


 Sign Out
Sign Out


Pharmacology: Pharmacodynamics: The omega-3 series polyunsaturated fatty acids, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), are essential fatty acids.
Omacor acts on plasma lipids by lowering triglyceride levels resulting in a fall in VLDL (very low density lipoprotein), and the substance is also active on haemostasis and blood pressure.
Omacor reduces the synthesis of triglycerides in the liver because EPA and DHA are poor substrates for the enzymes responsible for triglyceride synthesis and they inhibit esterification of other fatty acids.
The increase in peroxisomes of β-oxidation of fatty acids in the liver also contributes to the fall in triglycerides, by reducing the quantity of free fatty acids available for their synthesis. The inhibition of this synthesis lowers VLDL.
Omacor increases LDL-Cholesterol in some patients with hypertriglyceridaemia. Rises in HDL-Cholesterol are only small, significantly smaller than seen after administration of fibrates, and occur inconsistently.
The long-term lipid-lowering effect (after more than one year) is not known. Furthermore, there is no strong evidence that lowering triglycerides reduces the risk of ischaemic heart disease.
During treatment with Omacor, there is a fall in thromboxane A2 production and a slight increase in bleeding time. No significant effect has been observed on the other coagulation factors.
Hypertriglyceridaemia: There have been eight double-blind, parallel group, placebo-controlled studies in hypertriglyceridaemia, using Omacor 4 g per day. These eight studies are the pivotal studies. These studies included seven individual studies and one part of a study that evaluated Omacor 2 g, 4 g, 8 g, and placebo treatment arms.
The duration of the eight pivotal studies was short term (maximum 12 weeks).
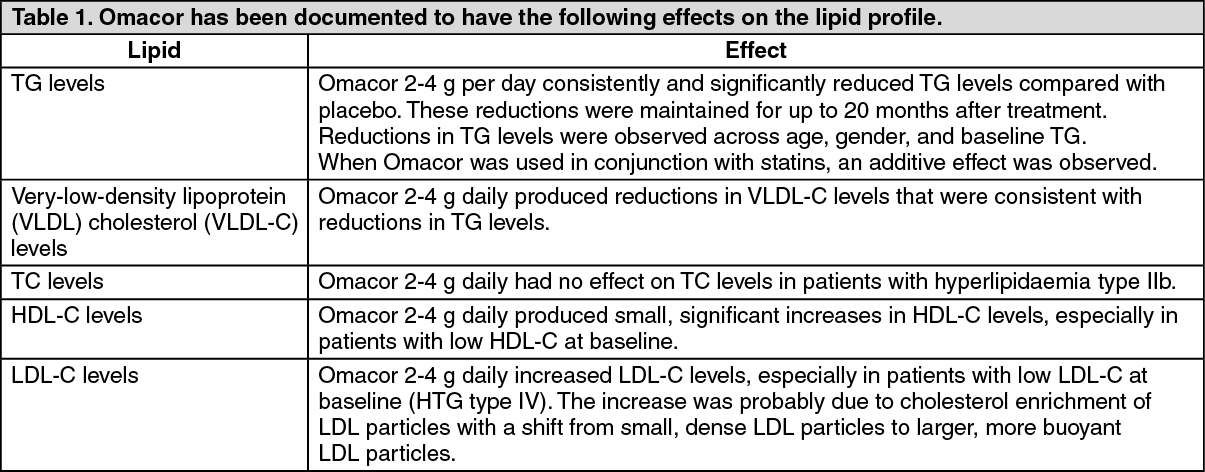
Numerous studies in patients with hypertriglyceridemia have been conducted with Omacor, with variable designs: double-blind studies, placebo-controlled studies, randomised studies, open studies and long term studies (up to 24 months). Omacor at doses of 4 g per day consistently and significantly reduced triglycerides levels compared to placebo. The studies have shown that the reductions were maintained for up to 24 months after treatment. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe following table summarises the median percent changes in lipid parameters from baseline in the overall population, and in patients with Types IIb, IV and V dyslipidaemia. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageRemarks: The documented number of patients enrolled in clinical trials with Type III dyslipidaemia is very limited, and no studies were designed to especially investigate the effect of Omacor in these patients. Type III dyslipidaemic patients are homozygotes for ApoE, and genotyping of patients was only performed in one study (K85-95011). More Type III dyslipidaemic patients may have been therefore enrolled in clinical studies without being verified as such. There is no reason to believe that Type III dyslipidaemic patients do not respond to Omacor.
One of the pivotal clinical trials in patients with type IV and V dyslipidaemia (K85-95009 study) demonstrated a mean LDL-C increase of 42.6% with Omacor 4 g/day. 67% of the patients in the study experienced increases in LDL-C, and the increases observed were in the range of 6%-110%. However, mean LDL-C concentrations at the end of the study were still only equal to 2.69 mmol/L (104 mg/dL). For the majority of these patients (40 of 42 with no history of coronary disease) this is still below their target LDL-C levels.
In clinical trials on patients with Type IIb dyslipidaemia mean LDL-C is unchanged or slightly increased (maximum 8.6%) with Omacor treatment. In studies with concomitant treatment of Omacor and a statin no significant increase in LDL-C has been observed with Omacor.
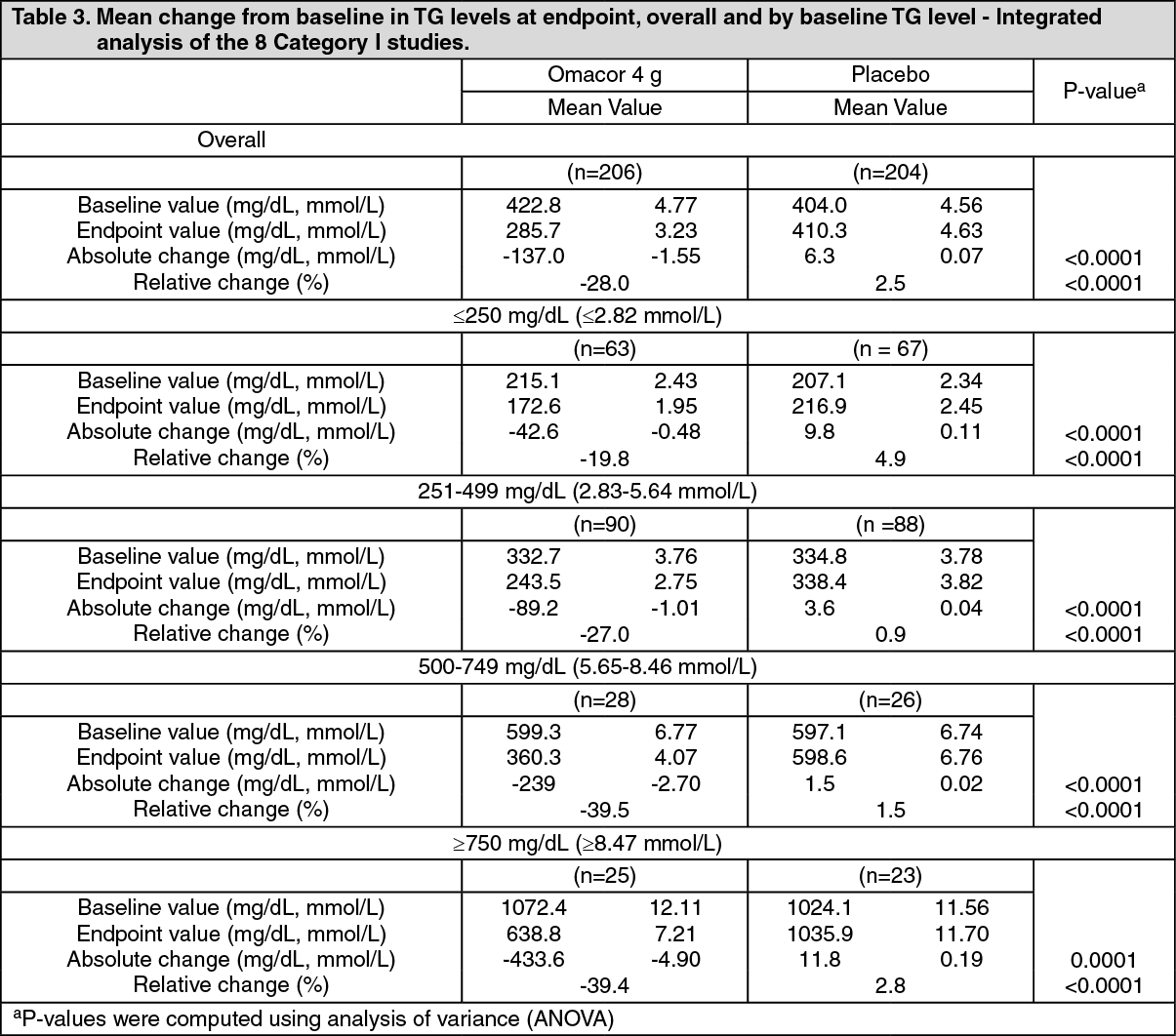
The cholesterol enrichment of LDL particles appears to happen in conjunction with a marked reduction in VLDL-C. Studies also demonstrate a shift from small, dense LDL particles to larger, more buoyant LDL particles, indicating a shift towards less atherogenic lipoprotein particles. Consistent with the overall population (see Table 3 hereafter), subjects in each baseline triglycerides level category in the Omacor 4 g treatment group had significantly larger mean absolute and relative changes in triglycerides levels compared with those in the placebo treatment group.
For the subjects who received Omacor 4 g per day, those with higher baseline levels (TG=500-749 mg/dL and ≥750 mg/dL [5.65-8.46 mmol/L, and ≥8.47 mmol/L])) had greater reductions in triglycerides levels, and therefore were more likely to exhibit a better response to Omacor. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageA number of studies have been conducted to evaluate the effect of concomitant use of Omacor with widely used statins (simvastatin, atorvastatin). The studies have been carried out in patients with elevated serum triglycerides receiving statin therapy. The results of the studies demonstrate that the combined treatment increases the efficacy in lowering triglycerides. In these studies, little or no effect on LDL-C has been observed and no significant safety issues have been raised.
Pharmacokinetics: During and after absorption, there are three main pathways for the metabolism of the omega-3 fatty acids: the fatty acids are first transported to the liver where they are incorporated into various categories of lipoproteins and then channelled to the peripheral lipid stores; the cell membrane phospholipids are replaced by lipoprotein phospholipids and the fatty acids can then act as precursors for various eicosanoids; the majority is oxidised to meet energy requirements.
The concentration of omega-3 fatty acids, EPA and DHA, in the plasma phospholipids corresponds to the EPA and DHA incorporated into the cell membranes.
Animal pharmacokinetic studies have shown that there is a complete hydrolysis of the ethyl ester accompanied by satisfactory absorption and incorporation of EPA and DHA into the plasma phospholipids and cholesterol esters.
Toxicology: Preclinical safety data: No safety issues have been identified relevant to human use at the recommended daily intake. Non-clinical data reveal no special hazard for humans based on conventional studies of repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction. In addition non-clinical literature data on safety pharmacology indicate that there is no hazard to humans.