Turbuhaler: 1 metered dose contains budesonide 100 micrograms or 200 micrograms.
Respules: PULMICORT RESPULES contain budesonide 0.5 mg/2 mL or 1.0 mg/2 mL as the active ingredient.
The active ingredient, budesonide, is a non-halogenated glucocorticoid structurally related to 16α hydroxyprednisolone. The chemical name is 16α, 17α-22R, S-propylmethylenedioxy-pregna-1, 4-diene-11β, 21-diol-3, 20-dione; MW 430.5.
CAS Number: 51333-22-3.
Budesonide is a white to off-white powder, freely soluble in chloroform, sparingly soluble in ethanol and practically insoluble in water and heptane. Budesonide melts with decomposition between 224°C and 231.5°C.
Excipients/Inactive Ingredients: Turbuhaler: Pulmicort Turbuhaler contains no excipients.
Respules: disodium edetate, sodium chloride, polysorbate 80 (E 433) citric acid - anhydrous (E 330), sodium citrate (E 331) and water for injections.
Pharmacotherapeutic group: Turbuhaler: Inhalation drugs for obstructive airway diseases. ATC code: Turbuhaler: R03BA02.
Pharmacology: Pharmacodynamics: Turbuhaler: Budesonide is a glucocorticosteroid with a high local anti-inflammatory effect.
The precise mechanism of action of glucocorticosteroids in the treatment of asthma is not fully understood. Anti-inflammatory effects such as inhibited release of inflammatory mediators and inhibition of cytokine-mediated immune response are probably important. The activity of budesonide, measured as its affinity for glucocorticosteroid receptors is approx. 15 times higher than that of prednisolone.
Budesonide has anti-inflammatory effects shown as reduced bronchial obstruction during both the early and the late phase of an allergic reaction. Budesonide has been shown to decrease airway reactivity to histamine and methacholine in hyper-reactive patients.
Studies have shown that the earlier budesonide treatment is initiated after the onset of asthma, the better lung function can be expected.
Studies in healthy volunteers with Pulmicort Turbuhaler have shown dose-related effects on plasma and urinary cortisol. At recommended doses, Pulmicort Turbuhaler, causes significantly less effect on the adrenal function than prednisone 10 mg, as shown by ACTH tests.
In children over the age of 3 years, no systemic effects have been detected with doses up to 400 micrograms per day. In the range 400-800 micrograms per day biochemical signs of a systemic effect may occur. With daily doses in excess of 800 micrograms such signs are common.
Asthma, like inhaled corticosteroids, can delay growth. An initial small but generally transient reduction in growth (approximately 1 cm) has been observed, which usually occurs within the first year of treatment. Long-term studies in a clinical practice environment suggest that children and adolescents treated with inhaled budesonide on average achieve their adult target height. However, in a long-term double-blind study, in which the budesonide dose was generally not titrated to the lowest effective dose, children and adolescents treated with inhaled budesonide became on average 1.2 cm shorter as adults than those randomised to placebo. See Precautions about titration to the lowest effective dose and about monitoring the growth in children.
Inhalation therapy with budesonide is effective in preventing exercise-induced asthma.
Respules: PULMICORT is a corticosteroid for inhalation use in the treatment and prophylaxis of asthma.
Studies in animals and humans have shown an advantageous ratio between topical anti-inflammatory activity and systemic glucocorticoid effect over a wide dose range. This is explained by the extensive first pass hepatic degradation of budesonide after systemic absorption, approximately 85-90%, in combination with the low potency of formed metabolites.
Budesonide is approximately twice as potent as beclomethasone dipropionate as shown in the skin blanching test for anti-inflammatory activity of topical steroids in humans. Budesonide has, however, less systemic effect than beclomethasone dipropionate, as measured by depression of morning plasma cortisol and effect on differential WBC count. The improved ratio of topical anti-inflammatory activity to systemic effect of budesonide is due to high glucocorticoid receptor affinity combined with a high first pass metabolism and a short half-life.
Doses of 0.8 mg have been found to suppress plasma cortisol levels and urinary cortisol secretion. A single inhalation of 3.2 mg budesonide was found to suppress plasma cortisol levels to a degree similar to 10 mg oral prednisolone.
Budesonide has been shown to counteract the mainly "IgE" but not the mainly "IgG" mediated lung anaphylaxis in guinea pigs. Pre-treatment for one to four weeks with inhaled budesonide 1 mg daily in asthmatic patients inhibited the immediate bronchial reaction to allergen challenge in a time-related manner; the late reaction is inhibited after one week of inhaled treatment.
Inhaled budesonide pre-treatment for 2 to 4 weeks has also been shown to reduce non-specific bronchial hyper-responsiveness in asthmatic patients to both direct (histamine, methacholine) and indirect (exercise) provocative stimuli in a time-related manner.
Budesonide did not potentiate β-receptor-mediated bronchodilation, and did not affect theophylline-induced relaxation of respiratory airway smooth muscle in guinea pigs. In man, single oral inhalations of up to 1.6 mg budesonide produced mild bronchodilation. This effect is maximal at 6 hours after inhalation with a duration of 12 hours.
Pharmacokinetics: Turbuhaler: Absorption: Inhaled budesonide is rapidly absorbed. The peak plasma concentration is reached within 30 minutes after inhalation. In studies, the average deposition of budesonide in the lungs after inhalation via Turbuhaler has been shown to be 25-35% of the metered dose. The systemic bioavailability is approx. 38% of the metered dose.
Distribution and metabolism: Plasma protein binding is approx. 90%. The volume of distribution is approx. 3 l/kg. Budesonide undergoes extensive (approx. 90%) first pass metabolism in the liver to metabolites with low glucocorticosteroid activity. The glucocorticosteroid activity of the major metabolites, 6β-hydroxybudesonide and 16α-hydroxyprednisolone, is less than 1% of that of budesonide.
Elimination: Budesonide is eliminated through metabolism, catalysed primarily by the enzyme CYP3A4. The metabolites are excreted in the urine in unchanged or conjugated form. Only negligible amounts of unchanged budesonide are recovered in the urine. Budesonide has a high systemic clearance (approx. 1.2 l/min), and the plasma half-life after intravenous administration is on average 4 hours. The pharmacokinetics of budesonide is proportional to the dose at relevant dosages.
The pharmacokinetics of budesonide in children and in patients with impaired renal function is unknown. Exposure to budesonide may be increased in patients with hepatic disease.
Respules: Approximately 10% of the discharged dose of PULMICORT aerosol is deposited in the lungs.
The volume of distribution of budesonide in adult man is approximately 300 L and in children is 3.1 to 4.8 L/kg indicating a high tissue affinity. Plasma protein binding is 88.3±1.5% in humans.
In adults the plasma half-life following inhalation via aerosol was 2.0±0.2 hours and in children 1.5 hour with peak plasma levels occurring immediately after administration.
Negligible biotransformation was observed in human lung and serum preparations.
PULMICORT is 90% inactivated on first pass through the liver, via metabolism to more polar metabolites with a more than 100-fold lower glucocorticosteroid systemic activity than the parent compound.
In human volunteers who inhaled tritiated budesonide, 31.8±7.5% of the discharged dose was recovered in urine and 15.1±4.3% in faeces (0-96 h). Plasma clearance of unchanged budesonide was calculated to be 84 L/h in adults and 1.5 to 2 L/h/kg in children.
Toxicology: Preclinical safety data: Turbuhaler: In toxicity studies budesonide caused only the expected glucocorticoid effects.
Budesonide has not exhibited any genotoxic effects.
In animal reproduction studies, corticosteroids such as budesonide have been shown to induce malformations (cleft palate, skeletal malformations). However, these animal experimental results do not seem to be relevant in humans at the recommended doses.
Turbuhaler: Pulmicort Turbuhaler is indicated for patients with bronchial asthma who require maintenance treatment with glucocorticosteroids for control of the underlying airways inflammation.
Respules: Treatment of bronchial asthma.
PULMICORT may also be used when replacement or reduction in oral steroid therapy is desirable.
PULMICORT RESPULES provide budesonide in a nebulising suspension which is recommended when other modes of steroid therapy are unsuitable.
Turbuhaler: The dosage of Pulmicort Turbuhaler is individual.
Initially, at the beginning of inhaled corticosteroid therapy, for therapy during periods of severe asthma or when scaling down or withdrawing oral corticosteroids the dosage should be: Children 5-7 years: 200-400 micrograms daily divided into 2-4 administrations.
Children 7 years and more: 200-800 micrograms daily divided into 2-4 administrations.
Adults: 200-1600 micrograms daily divided into 2-4 administrations, (less severe cases 200-800 micrograms daily, more severe cases 800-1600 micrograms daily).
Administration twice daily (morning and evening) is usually sufficient.
The maintenance dose is individual and should be the lowest possible. When the maintenance dose is 400 micrograms or lower the dose can be given once daily. The dose may then be given in the morning or in the evening. If deterioration of asthma occurs, the frequency of dosing and the daily dose should be increased.
Following a single dose an effect may be expected after a few hours. The full therapeutic effect is only achieved after a few weeks of treatment. Treatment with Pulmicort Turbuhaler is prophylactic therapy with no demonstrated effect on acute disorders.
Clinical trials indicate that a larger amount of budesonide is deposited in the lungs when administered with Pulmicort Turbuhaler, compared with Pulmicort pMDI. If a patient in a stable phase is transferred from Pulmicort pMDI to Pulmicort Turbuhaler a reduction in dose may therefore be appropriate.
In patients in whom an increased therapeutic effect is desired, in general an increase of the Pulmicort Turbuhaler dose is to be recommended in preference to combination treatment with oral corticosteroids on account of the lower risk of systemic side effects.
Patients dependent on oral steroids: When transfer from oral steroids to Pulmicort Turbuhaler is initiated the patient must be in a relatively stable condition. For 10 days, a high dose of Pulmicort Turbuhaler is given in combination with the previously used oral steroid. After that, the oral dose should be gradually reduced by e.g. 2.5 mg prednisolone or equivalent per month to the lowest possible level. The oral steroid can often be discontinued entirely.
There is no experience of treatment of patients with impaired hepatic or renal function. Since budesonide is predominantly eliminated through hepatic metabolism, increased exposure may be expected in patients with severe cirrhosis of the liver.
Instructions for correct use of Turbuhaler: It is important that the inhaler is used correctly.
Turbuhaler is inspiratory flow-driven which means that, when the patient inhales through the mouthpiece, the substance will follow the inspired air into the airways.
Note: It is important to instruct the patient: To carefully read the instructions for use: "How to use Pulmicort Turbuhaler" under Cautions for Usage.
To breathe in forcefully and deeply through the mouthpiece to ensure that an optimal dose is delivered to the lungs.
Never to breathe out through the mouthpiece.
To rinse the mouth out with water after inhaling the prescribed dose to minimise the risk of oropharyngeal thrush.
The patient may not taste or feel any medication when using Pulmicort Turbuhaler due to the small amount of drug dispensed.
Respules: Bronchial asthma: PULMICORT RESPULES Nebulising Suspension: PULMICORT RESPULES should be administered from a suitable nebuliser. The dose delivered to the patient varies between 40-60% of the nominal dose depending on the nebulising equipment used. The nebulisation time and the dose delivered is dependent on flow rate, volume of nebuliser chamber and volume fill. A suitable fill for most nebulisers is 2-4 mL.
Some sedimentation may occur during storage of PULMICORT RESPULES. If this does not readily resuspend completely upon shaking, the RESPULE should be discarded.
Dosage initially, or during periods of severe asthma, or while reducing oral corticosteroids: Adults: 1-2 mg twice daily.
Children: 0.5-1 mg twice daily.
Maintenance: The maintenance dose should be individualised and should be the lowest dose, which keeps the patient symptom-free. Recommended doses are: Adults: 0.5-1 mg twice daily.
Children: 0.25-0.5 mg twice daily.
Patient Instructions: 1. It is essential that the patient be instructed that PULMICORT is a preventative agent, which must be taken regularly and is not to be used as sole therapy to relieve an acute asthma attack.
2. The patient should be instructed in the proper use of the inhaler device considered appropriate for his/her particular needs. A full set of instructions are provided with each pack of PULMICORT.
3. Patients also receiving bronchodilators by inhalation should be advised to use the bronchodilator before PULMICORT in order to enhance its penetration into the bronchial tree. Several minutes should elapse between the use of the two inhalers.
Clinical Management: Patients - not oral corticosteroid dependent: Treatment with the recommended doses of PULMICORT usually gives a therapeutic effect within 10 days.
In patients with excessive mucus secretion in the bronchi, an initial short course (about 2 weeks) of an oral corticosteroid, commencing with a high dose and gradually reducing, should be given in addition to PULMICORT. Treatment should be continued for at least one month before determining the maximal response to a given dose of PULMICORT.
Patients - oral corticosteroid dependent: Transfer of patients dependent on oral corticosteroids to PULMICORT requires special care because of slow normalisation of the disturbed hypothalamic-pituitary-adrenal function caused by extended treatment with oral corticosteroids (see Oral corticosteroid usage and Potential systemic effects of inhaled corticosteroids: HPA axis suppression and adrenal insufficiency under Precautions).
When PULMICORT treatment is initiated, the patient's asthma should be in a relatively stable phase. A high dose of PULMICORT should then be given in combination with the previously used oral corticosteroid dose for about 2 weeks. The dose of oral corticosteroid should then be reduced gradually (for example 1mg prednisolone or equivalent every four days, however, the exact rate of reduction will depend on individual clinical response) to the lowest possible level. The dose of PULMICORT should not be changed while the patient remains on oral corticosteroids.
In many cases, it may be possible to completely replace the oral corticosteroid with inhaled PULMICORT. In other patients, a low oral steroid maintenance dose may be necessary. Some patients may experience uneasiness during the withdrawal of oral corticosteroids due to the decreased systemic corticosteroid effect. The physician may need to actively support the patient and to stress the reason for the PULMICORT treatment.
The length of time needed for the body to regain sufficient natural corticosteroid production is often extended and may be as long as 12 months. Transferred patients should carry a warning card indicating that they may need supplementary systemic corticosteroids during periods of stress, such as severe infection, trauma or surgery. During such times it may be necessary to give additional oral corticosteroids.
During transfer from oral therapy to PULMICORT, a lower systemic steroid action is experienced. Earlier allergic symptoms may recur (eg. rhinitis, eczema, conjunctivitis) or patients may suffer from tiredness, headache, muscle and joint pain, lassitude and depression or occasionally nausea and vomiting. In these cases, further medical support may be required.
Turbuhaler: Acute overdose with Pulmicort Turbuhaler, even in high doses, is not expected to cause any clinical problems. If used chronically in high doses, systemic effects of glucocorticosteroids such as hypercortisolism and adrenal suppression can occur.
Respules: Symptoms: In most cases, occasional overdosing will not produce any obvious symptoms but will decrease the plasma cortisol level and increase the number and percentage of circulating neutrophils. The number and percentage of lymphocytes and eosinophils will decrease concurrently. Habitual overdosing may cause hypercorticism and hypothalamic-pituitary-adrenal suppression.
Treatment: Withdrawing PULMICORT or decreasing the dose will abolish these effects, although the normalization of the HPA-axis may be a slow process.
Hypersensitivity to budesonide or any other ingredients.
Turbuhaler: Special care is needed in patients with lung tuberculosis and fungal and viral infections. Children who are on immunosuppressant drugs are more susceptible to infections than healthy children. Chicken pox and measles, for example, can have a more serious or fatal course in children on immunosuppressant corticosteroids. In such children, or in adults who have not had these diseases, particular care should be taken to avoid exposure. If exposed, therapy with varicella zoster immune globulin (VZIG) or pooled intravenous immunoglobulin (IVIG), as appropriate, may be indicated. If chicken pox develops, treatment with antiviral agents may be considered. If, however, a viral upper respiratory infection is present, the patient should adhere to the regular asthma medication. In patients who are known to deteriorate rapidly when they have a viral respiratory infection, a short course of oral corticosteroid therapy should be considered.
Clinical studies have shown that viral infections cause significantly less problems in patients who are on regular treatment with topical glucocorticosteroids.
In order to minimise the risk of Candida infections in the oral cavity and throat, the patient should be instructed to rinse the mouth with water after each dose administration.
Concomitant treatment with ketoconazole, itraconazole or other potent CYP3A4 inhibitors should be avoided. If this is not possible, the interval between the administrations of the drugs should be as long as possible (see Interactions).
Particular care is needed in patients transferring from oral glucocorticosteroids, since they may remain at risk of impaired adrenal function for a considerable time. Patients, who have required high dose emergency glucocorticosteroid therapy or prolonged treatment at the highest recommended dose of inhaled glucocorticosteroids, may also be at risk. These patients may exhibit signs and symptoms of adrenal insufficiency when exposed to severe stress. Additional systemic glucocorticosteroid cover should be considered during periods of stress or elective surgery.
During the transfer from oral steroid therapy to Pulmicort Turbuhaler, patients may experience the return of previous symptoms such as muscle and joint pain. In these cases a temporary increase of the oral steroid dose may sometimes be necessary. If, in isolated cases, fatigue, headache, nausea, vomiting or similar symptoms occur, a generally unsatisfactory effect of the steroid should be suspected.
Replacement of systemic steroid treatment by Pulmicort Turbuhaler sometimes reveals allergies, e.g. rhinitis and eczema that were previously controlled by the systemic treatment.
Regular monitoring of growth is recommended in children and adolescents receiving long-term treatment with corticosteroids, irrespective of the administration form. The benefits of corticosteroid treatment must be placed in relation to possible risks of inhibition of growth. If growth is slowed, therapy should be reviewed with the aim of reducing the dose of inhaled corticosteroid, if possible, to the lowest dose at which effective control of asthma is maintained. In addition, consideration should be given to referring the patient to a paediatric respiratory specialist.
Pulmicort is not indicated for rapid relief of bronchospasm. Pulmicort is therefore not suitable as sole therapy for the treatment of status asthmaticus or other acute exacerbations of asthma where intensive measures are required.
If patients find short-acting bronchodilator treatment ineffective, or they need more inhalations than usual, medical attention must be sought. This indicates a worsening of the underlying conditions and warrants a reassessment of the therapy.
Acute exacerbations of asthma may need complementary treatment with a short oral steroid regimen.
Decreased liver function may affect the ability to eliminate budesonide.
Visual disturbance may be reported with systemic and topical corticosteroid use. If a patient presents with symptoms such as blurred vision or other visual disturbances, the patient should be considered for referral to an ophthalmologist for evaluation of possible causes which may include cataract, glaucoma or rare diseases such as central serous chorioretinopathy (CSCR) which have been reported after use of systemic and topical corticosteroids.
Respules: Bronchospasm: PULMICORT is not indicated for rapid relief of bronchospasm. PULMICORT is therefore not suitable as sole therapy for the treatment of status asthmaticus or other acute exacerbations of asthma where intensive measures are required.
If patients find short-acting bronchodilator treatment ineffective, or they need more inhalations than usual, medical attention must be sought. This indicates a worsening of the underlying conditions, and warrants a reassessment of the therapy.
Oral corticosteroid usage: Particular care is needed in patients who are being transferred from oral corticosteroids to PULMICORT, since they may remain at risk of impaired adrenal function for some considerable time (see Potential systemic effect of inhaled corticosteroids: HPA axis suppression and adrenal insufficiency as follows). These patients should be instructed to carry an appropriate warning card (see Clinical Management: Patients - oral corticosteroid dependent under Dosage & Administration).
Patients previously receiving high doses of systemic steroids may regain earlier allergic symptoms such as rhinitis and eczema when transferred from oral therapy to PULMICORT due to the reduced systemic steroid effect of budesonide (see Clinical Management: Patients - oral corticosteroid dependent under Dosage & Administration).
Potential systemic effects of inhaled corticosteroids: Inhaled steroids are designed to direct glucocorticoid delivery to the lungs in order to reduce overall systemic glucocorticoid exposure and side effects. However inhaled steroids may have adverse effects; possible systemic effects of inhaled steroids include depression of the HPA axis, reduction of bone density, cataracts and glaucoma and retardation of growth rate in children. In steroid-dependent patients, prior systemic steroid usage may be a contributing factor (see Oral corticosteroid usage as previously mentioned), but such effects may occur amongst patients who use only inhaled steroids regularly.
HPA axis suppression and adrenal insufficiency: Dose-dependent HPA axis suppression (as indicated by 24 hour urinary and/or plasma cortisol AUC) has been observed with inhaled budesonide, although the physiological circadian rhythms of plasma cortisol were preserved. This indicates that the HPA axis suppression may represent a physiological adaption in response to inhaled budesonide, not necessarily adrenal insufficiency. The lowest dose that results in clinically relevant adrenal insufficiency has not been established. Very rare cases of clinically relevant adrenal dysfunction have been reported in patients using inhaled budesonide at recommended doses.
Particular care is needed in patients who are being transferred from oral corticosteroids to PULMICORT, since they may remain at risk of impaired adrenal function for some considerable time (see Oral corticosteroid usage as previously mentioned). Patients who have required high dose emergency corticosteroid therapy, prolonged treatment at the highest recommended dose of inhaled corticosteroids or patients administering concomitant medication metabolised by CYP3A4 (see Interactions) may also be at risk. These patients may exhibit signs and symptoms of adrenal insufficiency when exposed to severe stress such as trauma, surgery, infection (particularly gastroenteritis) or other conditions associated with severe electrolyte loss. Monitoring for signs of adrenal dysfunction is advisable in these patient groups. For these patients additional systemic glucocorticosteroid cover should be considered during periods of stress, severe asthma attack or elective surgery.
Bone density: Whilst corticosteroids may have an effect on bone mass at high doses, long term follow up (3-6 years) studies of budesonide treatment in adults at recommended doses, have not demonstrated a negative effect on bone mass compared to placebo, including one study conducted in patients with a high risk of osteoporosis. The lowest dose that does effect bone mass has not been established.
Bone mineral density measurements in children should be interpreted with caution as an increase in bone area in growing children may reflect an increase in bone volume. In three large medium to long term (12 months - 6 years) studies in children (5-16 years), no effects on bone mineral density were observed after treatment with Pulmicort (189-1322 μg/day) compared to nedocromil, placebo or age matched controls. However, in a randomised 18 month study (n=176; 5-10 years), bone mineral density was significantly decreased by 0.11 g/cm2 (p=0.023) in the group treated with inhaled budesonide via Turbuhaler compared with the group treated with inhaled disodium cromoglycate. The dose of budesonide was 400 μg twice daily for 1 month, 200 μg twice daily for 5 months and 100 μg twice daily for 12 months and the dose of disodium cromoglycate 10 mg three times daily. The clinical significance of this result remains uncertain.
Growth: Long term studies show that children treated with inhaled budesonide ultimately achieve adult target height. However, an initial reduction of growth velocity (approximately 1 cm) has been observed and is generally within the first year of treatment.
Rare individuals may be exceptionally sensitive to inhaled corticosteroids. Height measurements should be performed to identify patients with increased sensitivity. The potential growth effects of prolonged treatment should be weighed against the clinical benefit. To minimise the systemic effects of inhaled corticosteroids, each patient should be titrated to his/her lowest effective dose (see Dosage & Administration).
Visual disturbance: Visual disturbance may be reported with systemic and topical corticosteroid use. If a patient presents with symptoms such as blurred vision or other visual disturbances, the patient should be considered for referral to an ophthalmologist for evaluation of possible causes which may include cataract, glaucoma or rare diseases such as central serous chorioretinopathy (CSCR) which have been reported after use of systemic and topical corticosteroids.
Infections and tuberculosis: High doses of glucocorticosteroids may mask some signs of existing infection and new infections may appear during their use. Special care is needed in patients with active or quiescent pulmonary tuberculosis or fungal, bacterial or viral infections of the respiratory system.
Hepatic function: Reduced liver function may affect the elimination of corticosteroids. This may be clinically relevant in patients with severely compromised liver function.
Positive pressure delivery systems: Respiratory drugs should not be used with positive pressure delivery systems (eg. IPPB) in pulmonary conditions involving pneumothorax, air cysts or mediastinal emphysema unless special drainage is performed.
Carcinogenicity and mutagenicity: The carcinogenic potential of budesonide has been evaluated in mouse and rat at oral doses up to 200 and 50 μg/kg/day, respectively. No oncogenic effect was noted in the mouse. One study indicated an increased incidence of brain gliomas in male Sprague-Dawley rats given budesonide, however the results were considered equivocal. Further studies performed in male Sprague-Dawley and Fischer rats showed that the incidence of gliomas in the budesonide-treated rats was low and did not differ from that in the reference glucocorticoid groups or the controls. It has been concluded that treatment with budesonide does not increase the incidence of brain tumours in the rat.
In male rats dosed with 10, 25 and 50 μg/kg/day, those receiving 25 and 50 μg/kg/day showed an increased incidence of primary hepatocellular tumours. This was observed in all three steroid groups (budesonide, prednisolone, triamcinolone acetonide) in a repeat study in male Sprague-Dawley rats thus indicating a class effect of corticosteroids.
The mutagenic potential of budesonide was evaluated in 6 different test systems. No mutagenic or clastogenic effects of budesonide were found.
Effects on ability to drive and use machines: Turbuhaler: Pulmicort Turbuhaler does not affect ability to drive or use machines.
Turbuhaler: Pregnancy: Data from approximately 2000 pregnancies have not revealed any increased risk of malformations as a result of treatment with budesonide. Animal studies have shown that glucocorticosteroids can induce malformations, but this is judged not to be relevant for humans with the recommended dosage.
Animal studies have also identified an involvement of excess prenatal glucocorticoids in increased risks for intrauterine growth retardation, adult cardiovascular disease and permanent changes in glucocorticoid receptor density, neurotransmitter turnover and behaviour at exposures below the teratogenic dose range.
During pregnancy the aim must be the lowest effective dose of budesonide while taking account of the risk of a worsening of the asthma.
Lactation: Budesonide is excreted in breast milk. However, at therapeutic doses of Pulmicort Turbuhaler no effects on the suckling child are anticipated. Pulmicort Turbuhaler can be used during breastfeeding.
Respules: Use in pregnancy - Category A*: The benefits of asthma control outweigh any potential for an adverse pregnancy outcome.
Results from a large prospective epidemiological study and from world-wide post marketing experience indicate that inhaled budesonide during pregnancy has no adverse effects on the health of the foetus or new born child.
Inhaled glucocorticosteroids, such as budesonide, should be considered because of the lower systemic effects of doses, compared to those of oral glucocorticosteroids, required to achieve similar pulmonary responses.
*Category A: Drugs which have been taken by a large number of pregnant women and women of childbearing age without any proven increase in the frequency of malformations or other direct or indirect harmful effects on the foetus having been observed.
Use in lactation: Budesonide is excreted in breast milk. However, due to the relatively low doses used via the inhalational route the amount of drug present in the breast milk, if any, is likely to be low. Breastfeeding can be considered if the potential benefit outweighs any potential risks.
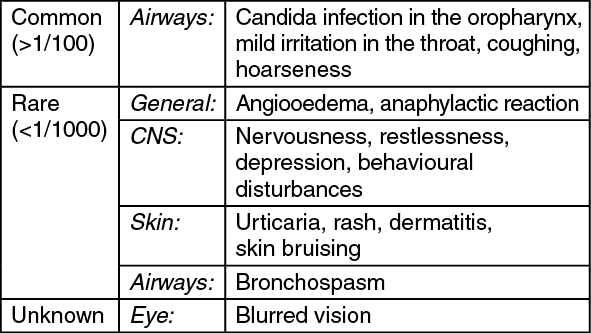
Turbuhaler: Up to 10% of patients treated may be expected to experience adverse reactions of a local nature. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
On account of the risk of Candida infections in the oropharynx the patient must rinse the mouth with water after every dose.
In rare cases signs or symptoms of systemic glucocorticosteroid effect, including hypofunction of the adrenal gland and reduction of growth velocity, may occur with inhaled glucocorticosteroids, probably depending on dose, exposure time, concomitant and previous steroid exposure, and individual sensitivity.
Respules: PULMICORT is generally well tolerated. Most adverse reactions have been mild and of a local character. Systemic effects and oropharyngeal complications caused by budesonide were found to be dose-dependent.
Clinical signs of steroid excess were present in 50% of patients (n=10) taking 1.6mg or more daily of budesonide alone for long periods.
Clinical trials, literature reports and post-marketing experience suggest that the following adverse drug reactions may occur:
Common (more than 1%): Nose and throat: hoarseness; sore, irritated throat; irritation of the tongue and mouth; dry mouth; oral candidasis.
Respiratory: cough.
Uncommon (less than 1%): Nose and throat: irritation of the larynx; bad taste.
Gastrointestinal: diarrhoea; nausea.
Hypersensitivity reactions: immediate and delayed hypersensitivity reactions such as skin reactions (eg. urticaria, rash, dermatitis), bronchospasm, angioedema and anaphylactic reaction.
Central nervous system: headache; lightheadedness; thirst; tiredness.
Metabolic and nutritional disorders: weight gain.
Unknown: Eye disorders: blurred vision.
If oropharyngeal candidiasis develops, it may be treated with appropriate anti-fungal therapy whilst still continuing with PULMICORT therapy. The incidence of candidiasis can generally be held to a minimum by having patients rinse their mouth with water after each inhalation.
Inhaled steroids may have adverse effects in higher than recommended doses; possible systemic effects of inhaled steroids include depression of the HPA axis, reduction of bone density and retardation of growth rate in children (see Potential systemic effects of inhaled corticosteroids under Precautions).
Reduction in growth velocity has been reported in association with administration of inhaled corticosteroids, however studies with budesonide indicate that this is transient and that final adult height may ultimately be achieved (see Growth under Precautions).
Dose-dependent HPA axis suppression has been observed with budesonide, however this may represent a physiological adaption rather than adrenal insufficiency (see HPA axis suppression and adrenal insufficiency under Precautions). The lowest dose that results in clinically relevant adrenal insufficiency has not been established.
No negative effects on bone mass have been observed in adults treated with inhaled budesonide at recommended doses. In children, bone mineral density should be interpreted with caution as an increase in bone area may reflect an increase in bone volume (see Bone density under Precautions).
Rare reports of skin bruising have occurred following treatment with inhaled glucocorticosteroids.
Psychiatric symptoms such as behavioural disturbances, nervousness, restlessness and depression have been observed with budesonide as well as other glucocorticosteroids.
Facial skin irritation has occurred in a few cases when a nebuliser with a face mask has been used. To prevent irritation the face should be washed after each use of PULMICORT RESPULES delivered via a nebuliser with a face mask.
Rarely, PULMICORT may provoke bronchoconstriction in hyperreactive patients. Bronchospasm may be treated with an inhaled β
2-agonist.
Turbuhaler: No clinically relevant interactions with other agents for asthma are known.
Ketoconazole 200 mg once daily increased the plasma concentrations of oral budesonide (3 mg in a single dose) on average six-fold when administered concomitantly. When ketoconazole was administered 12 hours after budesonide, the concentration was increased on average three-fold. Information about this interaction is lacking for inhaled budesonide, but markedly increased plasma levels are also expected in such cases. Since there is an absence of data to permit dosage recommendations, the combination should be avoided.
If this is not possible, the time interval between administration of ketoconazole and budesonide should be as long as possible. A reduction of the budesonide dose must also be considered. Other potent inhibitors of CYP3A4, i.e. itraconazole also cause a marked increase in the plasma levels of budesonide.
Respules: The metabolism of budesonide is primarily mediated by CYP3A, a subfamily of cytochrome P450. Inhibitors of this enzyme e.g. ketoconazole and itraconazole, can therefore increase systemic exposure to budesonide. This is of limited clinical importance for short-term (1-2 weeks) treatment with CYP3A inhibitors, but should be taken into consideration during long-term treatment.
Incompatibilities: Turbuhaler: Not relevant.
INSTRUCTIONS FOR USE/HANDLING: Turbuhaler: Read the complete instructions carefully before starting to take the medication.
Turbuhaler is a multidose inhaler from which very small amounts of powder are administered. When breathing in through Turbuhaler the powder is delivered to the lungs. It is therefore important that the patient inhales forcefully and deeply through the mouthpiece.
How to prepare a new inhaler for use: Before using Turbuhaler for the first time the patient needs to prepare the inhaler for use.
Unscrew and lift off the cover.
Hold the inhaler upright with the grip downwards. Do not hold the mouthpiece when turning the grip. Turn the grip as far as it will go in one direction, and then back again in the opposite direction as far as it will go. It does not matter which way the patient turns first. During this procedure the patient will hear a click. Perform the procedure twice.
The inhaler is now prepared for use, and the patient should not repeat the previously mentioned procedure again. To take a dose, continue according to the instructions as follows.
HOW TO USE PULMICORT TURBUHALER: To administer one dose, simply follow the instructions as follows: 1. Unscrew and lift off the cover.
2. Hold the inhaler upright with the grip downwards. Do not hold the mouthpiece when turning the grip. To load the inhaler with a dose, turn the grip as far as it will go in one direction, and then back again in the opposite direction as far as it will go. It does not matter which way the patient turns first. During this procedure the patient will hear a click.
3. Hold the inhaler away from the mouth. Breathe out. Do not breathe out through the mouthpiece.
4. Place the mouthpiece gently between the teeth, close the lips and inhale forcefully and deeply through the device. Do not chew or bite on the mouthpiece. Do not use Turbuhaler if it has been damaged or if the mouthpiece has become detached.
5. Remove the inhaler from the mouth before breathing out.
If more than one dose has been prescribed, repeat steps 2-5.
6. Replace the cover by screwing it back on tightly.
7. Rinse the mouth out with water after inhaling the prescribed dose.
NOTE: Never breathe out through the mouthpiece.
Always replace the cover properly after use.
As the amount of the powder dispensed is very small, the patient may not be able to taste it after inhalation. However, the patient can still be confident that the dose has been inhaled if the patient has followed the instructions.
Cleaning: Clean the outside of the mouthpiece regularly (weekly) with a dry tissue.
Do not use water for cleaning the mouthpiece.
Dose indicator: When a red mark is first seen in the indicator window there are approximately 20 doses left. When the red mark has reached the lower edge of the window the inhaler will no longer deliver the correct amount of medicine, and should be discarded. The sound heard as the patient shakes the inhaler is not produced by the medication but by a drying agent.
Disposal: Always be sure to dispose of the used Turbuhaler responsibly in the recommended way, since some of the medicine will remain inside it. Ask the pharmacist for advice.
Shelf-life: Respules: Unused Respules should be discarded three months after opening of foil packs.
Opened single dose units should be used within 12 hours. Note that if only 1 mL is used the remaining volume is not sterile.
Turbuhaler: Do not store above 30°C.
Must be stored with the protective cap in place.
Respules: Store in an upright position and protected from light. Stored below 30°C. Do not refrigerate.
R03BA02 - budesonide ; Belongs to the class of other inhalants used in the treatment of obstructive airway diseases, glucocorticoids.
Pulmicort respules 0.25 mg/mL
30 × 1's
Pulmicort respules 0.5 mg/mL
30 × 1's
Pulmicort turbuhaler 100 mcg/dose
1's
Pulmicort turbuhaler 200 mcg/dose
1's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
