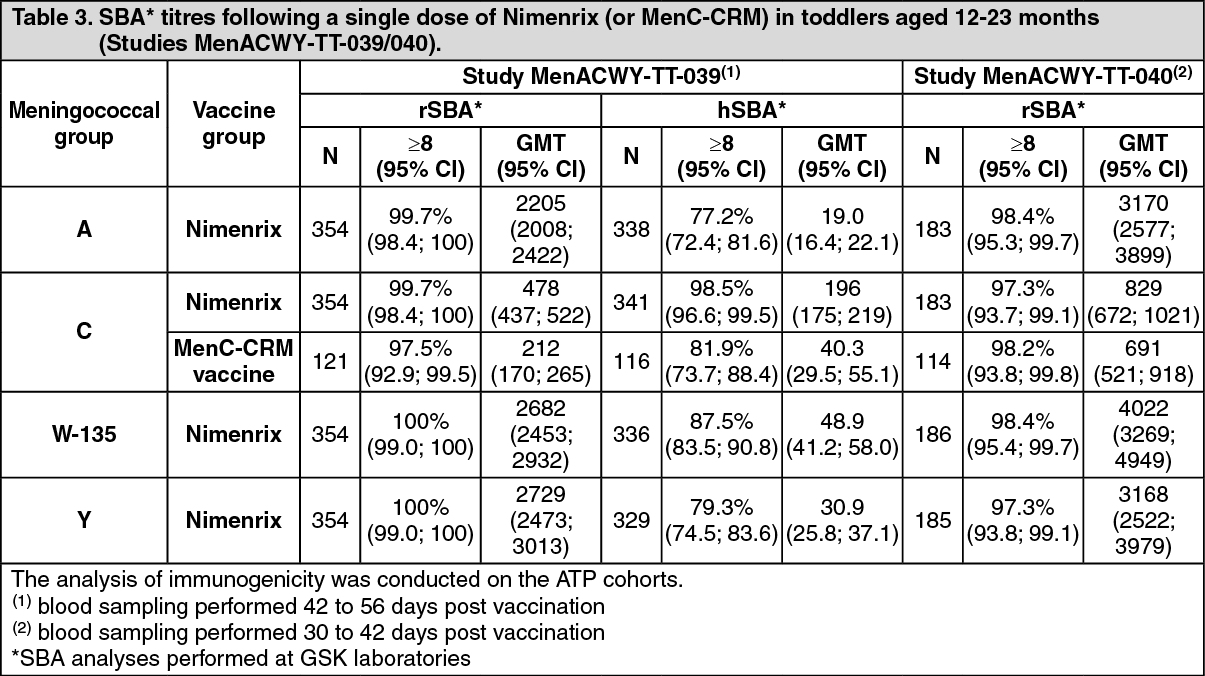
Immunogenicity in toddlers aged 12-23 months: In clinical studies MenACWY-TT-039 and MenACWY-TT-040, a single dose of Nimenrix elicited SBA titres against the four meningococcal groups, with group C rSBA titres that were comparable to those elicited by a licensed MenC-CRM vaccine in terms of the percentage of subjects with rSBA titres ≥8. In Study MenACWY-TT-039, hSBA was also measured as a secondary endpoint. Results are shown in Table 3. (See Table 3.)
 Click on icon to see table/diagram/image
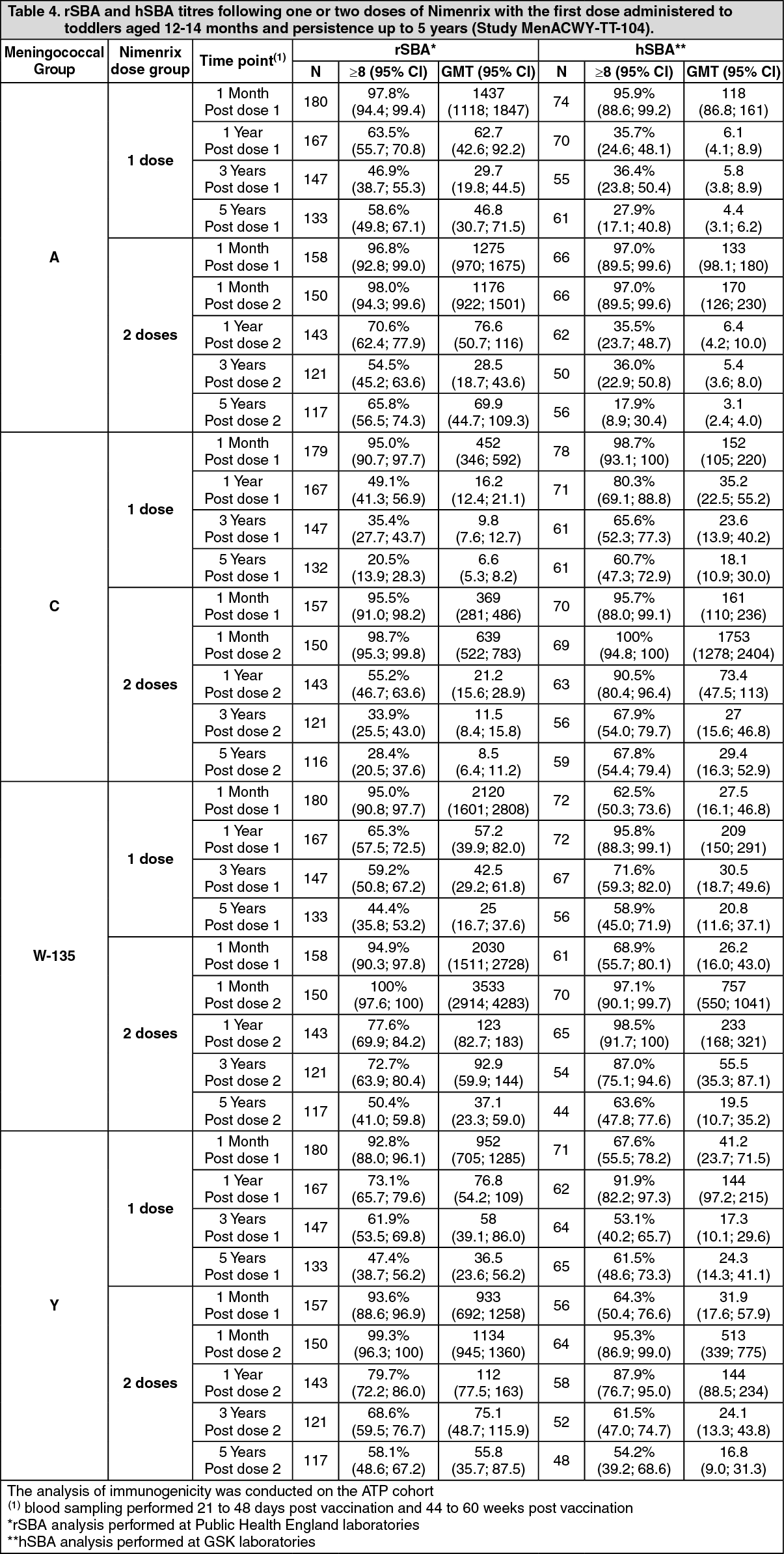
Click on icon to see table/diagram/imageLong term immunogenicity in toddlers: Study MenACWY-TT-104 evaluated the immunogenicity after 1 month and the persistence of the response up to 5 years following 1 or 2 doses (given 2 months apart) of Nimenrix in toddlers aged 12 to 14 months. One month following one or two doses administered 2 months apart Nimenrix elicited rSBA titres against all four meningococcal groups that were similar in terms of the percentage of subjects with rSBA titre ≥8 and GMT. As a secondary endpoint hSBA titres were measured. In terms of the percentage of subjects with hSBA titres ≥8, at 1 month post vaccination, hSBA titres against groups W-135 and Y were higher after two doses of Nimenrix than after one dose, while the hSBA titres against groups A and C were similar in the two dose groups. At Year 5 only a small difference in antibody persistence between one and two doses was observed, in terms of percentages of subjects with hSBA titres ≥8 against all groups. Antibody persistence was observed at Year 5 against groups C, W-135 and Y. After one and two doses the percentages of subjects with hSBA titres ≥8 for group C were 60.7% and 67.8%, group W-135 were 58.9% and 63.6% and group Y were 61.5% and 54.2%, respectively. For group A, 27.9% and 17.9% of subjects receiving one or two doses, respectively, had hSBA titres ≥8. (See Table 4.)
 Click on icon to see table/diagram/image
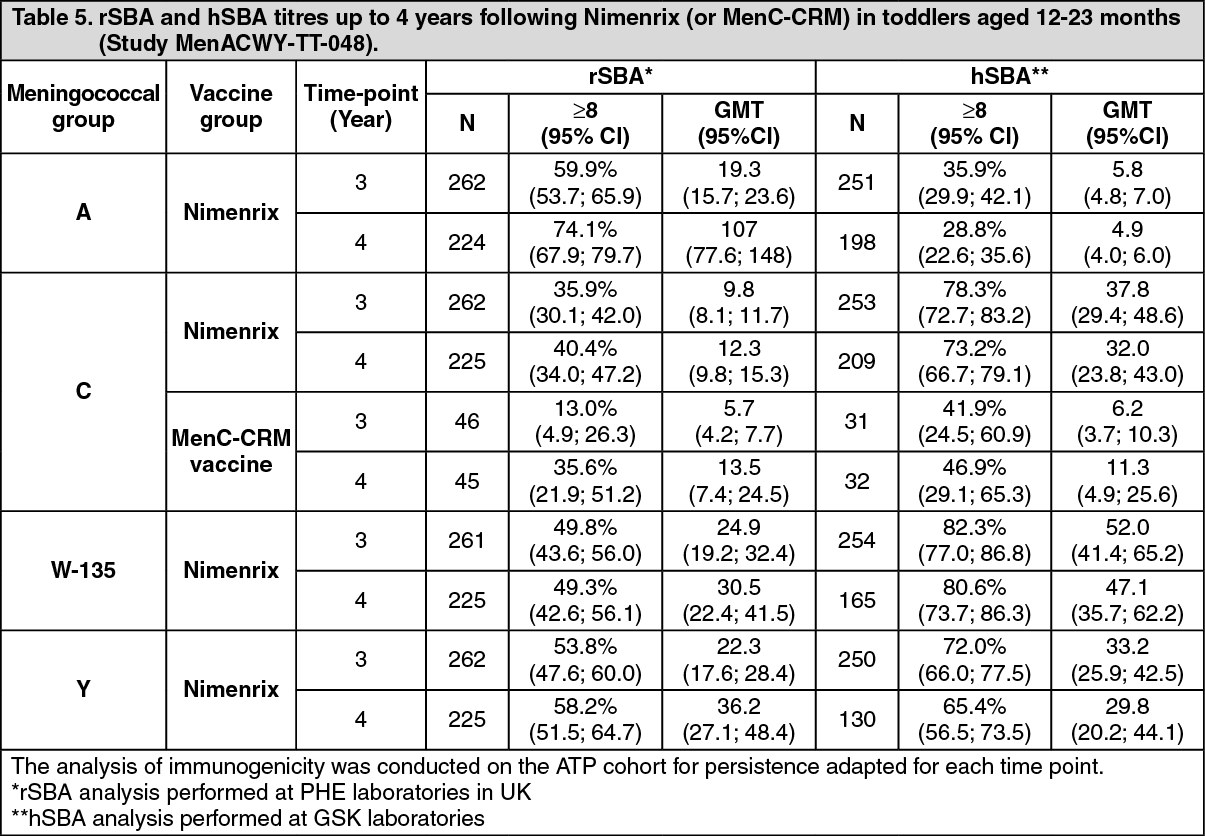
Click on icon to see table/diagram/imageIn children vaccinated at toddler age, the persistence of rSBA and hSBA titres was evaluated up to 4 years in Study MenACWY-TT-048. Results are shown in Table 5. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagerSBA and hSBA titres were determined over a period of 10 years in children initially vaccinated with one dose of Nimenrix or MenC-CRM at 12 to 23 months of age in Study MenACWY-TT-027. Persistence of SBA titres was evaluated in two extension studies: MenACWY-TT-032 (up to 5 years) and MenACWY-TT-100 (up to 10 years). Study MenACWY-TT-100 also evaluated the response to a single booster dose of Nimenrix administered 10 years following the initial vaccination with Nimenrix or MenC-CRM. Results are shown in Table 6 (see Precautions). (See Table 6.)
 Click on icon to see table/diagram/image
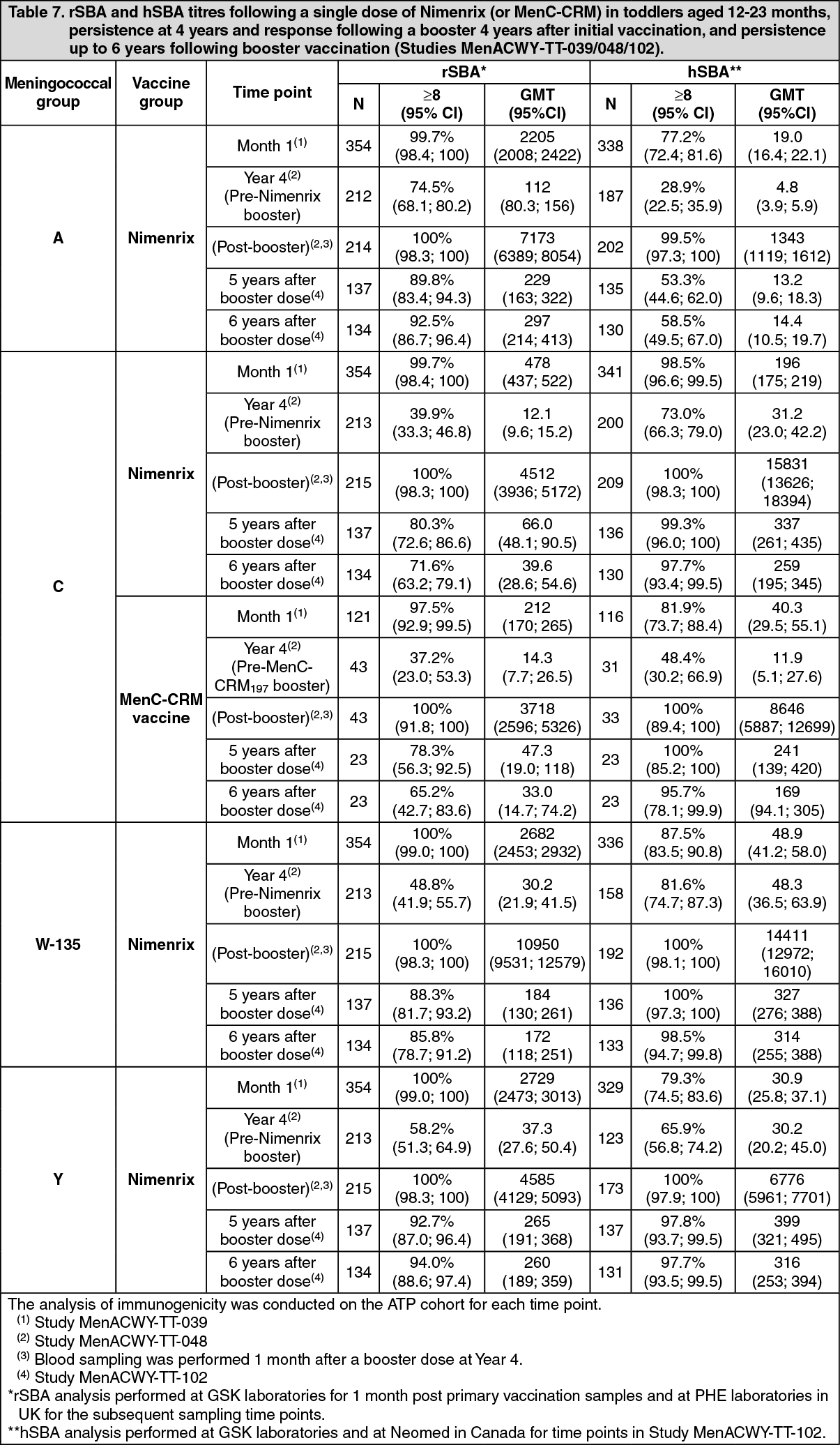
Click on icon to see table/diagram/imagePersistence of booster response: Study MenACWY-TT-102 evaluated the persistence of SBA titres up to 6 years after a booster dose of Nimenrix or MenC-CRM197 administered in Study MenACWY-TT-048 to children who initially received the same vaccine at 12 to 23 months of age in Study MenACWY-TT-039. A single booster dose was administered 4 years after the initial vaccination. Results are shown in Table 7 (see Precautions). (See Table 7.)
 Click on icon to see table/diagram/image
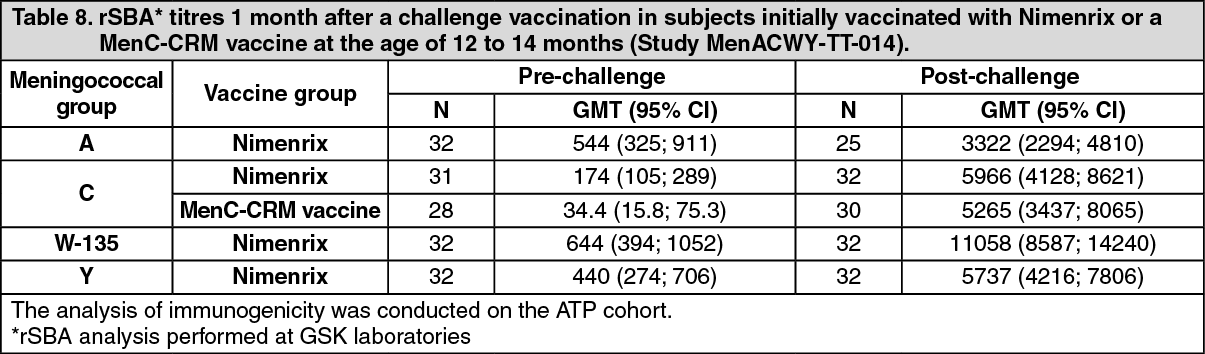
Click on icon to see table/diagram/imageImmune memory: In Study MenACWY-TT-014, the induction of immune memory was assessed 1 month after the administration of a fifth of the dose of ACWY-PS vaccine (10 µg of each polysaccharide) to children in the third year of life initially vaccinated in Study MenACWY-TT-013 with Nimenrix or a licensed MenC-CRM vaccine at the age of 12 to 14 months.
One month after the challenge dose, the GMTs elicited by the initial vaccination with Nimenrix increased by 6.5 to 8 fold for groups A, C, W-135, and Y, indicating that Nimenrix induces immune memory to all four meningococcal groups. The post-challenge rSBA-MenC GMT was similar in both study groups, indicating that Nimenrix induces an analogous immune memory to group C as the licensed MenC-CRM vaccine. Results are shown in Table 8. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageImmunogenicity in children aged 2-10 years: In two comparative studies conducted in subjects aged 2-10 years, one group of subjects received a dose of Nimenrix and a second group a dose of either a licensed MenC-CRM vaccine (Study MenACWY-TT-081) or the licensed ACWY-PS vaccine (Study MenACWY-TT-038) as comparator.
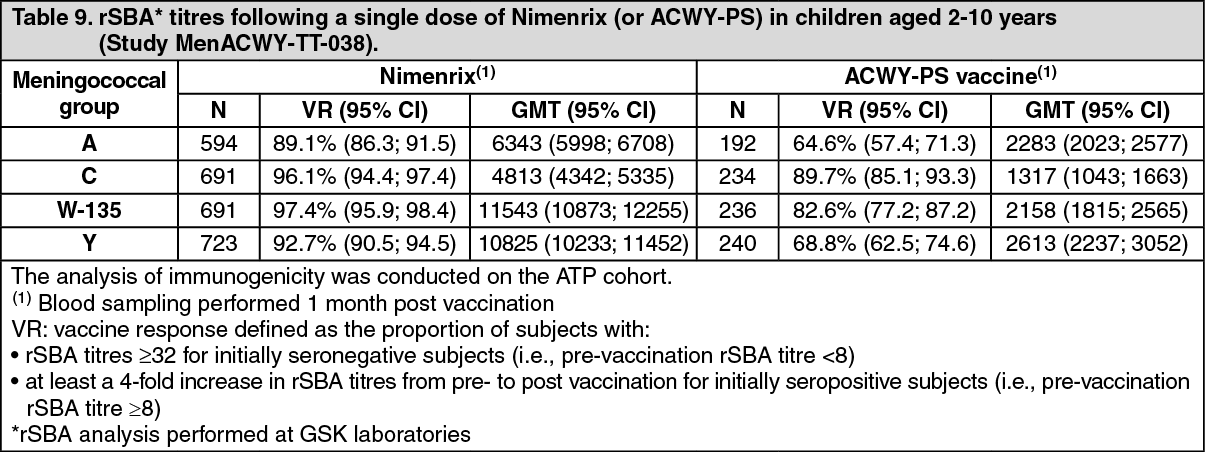
In Study MenACWY-TT-038, a single dose of Nimenrix was demonstrated to be non-inferior to the licensed ACWY-PS vaccine in terms of vaccine response to the four meningococcal groups as shown in Table 9. (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn Study MenACWY-TT-081, a single dose of Nimenrix (N = 268) was demonstrated to be non-inferior to another licensed MenC-CRM vaccine (N = 92) in terms of vaccine response to group C [94.8% (95% CI: 91.4; 97.1) and 95.7% (95% CI: 89.2; 98.8), respectively]. GMTs were lower for the Nimenrix group [2795 (95% CI: 2393; 3263)] versus the MenC-CRM vaccine [5292 (95% CI: 3815; 7340)].
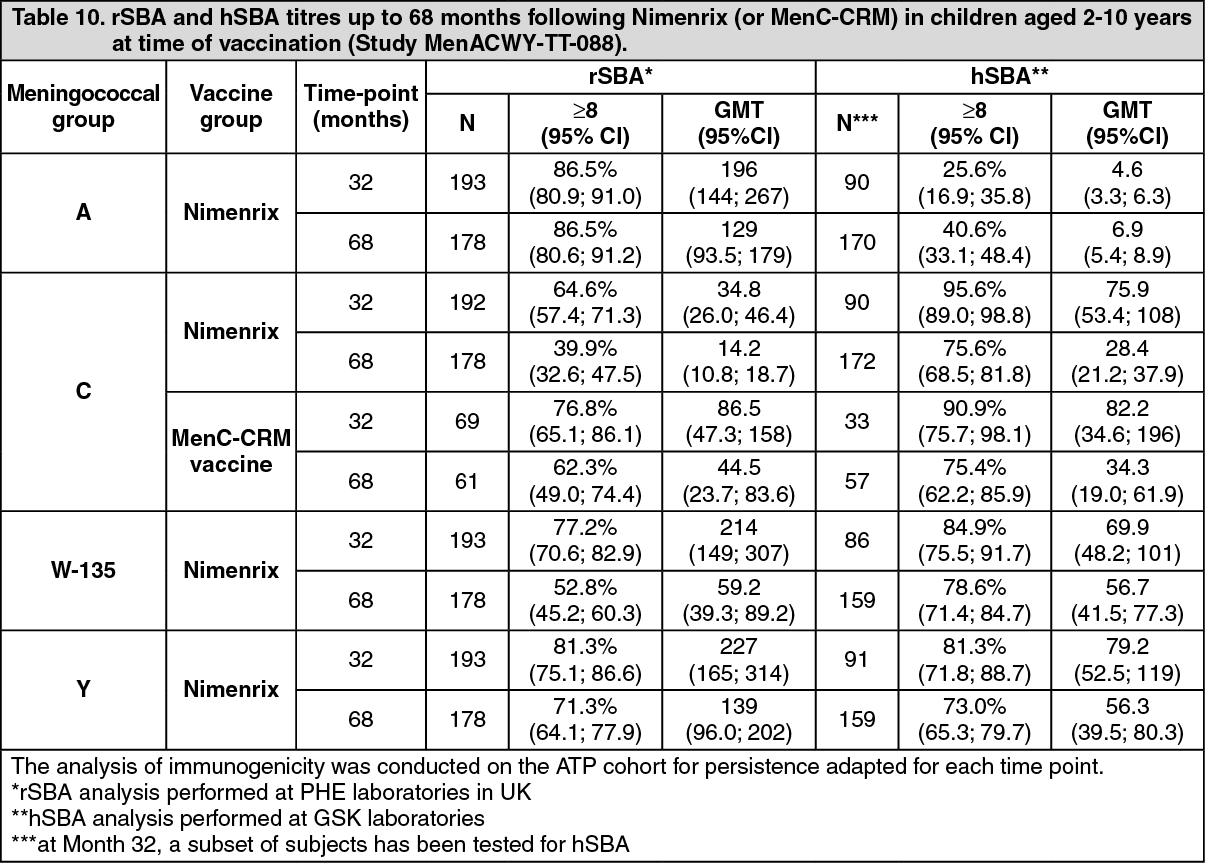
In Study MenACWY-TT-088, the persistence of SBA titres was evaluated up to 68 months after vaccination in children 2-10 years of age initially vaccinated in Study MenACWY-TT-081. Results are shown in Table 10 (see Precautions). (See Table 10.)
 Click on icon to see table/diagram/image
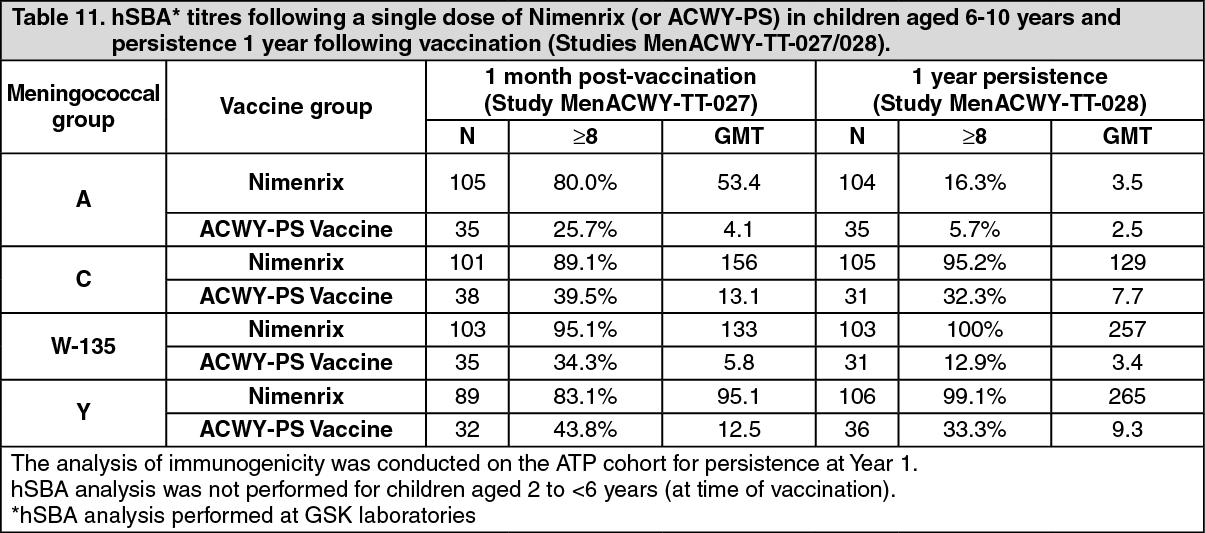
Click on icon to see table/diagram/imageIn Study MenACWY-TT-028, the persistence of hSBA titres was evaluated 1 year after vaccination in children aged 6-10 years who were initially vaccinated in Study MenACWY-TT-027. Results are shown in Table 11. (See Table 11.)
 Click on icon to see table/diagram/image
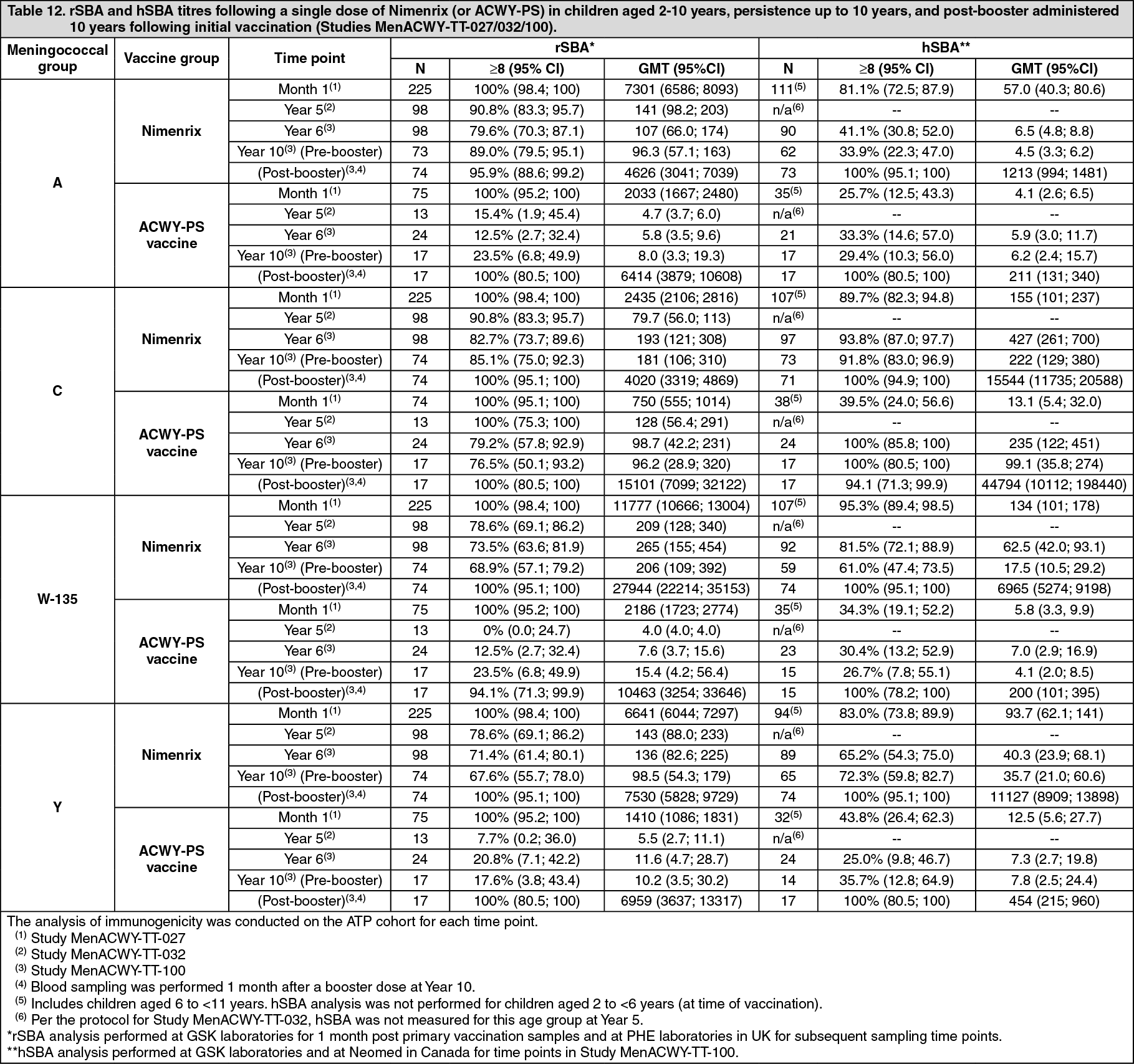
Click on icon to see table/diagram/imageSBA titres were determined over a period of 10 years in children initially vaccinated with one dose of Nimenrix or ACWY-PS at 2 to 10 years of age in Study MenACWY-TT-027. Persistence of SBA titres was evaluated in two extension studies: MenACWY-TT-032 (up to 5 years) and MenACWY-TT-100 (up to 10 years).
Study MenACWY-TT-100 also evaluated the response to a single booster dose of Nimenrix administered 10 years following the initial vaccination with Nimenrix or ACWY-PS. Results are shown in Table 12 (see Precautions). (See Table 12.)
 Click on icon to see table/diagram/image
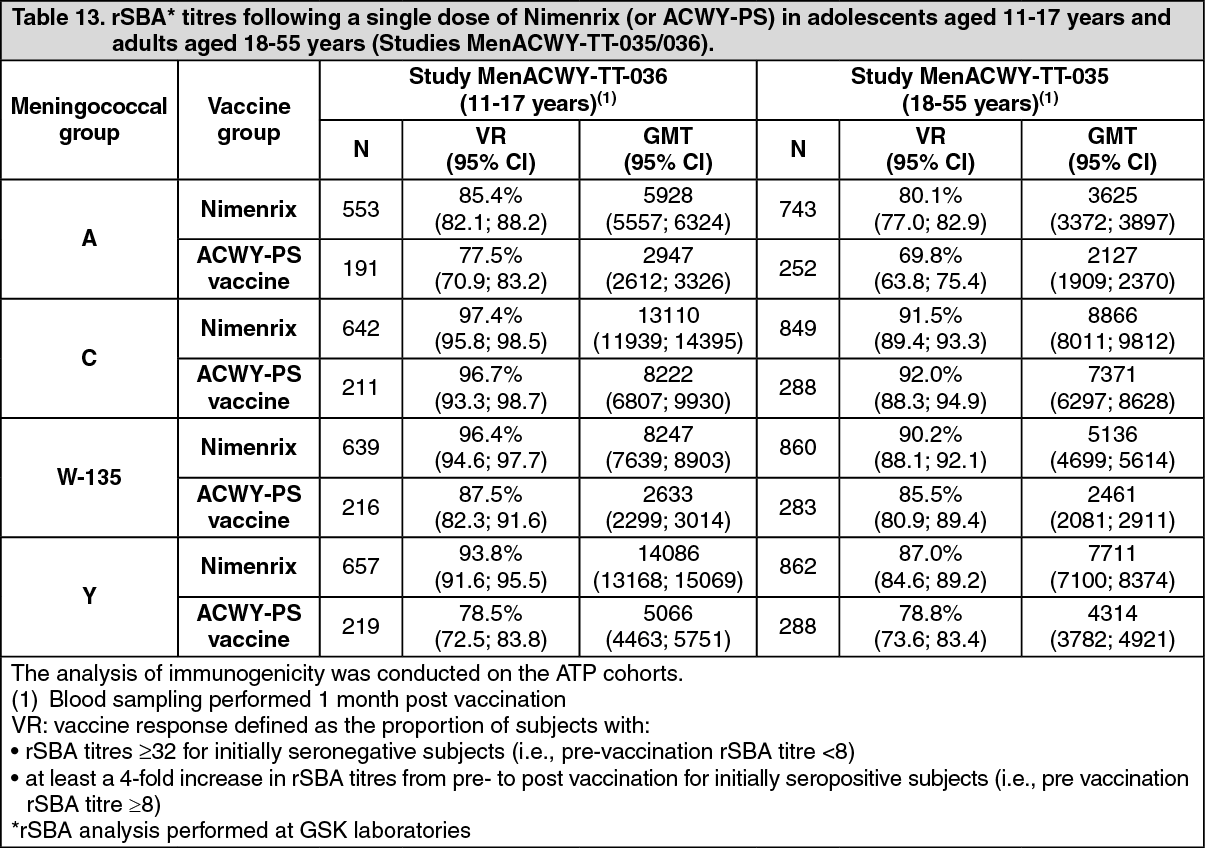
Click on icon to see table/diagram/imageImmunogenicity in adolescents aged 11-17 years and adults aged ≥18 years: In two clinical studies, conducted in adolescents aged 11-17 years (Study MenACWY-TT-036) and in adults aged 18-55 years (Study MenACWY-TT-035), either one dose of Nimenrix or one dose of the ACWY-PS vaccine was administered.
In both adolescents and adults, Nimenrix was demonstrated to be immunologically non-inferior to the ACWY-PS vaccine in terms of vaccine response. rSBA titres to the four meningococcal groups elicited by Nimenrix were either similar to or higher than those elicited by the ACWY-PS vaccine as shown in Table 13. (See Table 13.)
 Click on icon to see table/diagram/image
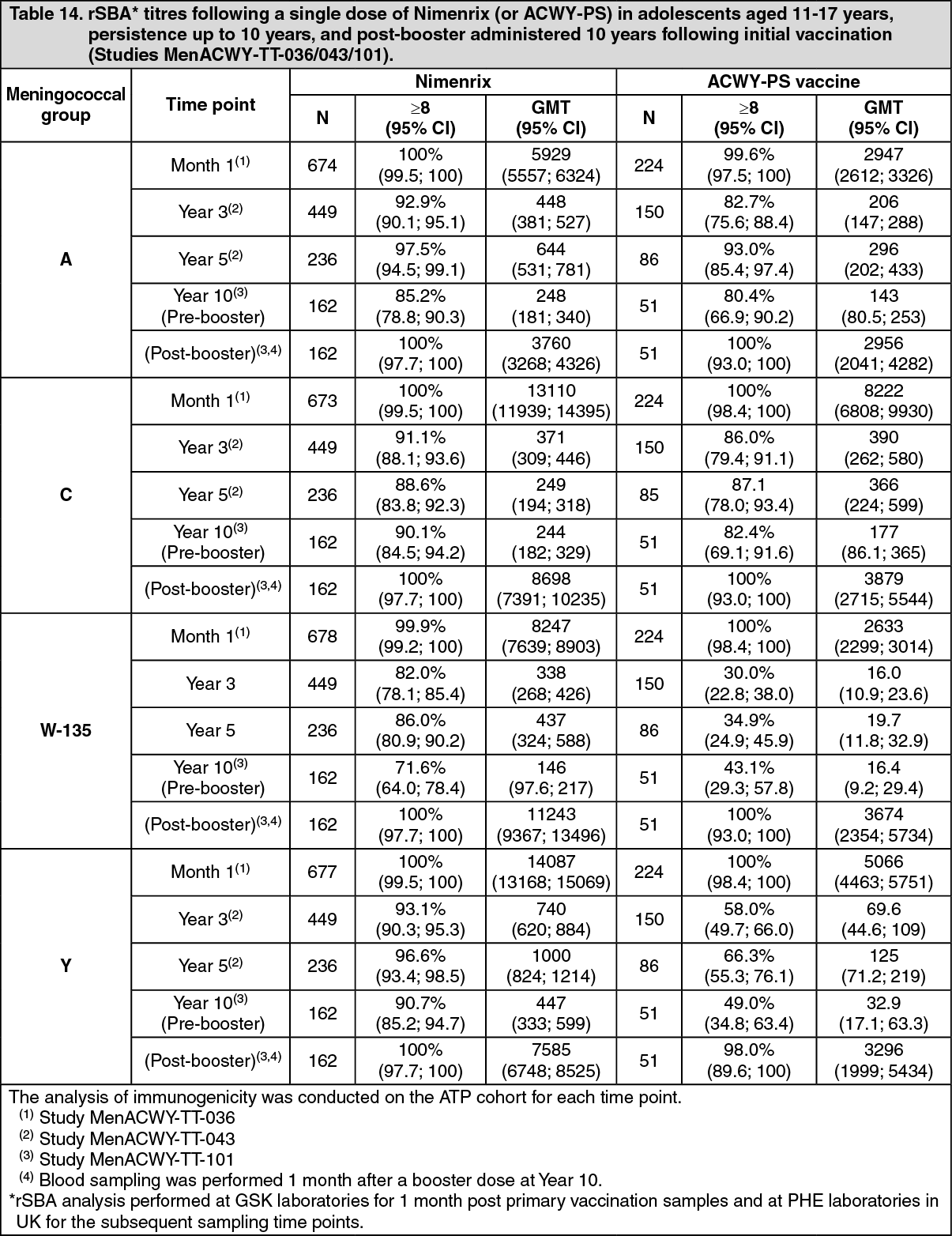
Click on icon to see table/diagram/imagerSBA titres were determined over a period of 10 years in subjects initially vaccinated with one dose of Nimenrix or ACWY-PS at 11 to 17 years of age in Study MenACWY-TT-036. Persistence of rSBA titres was evaluated in two extension studies: MenACWY-TT-043 (up to 5 years) and MenACWY-TT-101 (at 10 years). Study MenACWY-TT-101 also evaluated the response to a single booster dose of Nimenrix administered 10 years following the initial vaccination with Nimenrix or ACWY-PS. Results are shown in Table 14. (See Table 14.)
 Click on icon to see table/diagram/image
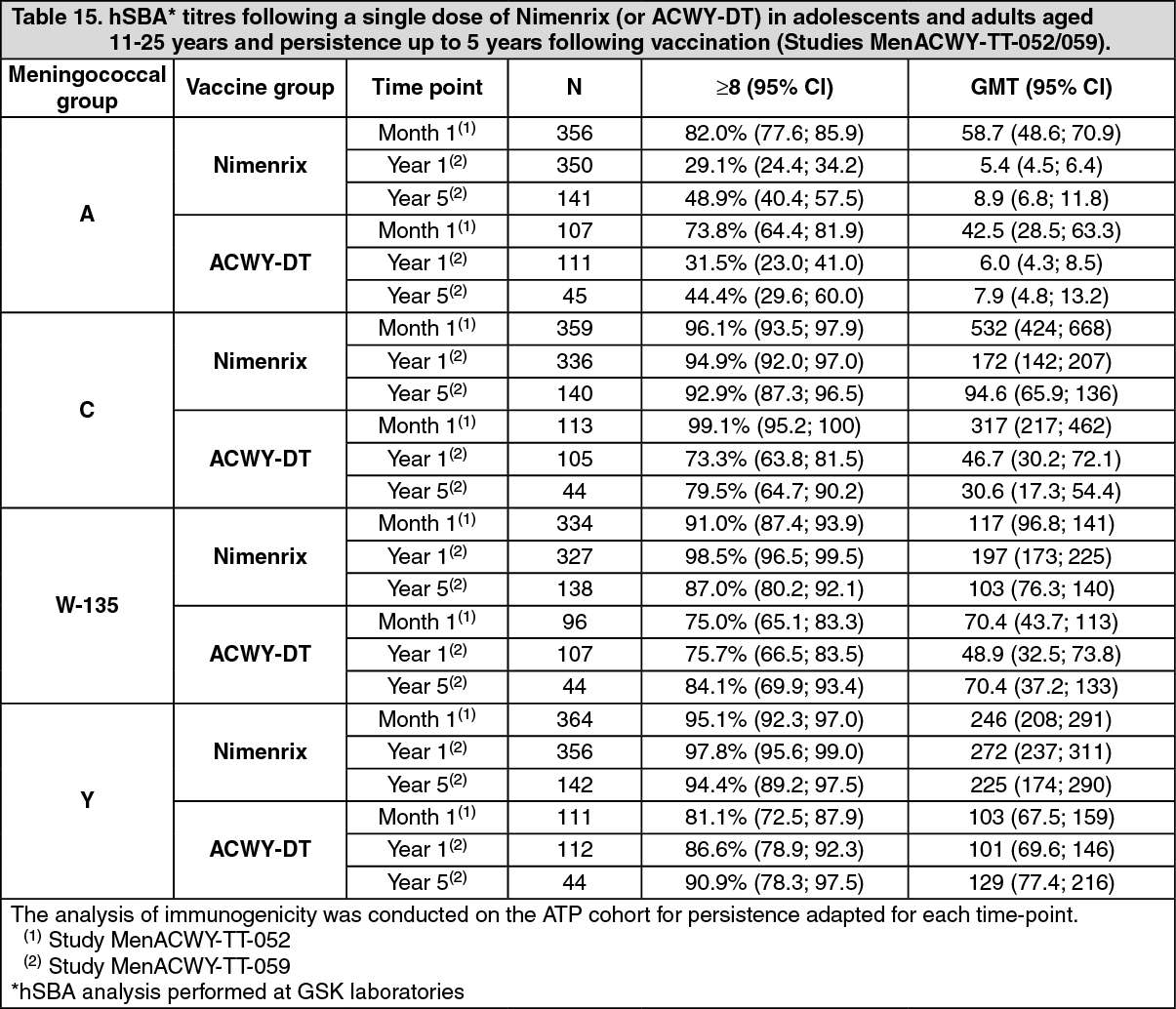
Click on icon to see table/diagram/imageIn Study MenACWY-TT-059, hSBA persistence was evaluated up to 5 years after vaccination in adolescents and adults aged 11-25 years initially vaccinated in Study MenACWY-TT-052.
For all meningococcal groups, the persistence of hSBA titres elicited by Nimenrix was similar to or higher than those induced by the licensed quadrivalent meningococcal diphtheria toxoid (DT) conjugate (ACWY-DT) vaccine as shown in Table 15. (See Table 15.)
 Click on icon to see table/diagram/image
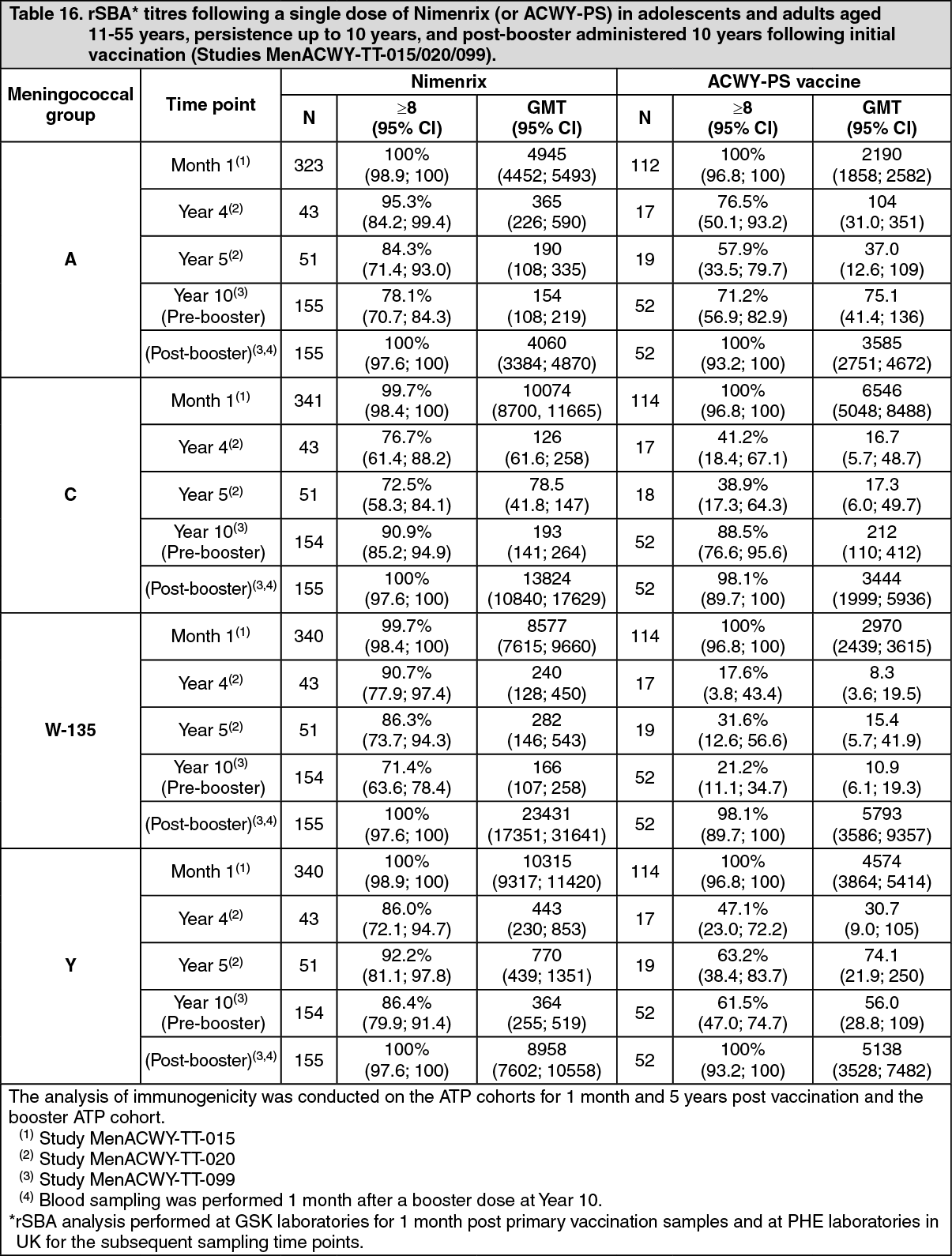
Click on icon to see table/diagram/imagerSBA titres were determined over a period of 10 years in subjects initially vaccinated with one dose of Nimenrix or ACWY-PS at 11 to 55 years of age in Study MenACWY-TT-015. Persistence of rSBA titres was evaluated in two extension studies: MenACWY-TT-020 (up to 5 years) and MenACWY-TT-099 (up to 10 years). Study MenACWY-TT-099 also evaluated the response to a single booster dose of Nimenrix administered 10 years following the initial vaccination with Nimenrix or ACWY-PS. Results are shown in Table 16. (See Table 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn a descriptive study conducted in 194 adults aged 56 years and older (Study MenACWY-TT-085), Nimenrix was immunogenic, with a vaccine response rate ≥63.4% and with ≥97.4% of subjects with rSBA titres ≥8 against all four meningococcal groups. Moreover, at least 93.2% of subjects achieved the more conservative threshold of protection of rSBA titres ≥128.
Booster response for subjects previously vaccinated with a conjugate meningococcal vaccine against Neisseria meningitidis: Nimenrix booster vaccination in subjects previously primed with a monovalent (MenC-CRM) or a quadrivalent conjugate meningococcal vaccine (MenACWY-TT) was studied in subjects from 12 months of age onwards who received a booster vaccination. Robust anamnestic responses to the antigen(s) in the priming vaccine were observed (see Tables 6, 7, 12, 14, and 16).
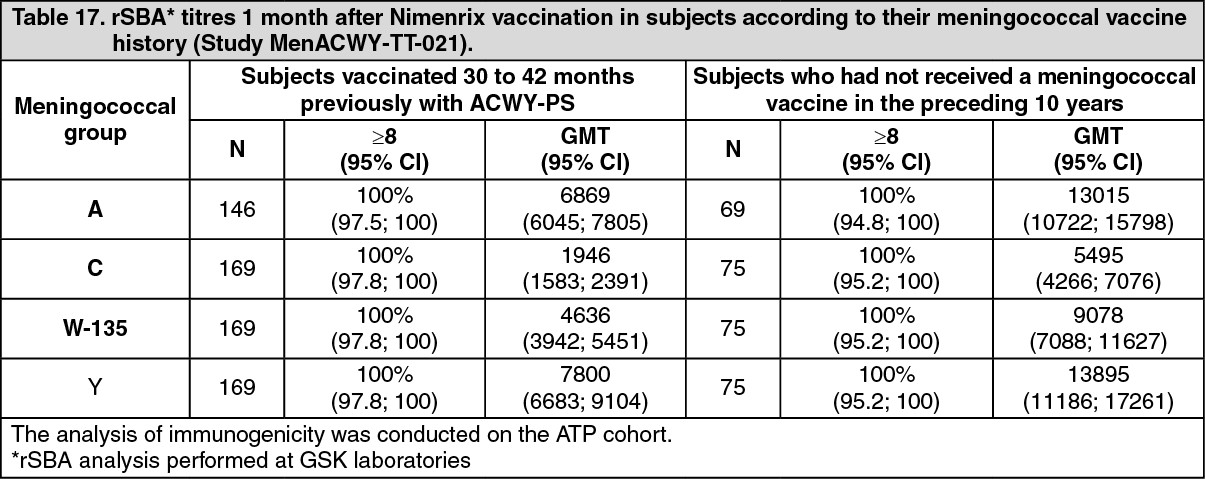
Response to Nimenrix in subjects previously vaccinated with a plain polysaccharide meningococcal vaccine against Neisseria meningitidis: In Study MenACWY-TT-021 conducted in subjects aged 4.5-34 years, the immunogenicity of Nimenrix administered between 30 and 42 months after vaccination with a ACWY-PS vaccine was compared to the immunogenicity of Nimenrix administered to age-matched subjects who had not been vaccinated with any meningococcal vaccine in the preceding 10 years. The rSBA GMTs were significantly lower in the subjects who had received a dose of ACWY-PS vaccine 30-42 months prior to Nimenrix. The clinical relevance of this observation is unknown since all subjects achieved rSBA titres ≥8 for all four meningococcal groups. Results are shown in Table 17. (See Table 17.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageImmunogenicity in children aged 2-17 years with anatomical or functional asplenia: Study MenACWY-TT-084 evaluated the immunogenicity of one and two doses of Nimenrix given 2 months apart in 43 at-risk subjects aged 2-17 years (at increased risk for meningococcal disease, i.e., asplenic subjects, and hyposplenic subjects) compared to 43 healthy age-matched subjects.
One month after the first vaccine dose, vaccine response rates (rSBA titre ≥1:32 or a ≥4-fold increase in rSBA titre from baseline) for groups A, C, W-135, and Y, respectively, were 100%, 92.5%, 100% and 97.5% in the at-risk group and were 97.5%, 97.5%, 97.5%, and 100% for healthy subjects. After the second vaccine dose, vaccine response rates in both at-risk and healthy subjects were 100% for each of the four meningococcal groups.
One month after Vaccination 1, hSBA response rates for groups A, C, W-135, and Y, respectively, were 69.7%, 77.1%, 55.6%, and 60.5% in the at-risk group and were 69.7%, 60.6%, 65.5%, and 76.3%, in the healthy group. One month after Vaccination 2, hSBA response rates were 84.8%, 100%, 80.6% and 73.0%, in the at-risk group and 75.0%, 85.3%, 77.4%, and 73.0% in the healthy group.
Impact of a single dose of Nimenrix: The Netherlands introduced Nimenrix into the national immunization program in 2018 as a single dose at 14 months of age. A catch-up campaign for individuals 14-18 years of age initiated in 2018 and in 2020 a single dose of Nimenrix at 14 years of age became routine, resulting in a toddler and adolescent national immunization program. Within two years, the incidence of meningococcal disease caused by groups C, W, and Y was significantly reduced by 100% (95% CI: 14, 100) in individuals 14-18 years of age, 85% (95% CI: 32, 97) in all vaccine eligible ages (direct effect), and 50% (95% CI: 28, 65) in non-vaccine eligible ages (indirect effect). In children 15 to 36 months, there were only 3 cases during the pre-vaccination period and 2 cases in the post-vaccination period, resulting in an IRR of 33% (95% CI: -302, 89). The low number of cases among this age group, does not allow for a reliable assessment of vaccine impact as indicated by the wide 95% CIs.
Pharmacokinetics: Not relevant for vaccines.
Toxicology: Preclinical Safety Data: Non-clinical data reveal no special hazard for humans based on local tolerance, acute toxicity, repeated dose toxicity, developmental/reproductive toxicity and fertility studies.