


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of action: Paclitaxel is an antimicrotubule agent that promotes the assembly of microtubules from tubulin dimers and stabilises microtubules by preventing depolymerisation. This stability results in the inhibition of the normal dynamic reorganisation of the microtubule network that is essential for vital interphase and mitotic cellular functions. In addition, paclitaxel induces abnormal arrays or "bundles" of microtubules throughout the cell cycle and multiple asters of microtubules during mitosis.
Abraxane contains human serum albumin-paclitaxel nanoparticles of approximately 130 nm in size, where the paclitaxel is present in a non-crystalline, amorphous state. Upon intravenous administration, the nanoparticles dissociate rapidly into soluble, albumin bound paclitaxel complexes of approximately 10 nm in size. Albumin is known to mediate endothelial caveolar transcytosis of plasma constituents, and in vitro studies demonstrated that the presence of albumin in Abraxane enhances transport of paclitaxel across endothelial cells. It is hypothesised that this enhanced transendothelial caveolar transport is mediated by the gp-60 albumin receptor, and that there is enhanced accumulation of paclitaxel in the area of tumour due to the albumin-binding protein Secreted Protein Acidic Rich in Cysteine (SPARC).
Clinical efficacy and safety: Breast cancer: Data from 106 patients accrued in two single-arm open-label studies and from 454 patients treated in a randomised Phase III comparative study are available to support the use of Abraxane in metastatic breast cancer. This information is presented below.
Single-arm open-label studies: In one study, Abraxane was administered as a 30-minute infusion at a dose of 175 mg/m2 to 43 patients with metastatic breast cancer. The second trial utilised a dose of 300 mg/m2 as a 30 minute infusion in 63 patients with metastatic breast cancer. Patients were treated without steroid pre-treatment or planned G-CSF support. Cycles were administered at 3 week intervals. The response rates in all patients were 39.5% (95% CI: 24.9%-54.2%) and 47.6% (95% CI: 35.3%-60.0%), respectively. The median time to disease progression was 5.3 months (175 mg/m2; 95% CI: 4.6-6.2 months) and 6.1 months (300 mg/m2; 95% CI: 4.2-9.8 months).
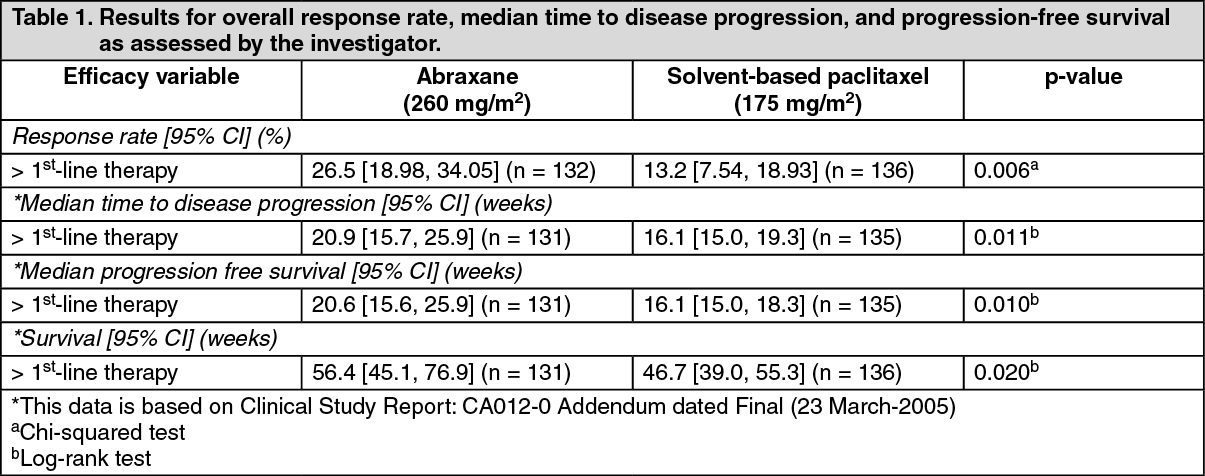
Randomised comparative study: This multi-centre trial was conducted in patients with metastatic breast cancer, who were treated every 3 weeks with single-agent paclitaxel, either as solvent-based paclitaxel 175 mg/m2 given as a 3-hour infusion with premedication to prevent hypersensitivity (N = 225), or as Abraxane 260 mg/m2 given as a 30 minute infusion without premedication (N = 229).
Sixty-four percent of patients had impaired performance status (ECOG 1 or 2) at study entry; 79% had visceral metastases; and 76% had > 3 sites of metastases. Fourteen percent of the patients had not received prior chemotherapy; 27% had received chemotherapy in the adjuvant setting only, 40% in the metastatic setting only, and 19% in both metastatic and adjuvant settings. Fifty-nine percent received study medicinal product as second or greater than second-line therapy. Seventy-seven percent of the patients had been previously exposed to anthracyclines.
Results for overall response rate and time to disease progression, and progression-free survival and survival for patients receiving > 1st-line therapy, are shown below. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTwo hundred and twenty nine patients treated with Abraxane in the randomized, controlled clinical trial were evaluated for safety. Neurotoxicity to paclitaxel was evaluated through improvement by one grade for patients experiencing Grade 3 peripheral neuropathy at any time during therapy. The natural course of peripheral neuropathy to resolution to baseline due to cumulative toxicity of Abraxane after >6 courses of treatment was not evaluated and remains unknown.
Pancreatic adenocarcinoma: A multicenter, multinational, randomized, open-label study was conducted in 861 patients to compare Abraxane/gemcitabine versus gemcitabine monotherapy as first-line treatment in patients with metastatic adenocarcinoma of the pancreas. Abraxane was administered to patients (N = 431) as an intravenous infusion over 30-40 minutes at a dose of 125 mg/m2 followed by intravenous infusion over 30-40 minutes at a dose of 1000 mg/m2 given on Days 1, 8 and 15 of each 28-day cycle. In the comparator treatment arm, gemcitabine monotherapy was administered to patients (N = 430) in accordance with the recommended dose and regimen. Treatment was administered until disease progression or development of an unacceptable toxicity. Of the 431 patients with pancreatic adenocarcinoma who were randomized to receive Abraxane in combination with gemcitabine, the majority (93%) were white, 4% were black and 2% were Asian. 16% had a Karnofsky Performance Status of 100; 42% had a KPS of 90; 35% had a KPS of 80; 7% had a KPS of 70; and <1% of patients had a KPS of below 70. Patients with high cardiovascular risk, history of peripheral artery disease and/or of connective tissue disorders and/or interstitial lung disease were excluded from the study.
Patients received a median treatment duration of 3.9 months in the Abraxane/gemcitabine arm and 2.8 months in the gemcitabine arm. 32% of patients in the Abraxane/gemcitabine arm compared with 15% of patients in the gemcitabine arm received 6 or more months of treatment. For the treated population, the median relative dose intensity for gemcitabine was 75% in the Abraxane/gemcitabine arm and 85% in the gemcitabine arm. The median relative dose intensity of Abraxane was 81%. A higher median cumulative dose of gemcitabine was delivered in the Abraxane/gemcitabine arm (11400 mg/m2) when compared with the gemcitabine arm (9000 mg/m2).
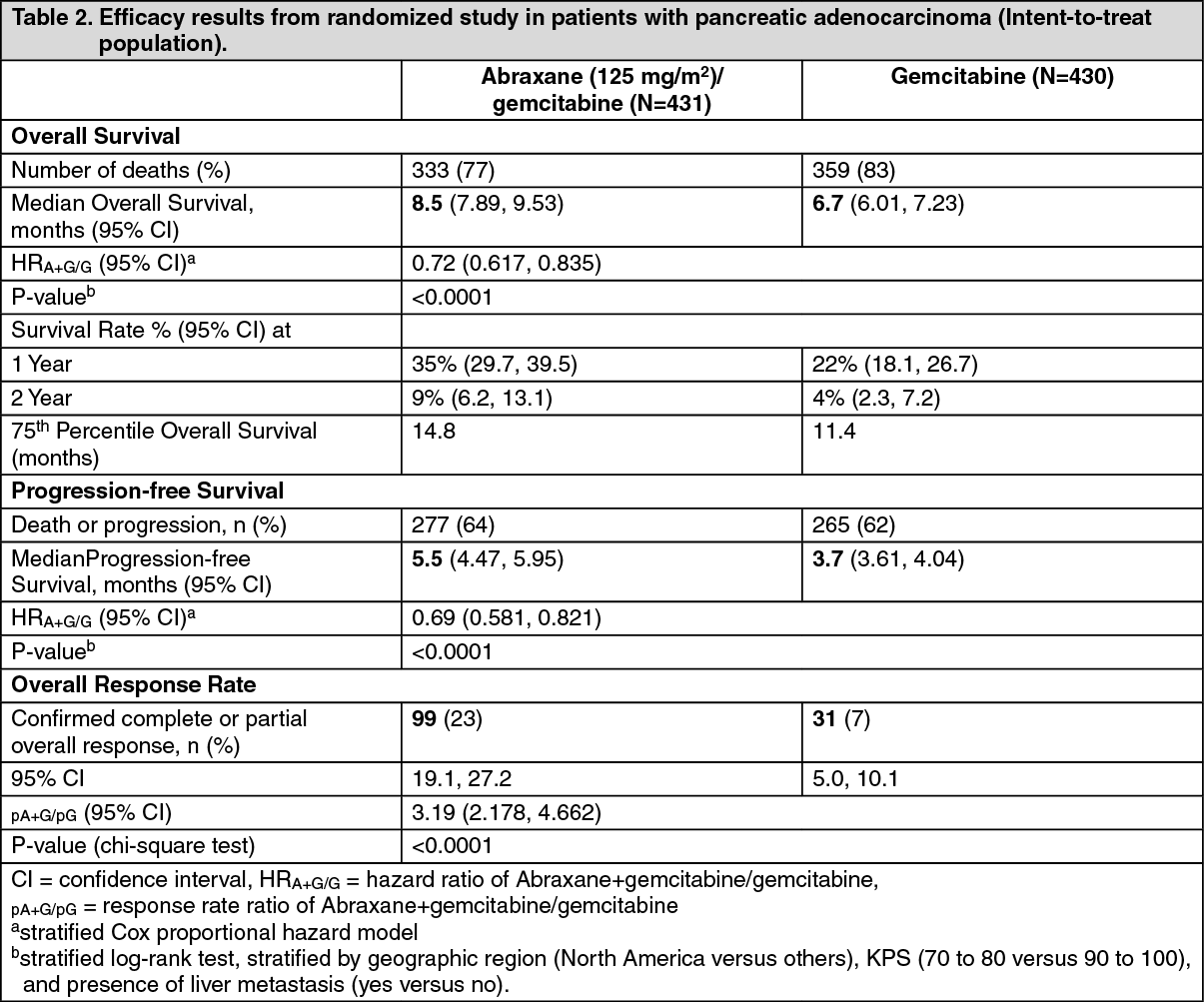
The primary efficacy endpoint was overall survival (OS). The key secondary endpoints were progression-free survival (PFS) and overall response rate (ORR), both assessed by independent, central, blinded radiological review using RECIST guidelines (Version 1.0). (See Table 2.)
 Click on icon to see table/diagram/image
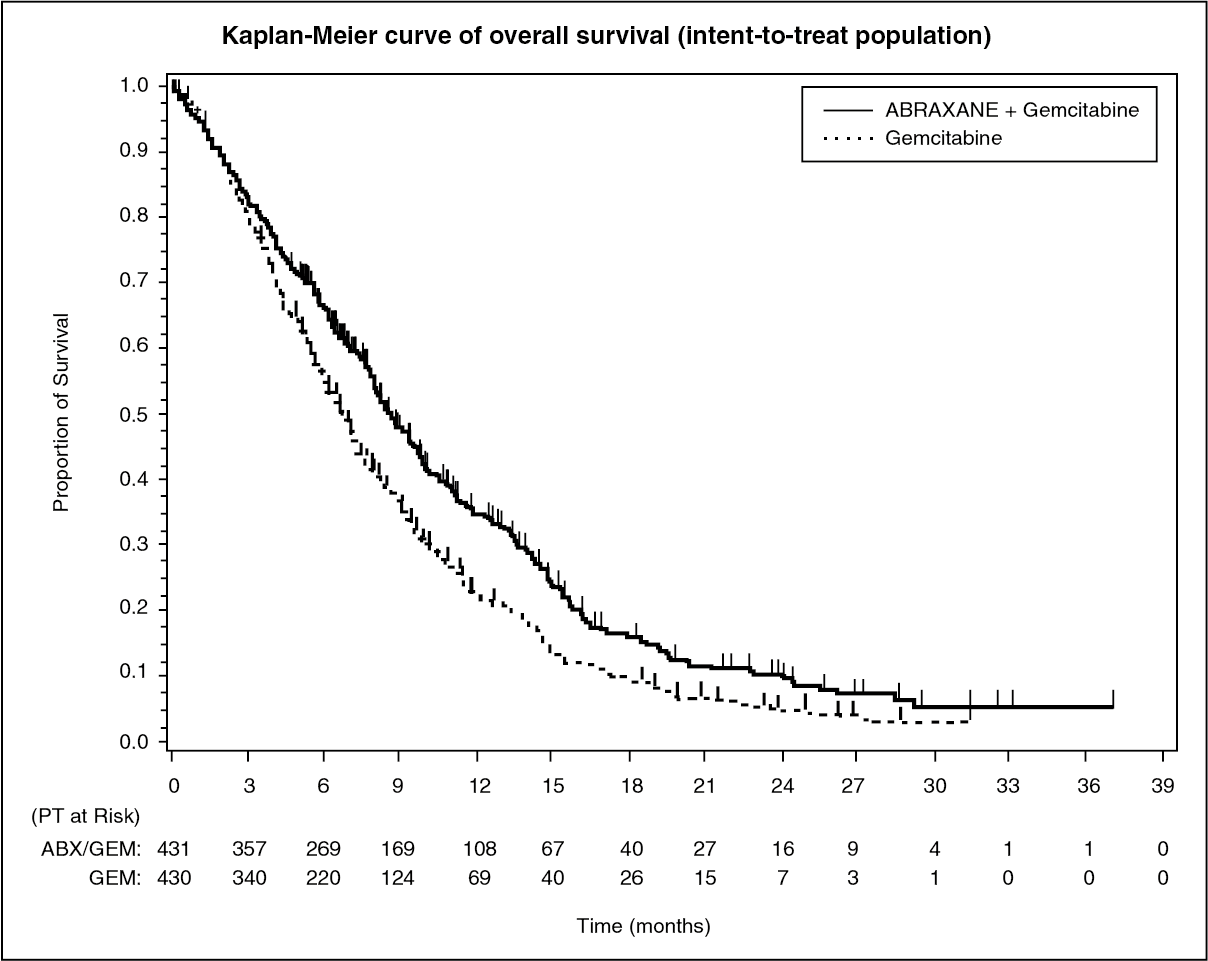
Click on icon to see table/diagram/imageThere was a statistically significant improvement in OS for patients treated with Abraxane/gemcitabine versus gemcitabine alone, with 1.8 months increase in median OS, 28% overall reduction in risk of death, 59% improvement in 1-year survival, and 125% improvement in 2-year survival rates. (See Figure.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTreatment effects on OS favoured the Abraxane/gemcitabine arm across the majority of pre-specified subgroups (including gender, KPS, geographic region, primary location of pancreatic cancer, stage at diagnosis, presence of liver metastases, presence of peritoneal carcinomatosis, prior Whipple procedure, presence of biliary stent at baseline, presence of pulmonary metastases, and number of metastatic sites). For patients ≥ 75 years of age in the Abraxane/gemcitabine and gemcitabine arms the survival Hazard Ratio (HR) was 1.08 (95% CI 0.653, 1.797). For patients with normal baseline CA 19-9 levels the survival HR was 1.07 (95% CI 0.692, 1.661).
There was a statistically significant improvement in PFS for patients treated with Abraxane/gemcitabine versus gemcitabine alone, with 1.8 months increase in median PFS.
Pharmacokinetics: The pharmacokinetics of total paclitaxel following 30- and 180-minute infusions of Abraxane at dose levels of 80 to 375 mg/m2 were determined in clinical studies. The paclitaxel exposure (AUC) increased linearly from 2653 to 16736 ng.hr/ml following dosing from 80 to 300 mg/m2.
In a study in patients with advanced solid tumours, the pharmacokinetic characteristics of paclitaxel following Abraxane administered intravenously at 260 mg/m2 over 30 minutes were compared with those following 175 mg/m2 of the solvent-based paclitaxel injection administered over 3 hours. Based on non-compartmental PK analysis, the plasma clearance of paclitaxel with Abraxane was larger (43%) than that following a solvent-based paclitaxel injection and its volume of distribution was also higher (53%). There were no differences in terminal half-lives.
In a repeat dose study with 12 patients receiving Abraxane administered intravenously at the 260 mg/m2, intrapatient variability in AUC was 19% (range = 3.21%-27.70%). There was no evidence for accumulation of paclitaxel with multiple treatment courses.
Distribution: Following Abraxane administration to patients with solid tumours, paclitaxel is evenly distributed into blood cells and plasma and is highly bound to plasma proteins (94%).
The protein binding of paclitaxel following Abraxane was evaluated by ultrafiltration in a within-patient comparison study. The fraction of free paclitaxel was significantly higher with Abraxane (6.2%) than with solvent-based paclitaxel (2.3%). This resulted in significantly higher exposure to unbound paclitaxel with Abraxane compared with solvent-based paclitaxel, even though the total exposure is comparable. This is possibly due to paclitaxel not being trapped in Cremophor EL micelles as with solvent-based paclitaxel. Based on the published literature, in vitro studies of binding to human serum proteins, (using paclitaxel at concentrations ranging from 0.1 to 50 µg/ml), indicate that the presence of cimetidine, ranitidine, dexamethasone, or diphenhydramine did not affect protein binding of paclitaxel.
Based on population pharmacokinetic analysis, the total volume of distribution is approximately 1741 L; the large volume of distribution indicates extensive extravascular distribution and/or tissue binding of paclitaxel.
Biotransformation and elimination: Based on the published literature, in vitro studies with human liver microsomes and tissue slices show that paclitaxel is metabolised primarily to 6α-hydroxypaclitaxel; and to two minor metabolites, 3'-p-hydroxypaclitaxel and 6α-3'-p-dihydroxypaclitaxel. The formation of these hydroxylated metabolites is catalysed by CYP2C8, CYP3A4, and both CYP2C8 and CYP3A4 isoenzymes, respectively.
In patients with metastatic breast cancer, after a 30-minute infusion of Abraxane at 260 mg/m2, the mean value for cumulative urinary excretion of unchanged active substance accounted for 4% of the total administered dose with less than 1% as the metabolites 6α-hydroxypaclitaxel and 3'-p-hydroxypaclitaxel, indicating extensive non-renal clearance. Paclitaxel is principally eliminated by hepatic metabolism and biliary excretion.
At the clinical dose range of 80 to 300 mg/m2, the mean plasma clearance of paclitaxel ranges from 13 to 30 L/h/m2, and the mean terminal half-life ranges from 13 to 27 hours.
Hepatic impairment: The effect of hepatic impairment on population pharmacokinetics of Abraxane was studied in patients with advanced solid tumours. This analysis included patients with normal hepatic function (n=130), and pre-existing mild (n=8), moderate (n=7), or severe (n=5) hepatic impairment (according to NCI Organ Dysfunction Working Group criteria). The results show that mild hepatic impairment (total bilirubin >1 to ≤1.5 x ULN) has no clinically important effect on pharmacokinetics of paclitaxel. Patients with moderate (total bilirubin >1.5 to ≤3 x ULN) or severe (total bilirubin >3 to ≤5 x ULN) hepatic impairment have a 22% to 26% decrease in the maximum elimination rate of paclitaxel and approximately 20% increase in mean paclitaxel AUC compared with patients with normal hepatic function. Hepatic impairment has no effect on mean paclitaxel Cmax. In addition, elimination of paclitaxel shows an inverse correlation with total bilirubin and a positive correlation with serum albumin.
Pharmacokinetic/pharmacodynamic modeling indicates that there is no correlation between hepatic function (as indicated by the baseline albumin or total bilirubin level) and neutropenia after adjusting for Abraxane exposure.
Pharmacokinetic data are not available for patients with total bilirubin >5 x ULN or for patients with metastatic adenocarcinoma of the pancreas (see Dosage & Administration).
Renal impairment: Population pharmacokinetic analysis included patients with normal renal function (n=65), and pre-existing mild (n=61), moderate (n=23), or severe (n=l) renal impairment (according to draft FDA guidance criteria 2010). Mild to moderate renal impairment (creatinine clearance ≥30 to <90 ml/min) has no clinically important effect on the maximum elimination rate and systemic exposure (AUC and Cmax) of paclitaxel. Pharmacokinetic data are insufficient for patients with severe renal impairment and not available for patients with end stage kidney disease.
Older people: Population pharmacokinetic analysis for Abraxane included patients with ages ranging from 24 to 85 years old and shows that age does not significantly influence the maximum elimination rate and systemic exposure (AUC and Cmax) of paclitaxel.
Pharmacokinetic/pharmacodynamic modelling using data from 125 patients with advanced solid tumours indicates that patients ≥ 65 years of age may be more susceptible to development of neutropenia within the first treatment cycle, although the plasma paclitaxel exposure is not affected by age.
Other intrinsic factors: Population pharmacokinetic analyses for Abraxane indicate that gender, race (Asian vs. White), and type of solid tumours do not have a clinically important effect on systemic exposure (AUC and Cmax) of paclitaxel. Patients weighing 50 kg had paclitaxel AUC approximately 25% lower than those weighing 75 kg. The clinical relevance of this finding is uncertain.
Toxicology: Preclinical safety data: The carcinogenic potential of paclitaxel has not been studied. However, based on the published literature, paclitaxel is a potentially carcinogenic and genotoxic agent at clinical doses, based upon its pharmacodynamic mechanism of action. Paclitaxel has been shown to be clastogenic in vitro (chromosome aberrations in human lymphocytes) and in vivo (micronucleus test in mice). Paclitaxel has been shown to be genotoxic in vivo (micronucleus test in mice), but it did not induce mutagenicity in the Ames test or the Chinese hamster ovary/hypoxanthine-guanine phosphoribosyl transferase (CHO/HGPRT) gene mutation assay.
Paclitaxel at doses below the human therapeutic dose was associated with low fertility when administered prior and during mating in male and female rats and foetal toxicity in rats. Animal studies with Abraxane showed non-reversible, toxic effects on the male reproductive organs at clinically relevant exposure levels.
Paclitaxel and/or its metabolites were excreted into the milk of lactating rats. Following intravenous administration of radiolabelled paclitaxel to rats on days 9 to 10 postpartum, concentrations of radioactivity in milk were higher than in plasma and declined in parallel with the plasma concentrations.