Pharmacotherapeutic group: DPP-4 inhibitor.
ATC code: A10BH05.
Pharmacology: Linagliptin is an inhibitor of the enzyme DPP-4 (Dipeptidyl peptidase 4, EC 3.4.14.5) an enzyme which is involved in the inactivation of the incretin hormones GLP-1 and GIP (glucagon-like peptide-1, glucose-dependent insulinotropic polypeptide). These hormones are rapidly degraded by the enzyme DPP-4. Both incretin hormones are involved in the physiological regulation of glucose homeostasis. Incretins are secreted at a low basal level throughout the day and levels rise immediately after meal intake. GLP-1 and GIP increase insulin biosynthesis and secretion from pancreatic beta cells in the presence of normal and elevated blood glucose levels. Furthermore GLP-1 also reduces glucagon secretion from pancreatic alpha cells, resulting in a reduction in hepatic glucose output. Linagliptin binding to DPP-4 is reversible but long-lasting and thus leads to a sustained increase and a prolongation of active incretin levels.
In vitro, linagliptin inhibits DPP-4 with nanomolar potency and exhibits a >10000 fold selectivity versus DPP-8 or DPP-9 activity.
Pharmacodynamics: Clinical trials: Linagliptin monotherapy: The efficacy and safety of linagliptin monotherapy was evaluated in a double blind placebo controlled study of 24 weeks duration. Treatment with once daily linagliptin at 5 mg provided a significant improvement in HbA1c (-0.69 % change compared to placebo), in patients with baseline HbA1c of approximately 8 %. Linagliptin also showed significant improvements in fasting plasma glucose (FPG) 2-hour post-prandial glucose (PPG), and a greater portion of patients achieved a target HbA1c of < 7.0%, compared to placebo.
The improvement in HbA1c was not affected by gender, age, race, baseline BMI, presence of metabolic syndrome, or a standard index of insulin resistance (HOMA-IR). Treatment with linagliptin 5 mg daily significantly improved surrogate markers of beta cell function, including HOMA (Homeostasis Model Assessment), proinsulin to insulin ratio, and measures of beta cell responsiveness from the frequently-sampled meal tolerance test. The observed incidence of hypoglycaemia in patients treated with linagliptin was similar to placebo. Body weight did not differ significantly between the groups.
Linagliptin monotherapy for patients ineligible for metformin: The efficacy and safety of linagliptin monotherapy was also evaluated in patients for whom metformin therapy is inappropriate, due to intolerability or contraindication, in a double blind placebo controlled study of 18 weeks duration, followed by a 34 week safety extension period (placebo patients switched to glimepiride). Linagliptin provided significant improvements in HbA1c, (-0.60% change compared to placebo), from a mean baseline HbA1c of 8.09 %. The mean HbA1c change from baseline remained constant for linagliptin from week 18 to week 52. Linagliptin also showed significant improvements in FPG, and a greater portion of patients achieved a target HbA1c of < 7.0%, compared to placebo. The observed incidence of hypoglycaemia in patients treated with linagliptin was similar to placebo and was lower than seen with glimepiride during the safety extension. Body weight did not differ significantly between the groups during the placebo controlled 18 weeks, and patients treated with glimepiride had an increase in body weight during the safety extension.
Linagliptin monotherapy 12 week data in comparison with placebo, and 26 week data in comparison to an α-glucosidase inhibitor (voglibose): The efficacy and safety of linagliptin monotherapy was also evaluated in Japanese patients in a double blind study versus placebo for 12 weeks duration, and voglibose (α-glucosidase inhibitor) for 26 weeks duration. Linagliptin (5mg) provided significant improvements in HbA1c, (-0.87 % change compared to placebo) after 12 weeks from a mean baseline HbA1c of 8.0 %. Linagliptin (5mg) was also shown to provide significantly better improvements in HbA1c in comparion to voglibose, (-0.32 % change compared to voglibose) after 26 weeks from a mean baseline HbA1c of 8.0 %. Linagliptin also showed significant improvements in FPG and a greater portion of patients achieved a target HbA1c of < 7.0%, compared to both placebo and voglibose. The observed incidence of hypoglycaemia in patients treated with linagliptin was similar to placebo, and voglibose. Body weight did not differ significantly between linagliptin (5mg) and placebo after 12 weeks treatment. Patients treated with linagliptin (5mg), exhibited a small mean decrease from baseline in body weight (-0.16kg) after 26 weeks, compared to a significantly greater mean decrease in body weight in patients administered voglibose (-1.04 kg).
Linagliptin as add on to metformin therapy: The efficacy and safety of linagliptin in combination with metformin was evaluated in a double blind placebo controlled study of 24 weeks duration. Linagliptin provided significant improvements in HbA1c, (-0.64 % change compared to placebo), from a mean baseline HbA1c of 8 %. Linagliptin also showed significant improvements in FPG, 2-hour PPG by -67.1 mg/dl (-3.7 mmol/L) compared to placebo and a greater portion of patients achieved a target HbA1c of < 7.0% (28.3% on linagliptin vs. 11.4% on placebo). The observed incidence of hypoglycaemia in patients treated with linagliptin was similar to placebo. Body weight did not differ significantly between the groups.
Studies conducted using combinations of linagliptin 2.5mg tablet and varying strengths of metformin: The efficacy and safety of linagliptin in combination with metformin was evaluated in a 24-week placebo-controlled factorial study of initial therapy. Linagliptin 2.5 mg twice daily in combination with metformin (500 mg or 1000 mg twice daily) provided significant improvements in glycemic parameters compared with either monotherapy (mean baseline HbA1c 8.65%). The mean treatment difference in HbA1c between linagliptin+metformin combination therapy versus metformin monotherapy from baseline to Week 24 (LOCF) was -0.51% (95% CI -0.73, -0.30; p<0.0001) for linagliptin 2.5 mg+metformin 1000 mg twice daily compared to metformin 1000 mg twice daily, -0.58% (95% CI - 0.79, -0.36; p<0.0001) for linagliptin 2.5 mg+metformin 500 mg twice daily compared to metformin 500 mg twice daily. The placebo-corrected mean HbA1c change from baseline for linagliptin 2.5/metformin 1000 mg twice daily were 1.71% which led to HbA1c control (<7.0%) in 53.6% of patients (compared to 30.7% on monotherapy with metformin 1000 mg twice daily). Mean reductions from baseline in HbA1c were generally greater for patients with higher baseline HbA1c values. Effects on plasma lipids were generally neutral. The decrease in body weight with the combination of linagliptin and metformin was similar to that observed for metformin alone or placebo; there was no change from baseline for patients on linagliptin alone. The incidence of hypoglycaemia was similar across treatment groups (placebo 1.4%, linagliptin 5 mg 0%, metformin 2.1%, and linagliptin 2.5mg plus metformin twice daily 1.4%). In addition, this study included patients (n=66) with more severe hyperglycemia (HbA1c at baseline >/=11%) who were treated with twice daily open-label linagliptin 2.5 mg and metformin 1000 mg. In this group of patients, the mean baseline HbA1c value was 11.8% and mean FPG was 261.8 mg/dL. A mean decrease from baseline of -3.74% in HbA1c (n=48) and -81.2 mg/dL for FPG (n=41) was observed for patients completing the 24 week trial period without rescue therapy. In the LOCF analysis including all patients with primary endpoint measurements (n=65) at last observation without rescue therapy changes from baseline were -3.19% for HbA1c and -73.6 mg/dL for FPG.
The efficacy and safety of linagliptin 2.5 mg twice daily versus 5 mg once daily in combination with metformin in patients with insufficient glycemic control on metformin monotherapy was evaluated in a double blind placebo controlled study of 12 weeks duration. Linagliptin (2.5 mg twice daily and 5 mg once daily) added to metformin provided significant improvements in glycemic parameters compared with placebo. Linagliptin 5 mg once daily and 2.5 mg twice daily provided comparable (CI: -0.07; 0.19) significant HbA1c reductions of -0.80 % (from baseline 7.98%), and -0.74 (from baseline 7.96%) compared to placebo. The observed incidence of hypoglycaemia in patients treated with linagliptin was similar to placebo. Body weight did not differ significantly between the groups.
Linagliptin as add on to sulphonylurea therapy: The efficacy and safety of linagliptin in combination with sulphonylurea was evaluated in a double blind placebo controlled study of 18 weeks duration. Linagliptin provided significant improvements in HbA1c, (-0.47 % change compared to placebo), from a mean baseline HbA1c of 8.6%. Linagliptin also showed significant improvements in patients achieving a target HbA1c of < 7.0%. Body weight did not differ significantly between the groups.
Linagliptin as add on to insulin therapy: The efficacy and safety of the addition of linagliptin 5 mg to insulin alone or in combination with metformin and/or pioglitazone has been evaluated in a double blind placebo controlled study over 24 weeks duration. The mean treatment difference in HbA1c between linagliptin versus placebo from baseline to Week 24 (LOCF) was -0.65% (95% CI -0.74, -0.55; p<0.0001) from a mean baseline HbA1c of 8.3 %. Mean reductions from baseline in HbA1c were generally greater for patients with higher baseline HbA1c values. The mean HbA1c change from baseline was sustained for linagliptin from week 12 to week 24. Linagliptin also showed significant improvements in FPG of -11.25 mg/dL (95% CI -16.14, -6.36; p<0.0001) compared to placebo, and a greater portion of patients achieved a target HbA1c of < 7.0%, compared to placebo. This was achieved with a stable insulin dose. After 24 weeks of treatment, the mean daily insulin dose at baseline was 42 units in patients treated with linagliptin and 40 units in placebo-treated patients. The mean change from baseline to Week 24 in daily dose of insulin was 1.3 IU in the placebo group and 0.6 IU in the linagliptin group. Body weight did not differ significantly between the groups. Effects on plasma lipids were neutral. The incidence of hypoglycaemia was similar across treatment groups (22.2% linagliptin; 21.2% placebo).
Linagliptin as add on to a combination of metformin and sulphonylurea therapy: A placebo controlled study of 24 weeks in duration was conducted to evaluate the efficacy and safety of linagliptin 5 mg to placebo, in patients not sufficiently treated with a combination with metformin and a sulphonylurea. Linagliptin provided significant improvements in HbA1c (-0.62 % change compared to placebo), from a mean baseline HbA1c of 8.14%. Linagliptin also showed significant improvements in patients achieving a target HbA1c of < 7.0%, and also for fasting plasma glucose (FPG), compared to placebo. Body weight did not differ significantly between the groups.
Linagliptin as add on to a combination of metformin and empagliflozin: In patients inadequately controlled with metformin and empagliflozin (10 mg (n=247) or 25 mg (n=217)), 24-weeks treatment with add-on therapy of linagliptin 5 mg provided adjusted mean HbA1c reductions from baseline by -0.53% (significant difference to add-on placebo -0.32% (95% CI -0.25, -0.13) and -0.58% (significant difference to add-on placebo -0.47% (95% CI -0.66; -0.28), respectively. A statistically significant greater proportion of patients with a baseline HbA1c ≥7.0% and treated with linagliptin 5 mg achieved a target HbA1c of <7% compared to placebo.
In prespecified subgroups of patients with baseline HbA1c greater or equal than 8.5% (n=66 and n=42 patients on metformin plus empagliflozin 10 mg or 25 mg, respectively), the adjusted mean HbA1c reductions from baseline to 24 weeks on add-on therapy with linagliptin 5 mg were -0.97% (p=0.0875, for difference to add-on placebo) and -1.16% (p=0.0046, for difference to add-on placebo), respectively.
Linagliptin 24 month data, as add onto metformin in comparison with glimepiride: In a study comparing the efficacy and safety of the addition of linagliptin 5 mg or glimepiride (a sulphonylurea agent) in patients with inadequate glycaemic control on metformin monotherapy, linagliptin was similar to glimepiride in reducing HbA1c, with a mean treatment difference in HbA1c from baseline to 104 weeks for linagliptin compared to glimepiride of +0.20%. In this study, the proinsulin to insulin ratio, a marker of efficiency of insulin synthesis and release, showed a statistically significant improvement with linagliptin compared with glimepiride treatment. The incidence of hypoglycaemia in the linagliptin group (7.5%) was significantly lower than that in the glimepiride group (36.1%). Patients treated with linagliptin exhibited a significant mean decrease from baseline in body weight compared to a significant weight gain in patients administered glimepiride (-1.39 vs +1.29 kg).
Linagliptin as add on therapy in patients with severe renal impairment, 12 week placebo controlled data (stable background) and 40 week placebo controlled extension (adjustable background): The efficacy and safety of linagliptin was also evaluated in type 2 diabetes patients with severe renal impairment in a double blind study versus placebo for 12 weeks duration, during which background glycaemic therapies were kept stable. Patients were on a variety on background therapies including insulin, sulphonylurea, glinides and pioglitazone. There was a follow up 40 week period during which dose adjustments in antidiabetes background therapies were allowed.
Linagliptin provided significant improvements in HbA1c (-0.59 % change compared to placebo), from a mean baseline HbA1c of 8.2%. A greater portion of patients achieved a target HbA1c of < 7.0%, compared to placebo. The observed difference in HbA1c over placebo was -0.72% after 52 weeks.
Body weight did not differ significantly between the groups. The observed incidence of hypoglycaemia in patients treated with linagliptin was higher than placebo, due to an increase in asymptomatic hypoglycaemic events. This can be attributed to the antidiabetes background therapies (insulin and sulphonylurea or glinides). There was no difference between groups in severe hypoglycaemic events.
Linagliptin as add on therapy in elderly patients (age ≥ 70 years) with type 2 diabetes: The efficacy and safety of linagliptin in elderly (age ≥ 70years) type 2 diabetes patients has been evaluated in a double blind study versus placebo for 24 weeks duration. Patients received metformin and/or sulphonylurea and/or insulin as background therapy. Doses of background antidiabetic medications were kept stable during the first 12 weeks, after which adjustments were permitted. Linagliptin provided significant improvements in HbA1c of -0.64 % (95% CI - 0.81, -0.48; p<0.0001) compared to placebo after 24 weeks, from a mean baseline HbA1c of 7.8%. Linagliptin also showed significant improvements in FPG of -20.7mg/dL (95% CI -30.2, -11.2; p<0.0001) compared to placebo (-1.1 mmol/L). Body weight did not differ significantly between the groups. Mild hypoglycaemia was reported in a higher proportion of patients on linagliptin than placebo but the difference between the groups was attributed to background sulphonylurea. Hypoglycaemia rates were also comparable on a background of insulin with or without metformin (13 of 35 patients, 37.1% treated with linagliptin and 6 of 15 patients, 40.0% treated with placebo). However, on a background of sulphonylurea with or without metformin, hypoglycaemia was reported in a higher proportion of patients treated with linagliptin (24 of 82 patients, 29.3%) compared to placebo (7 of 42 patients, 16.7%). There was no difference between groups in severe hypoglycaemic events.
Initial combination with Linagliptin and Metformin in recently diagnosed treatment naïve patients with marked hyperglycaemia: The efficacy and safety of the initial combination of linagliptin 5 mg once daily and metformin twice daily (uptitrated in the first 6 weeks to 1500 mg or 2000 mg/d) compared to linagliptin 5 mg once daily has been studied in a 24 week trial in recently diagnosed treatment naive patients with type 2 diabetes mellitus and marked hyperglycaemia (baseline HbA1c 8.5-12.0%). After 24 weeks both linagliptin monotherapy as well as the initial combination of linagliptin and metformin significantly reduced HbA1c levels by -2.0% and -2.8% respectively, from a baseline HbA1c of 9.69% and 9.73% respectively (per protocol completers cohort). The treatment difference of -0.8% (95% CI -1.1 to -0.5) showed superiority for the initial combination over monotherapy (p<0.0001). Notably, 40% and 61% of patients in the monotherapy and combination arms achieved HbA1c <7.0%.
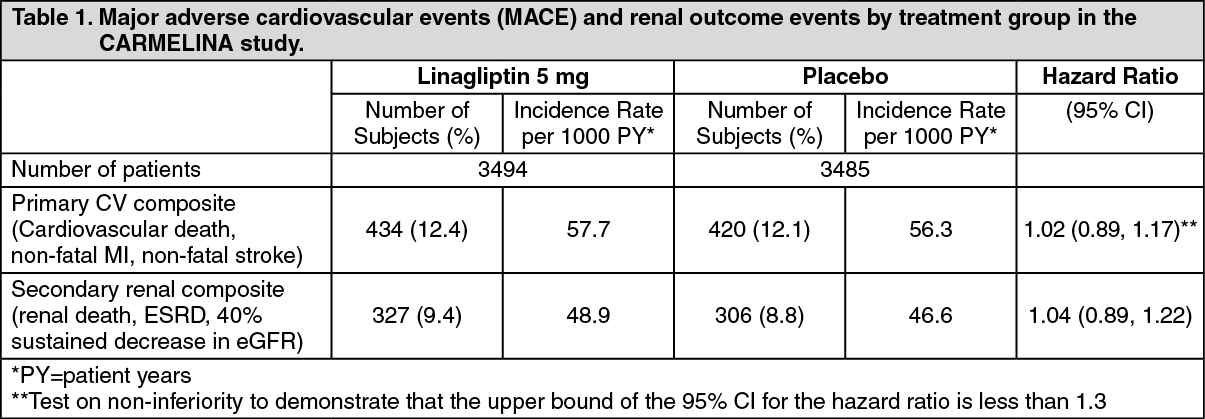
Linagliptin cardiovascular and renal safety study (CARMELINA): CARMELINA was a randomized study in 6979 patients with type 2 diabetes with increased CV risk evidenced by a history of established macrovascular or renal disease who were treated with linagliptin 5 mg (3494) or placebo (3485) added to standard of care targeting regional standards for HbA
1c, CV risk factors and renal disease. The study population included 1,211 (17.4%) patients ≥ 75 years of age and 4,348 (62.3%) patients with renal impairment. Approximately 19% of the population had eGFR ≥45 to <60 mL/min/1.73 m
2, 28% of the population had eGFR ≥30 to <45 mL/min/1.73 m
2 and 15% had eGFR < 30 mL/min/1.73 m
2.
The mean HbA
1c at baseline was 8.0%.
The study was designed to demonstrate non-inferiority for the primary cardiovascular endpoint which was a composite of the first occurrence of cardiovascular death or a non-fatal myocardial infarction (MI) or a non-fatal stroke (3P-MACE). The renal composite endpoint was defined as renal death or sustained end stage renal disease or sustained decrease of 40% or more in eGFR.
After a median follow up of 2.2 years, linagliptin, when added to standard of care, did not increase the risk of major adverse cardiovascular events or renal outcome events (Table 1 and figure). There was no increased risk in hospitalization for heart failure which was an additional adjudicated endpoint observed compared to standard of care without linagliptin in patients with type 2 diabetes (Table 2). (See Tables 1 and 2 and figure.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In analyses for albuminuria progression (change from normoalbuminuria to micro- or macroalbuminuria, or from microalbuminuria to macroalbuminuria) the estimated hazard ratio was 0.86 (95% CI 0.78, 0.95) for linagliptin versus placebo. The microvascular endpoint was defined as the composite of renal death, sustained ESRD, sustained decrease of ≥50% in eGFR, albuminuria progression, use of retinal photocoagulation or intravitreal injections of an anti-VEGF therapy for diabetic retinopathy or vitreous haemorrhage or diabetes-related-blindness. The estimated hazard ratio for time to first occurrence for the composite microvascular endpoint was 0.86 (95% CI 0.78, 0.95) for linagliptin versus placebo, mainly driven by albuminuria progression.
Linagliptin cardiovascular safety study (CAROLINA): CAROLINA was a randomized study in 6033 patients with early type 2 diabetes and increased CV risk or established complications who were treated with linagliptin 5 mg (3023) or glimepiride 1- 4 mg (3010) added to standard of care (including background therapy with metformin in 83% of patients) targeting regional standards for HbA
1c and CV risk factors. The mean age for study population was 64 years and included 2030 (34%) patients ≥ 70 years of age. The study population included 2089 (35%) patients with cardiovascular disease and 1130 (19%) patients with renal impairment with an eGFR < 60ml/min/1.73m2 at baseline. The mean HbA
1c at baseline was 7.15%.
The study was designed to demonstrate non-inferiority for the primary cardiovascular endpoint which was a composite of the first occurrence of cardiovascular death or a non-fatal myocardial infarction (MI) or a non-fatal stroke (3P-MACE).
After a median follow up of 6.25 years, linagliptin did not increase the risk of major adverse cardiovascular events (Table 3) as compared to glimepiride. Results were consistent for patients treated with or without metformin. (See Table 3.)
Click on icon to see table/diagram/image
The composite of treatment sustainability, a key secondary endpoint, was defined as the proportion of patients on study treatment following initial titration period (16 weeks) that maintain glycaemic control (HbA
1c ≤ 7.0%) at final visit without need for additional antidiabetic drug therapy (rescue medication) without any moderate (symptomatic with glucose value ≤ 70mg/dL) or severe (requiring assistance) hypoglycaemic episodes and without > 2% weight gain. A higher number of patients on linagliptin (481, 16.0%) achieved this key secondary endpoint compared to glimepiride (305, 10.2%).
For the entire treatment period (median time on treatment 5.9 years) the rate of patients with moderate or severe hypoglycaemia was 6.5% on linagliptin versus 30.9% on glimepiride, severe hypoglycaemia occurred in 0.3% of patients on linagliptin versus 2.2% on glimepiride.
Pharmacokinetics: The pharmacokinetics of linagliptin has been extensively characterized in healthy subjects and patients with type 2 diabetes. After oral administration of a 5 mg dose to healthy volunteers or patients, linagliptin was rapidly absorbed, with peak plasma concentrations (median Tmax) occurring 1.5 hours postdose.
Plasma concentrations of linagliptin decline in at least bi-phasic manner with a long terminal half-life (terminal half- life for linagliptin more than 100 hours), that is mostly related to the saturable, tight binding of linagliptin to DPP-4 and does not contribute to the accumulation of the drug. The effective half-life for accumulation of linagliptin, as determined from oral administration of multiple doses of 5 mg linagliptin, is approximately 12 hours. After once-daily dosing, steady-state plasma concentrations of 5 mg linagliptin are reached by the third dose. Plasma AUC of linagliptin increased approximately 33% following 5 mg doses at steady-state compared to the first dose. The intra-subject and inter-subject coefficients of variation for linagliptin AUC were small (12.6% and 28.5%, respectively). Plasma AUC of linagliptin increased in a less than dose-proportional manner in the dose range of 1 to 10mg. The pharmacokinetics of linagliptin was generally similar in healthy subjects and in patients with type 2 diabetes.
Absorption: The absolute bioavailability of linagliptin is approximately 30%. Because coadministration of a high-fat meal with linagliptin had no clinically relevant effect on the pharmacokinetics, linagliptin may be administered with or without food.
In vitro studies indicated that linagliptin is a substrate of P-glycoprotein and of CYP3A4. Ritonavir, a potent inhibitor of P-glycoprotein and CYP3A4, led to a twofold increase in exposure (AUC) and multiple co-administration of linagliptin with rifampicin, a potent inducer of P-gp and CYP3A, resulted in an about 40% decreased linagliptin steady-state AUC, presumably by increasing/decreasing the bioavailability of linagliptin by inhibition/induction of P- glycoprotein.
Distribution: As a result of tissue binding, the mean apparent volume of distribution at steady state following a single 5 mg intravenous dose of linagliptin to healthy subjects is approximately 1110 litres, indicating that linagliptin extensively distributes to the tissues. Plasma protein binding of linagliptin is concentration-dependent, decreasing from about 99% at 1 nmol/L to 75-89% at ≥30 nmol/L, reflecting saturation of binding to DPP-4 with increasing concentration of linagliptin. At high concentrations, where DPP-4 is fully saturated, 70-80% of linagliptin was bound to other plasma proteins than DPP-4, hence - 20-30% were unbound in plasma.
Biotransformation: Following a [
14C] linagliptin oral 10 mg dose, approximately 5% of the radioactivity was excreted in urine. Metabolism plays a subordinate role in the elimination of linagliptin. One main metabolite with an relative exposure of 13.3 % of linagliptin at steady state was detected which was found to be pharmacologically inactive and thus does not contribute to the plasma DPP-4 inhibitory activity of linagliptin.
Excretion: Following administration of an oral [
14C] linagliptin dose to healthy subjects, approximately 85% of the administered radioactivity was eliminated in faeces (80%) or urine (5%) within 4 days of dosing. Renal clearance at steady state was approximately 70 mL/min.
Special Populations: Renal Impairment: A multiple-dose, open-label study was conducted to evaluate the pharmacokinetics of linagliptin (5 mg dose) in patients with varying degrees of chronic renal impairment compared to normal healthy control subjects. The study included patients with renal impairment classified on the basis of creatinine clearance as mild (50 to <80 mL/min), moderate (30 to <50 mL/min), and severe (<30 mL/min), as well as patients with ESRD on hemodialysis. In addition patients with T2DM and severe renal impairment (<30 mL/min) were compared to T2DM patients with normal renal function. Creatinine clearance was measured by 24-hour urinary creatinine clearance measurements or estimated from serum creatinine based on the Cockcroft-Gault formula: (See equation.)
Click on icon to see table/diagram/image
Under steady-state conditions, linagliptin exposure in patients with mild renal impairment was comparable to healthy subjects. In moderate renal impairment, a moderate increase in exposure of about 1.7-fold was observed compared with control. Exposure in T2DM patients with severe RI was increased by about 1.4-fold compared to T2DM patients with normal renal function. Steady-state predictions for AUC of linagliptin in patients with ESRD indicated comparable exposure to that of patients with moderate or severe renal impairment. In addition, linagliptin is not expected to be eliminated to a therapeutically significant degree by haemodialysis or peritoneal dialysis. Therefore, no dosage adjustment of linagliptin is necessary in patients with any degree of renal impairment. In addition, mild renal impairment had no effect on linagliptin pharmacokinetics in patients with type 2 diabetes as assessed by population pharmacokinetic analyses.
Hepatic Impairment: In patients with mild moderate and severe hepatic impairment (according to the Child-Pugh classification), mean AUC and C
max of linagliptin were similar to healthy matched controls following administration of single/multiple 5 mg doses of linagliptin (patients with severe hepatic impairment received a single dose only). Model-based predictions of steady-state profiles for patients with severe hepatic impairment gave no indication for an increased exposure upon multiple dosing. No dosage adjustment for linagliptin is necessary for patients with mild, moderate or severe hepatic impairment.
Body Mass Index (BMI): No dosage adjustment is necessary based on BMI. Body mass index had no clinically relevant effect on the pharmacokinetics of linagliptin based on a population pharmacokinetic analysis of Phase I and Phase II data.
Gender: No dosage adjustment is necessary based on gender. Gender had no clinically relevant effect on the pharmacokinetics of linagliptin based on a population pharmacokinetic analysis of Phase I and Phase II data.
Geriatric: No dosage adjustment is required based on age, as age did not have a clinically relevant impact on the pharmacokinetics of linagliptin based on a population pharmacokinetic analysis of Phase I and Phase II data. Elderly subjects (65 to 80 years) had comparable plasma concentrations of linagliptin compared to younger subjects.
Paediatric: Studies characterizing the pharmacokinetics of linagliptin in paediatric patients have not been yet performed.
Race: No dosage adjustment is necessary based on race. Race had no obvious effect on the plasma concentrations of linagliptin based on a composite analysis of available pharmacokinetic data, including patients of Caucasian, Hispanic, African-American, and Asian origin. In addition the pharmacokinetic characteristics of linagliptin were found to be similar in dedicated phase I studies in Japanese, Chinese, Caucasian healthy volunteers and African American type 2 diabetes patients.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image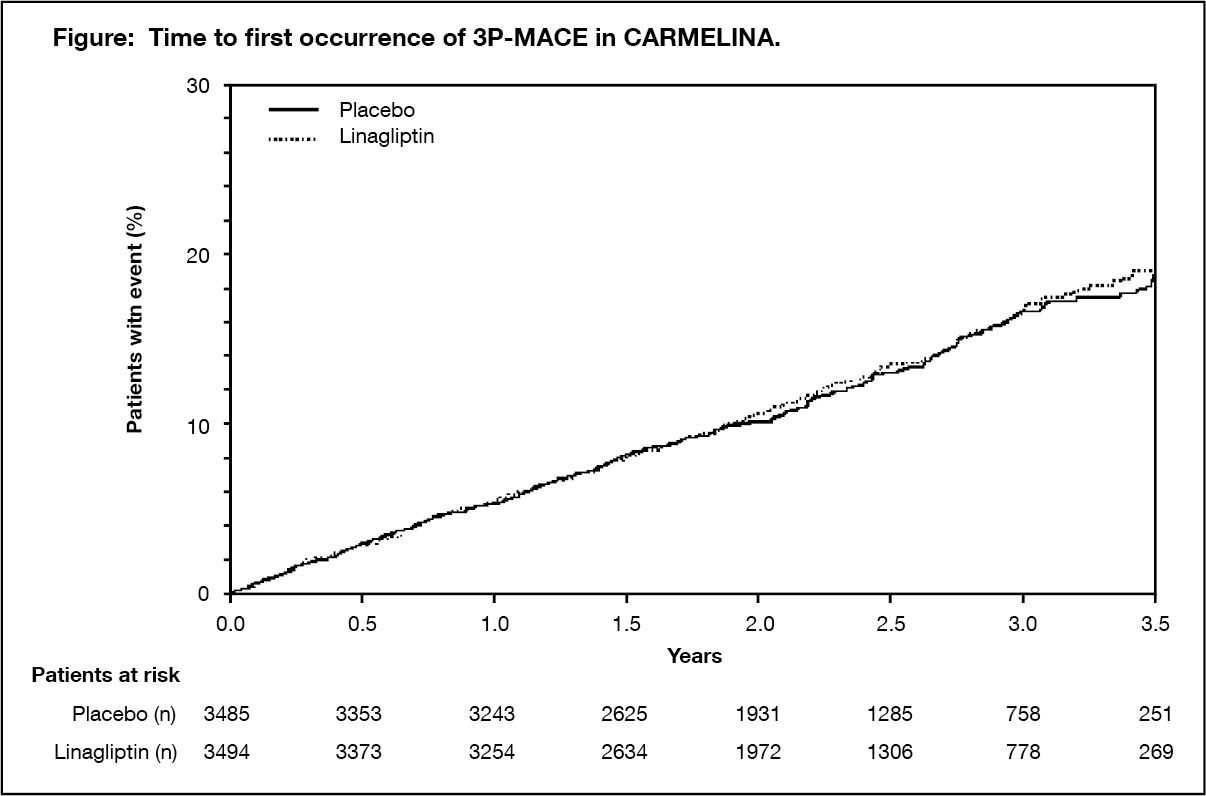 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image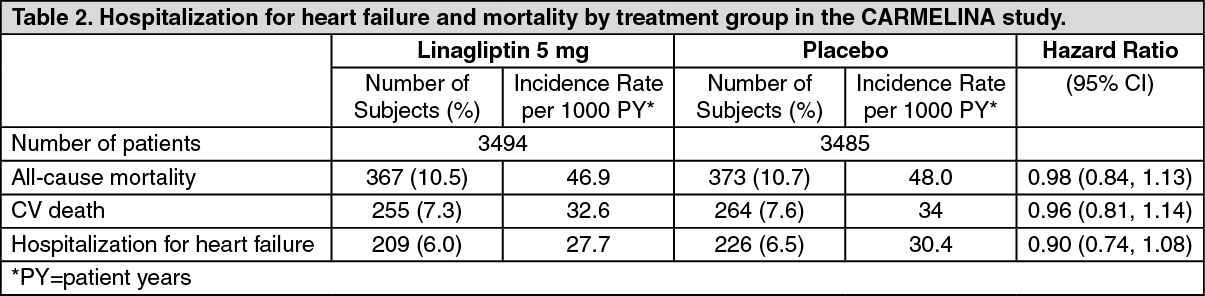 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image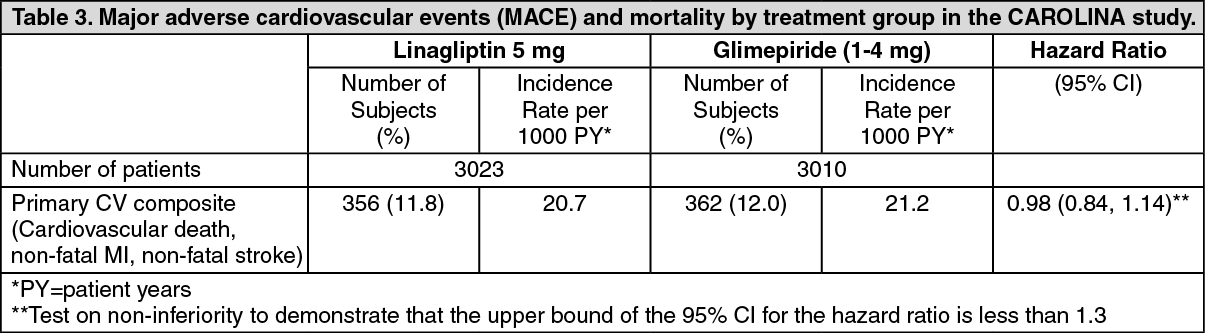 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image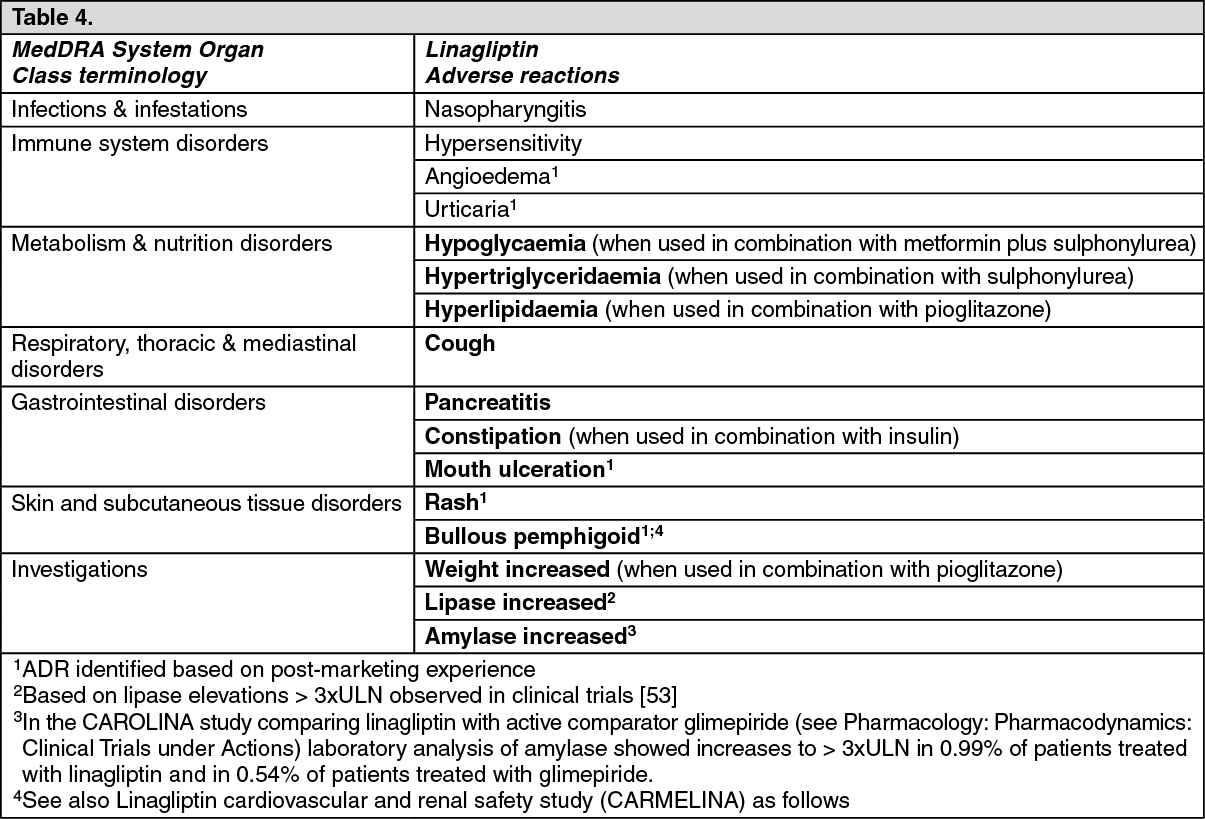 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out