


 Sign Out
Sign Out

In animal models of diabetes, pioglitazone reduces the hyperglycemia, hyperinsulinemia and hypertriglyceridemia characteristic of insulin-resistant states such as type 2 diabetes. The metabolic changes produced by pioglitazone result in increased responsiveness of insulin-dependent tissues and are observed in numerous animal models of insulin resistance.
Since pioglitazone enhances the effects of circulating insulin (by decreasing insulin resistance), it does not lower blood glucose in animal models that lack endogenous insulin.
Pharmacodynamics and Clinical Effects: Clinical studies demonstrate that Actos improves insulin sensitivity in insulin-resistant patients. Actos enhances cellular responsiveness to insulin, increases insulin-dependent glucose disposal, improves hepatic sensitivity to insulin and improves dysfunctional glucose homeostasis. In patients with type 2 diabetes, the decreased insulin resistance produced by Actos results in lower plasma glucose concentrations, plasma insulin levels and hemoglobin A1c values. Based on results from an open-label extension study, the glucose-lowering effects of Actos appear to persist for at least 1 year. In controlled clinical trials, Actos in combination with sulfonylurea, metformin or insulin had an additive effect on glycemic control.
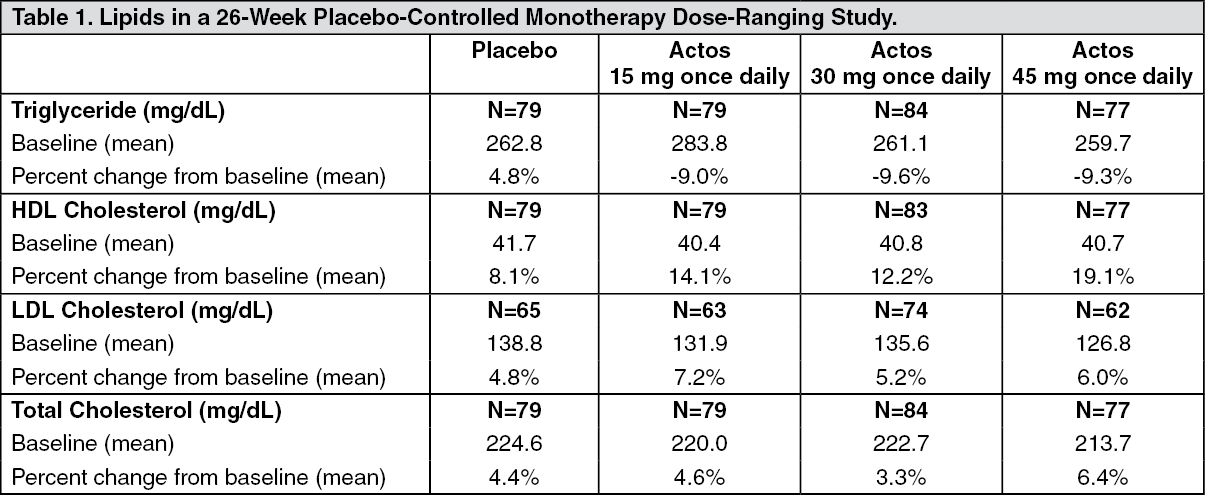
Patients with lipid abnormalities were included in clinical trials with Actos. Overall, patients treated with Actos had mean decreases in triglycerides, mean increases in high-density lipoprotein (HDL) cholesterol and no consistent mean changes in low-density lipoprotein (LDL) and total cholesterol.
In a 26-week, placebo-controlled, dose-ranging study, mean triglyceride levels decreased in the 15-, 30- and 45-mg Actos dose groups compared to a mean increase in the placebo group. Mean HDL levels increased to a greater extent in patients treated with Actos than in the placebo-treated patients. There were no consistent differences for LDL and total cholesterol in patients treated with Actos compared to placebo (see Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the two other monotherapy studies (24 weeks and 16 weeks) and in combination therapy studies with sulfonylurea (24 weeks and 16 weeks) and metformin (24 weeks and 16 weeks), the results were generally consistent with the previous data. In placebo-controlled trials, the placebo-corrected mean changes from baseline decreased 5% to 26% for triglycerides and increased 6% to 13% for HDL in patients treated with Actos. A similar pattern of results was seen in 24-week combination therapy studies of Actos with sulfonylurea or metformin.
In a combination therapy study with insulin (16 weeks), the placebo-corrected mean percent change from baseline in triglyceride values for patients treated with Actos was also decreased. A placebo-corrected mean change from baseline in LDL cholesterol of 7% was observed for the 15 mg dose group. Similar results to those noted previously for HDL and total cholesterol were observed. A similar pattern of results was seen in a 24-week combination therapy study with Actos with insulin.
Clinical Studies: Monotherapy: In the U.S., three randomized, double-blind, placebo-controlled trials with durations from 16 to 26 weeks were conducted to evaluate the use of Actos as monotherapy in patients with type 2 diabetes. These studies examined Actos at doses up to 45 mg or placebo once daily in 865 patients.
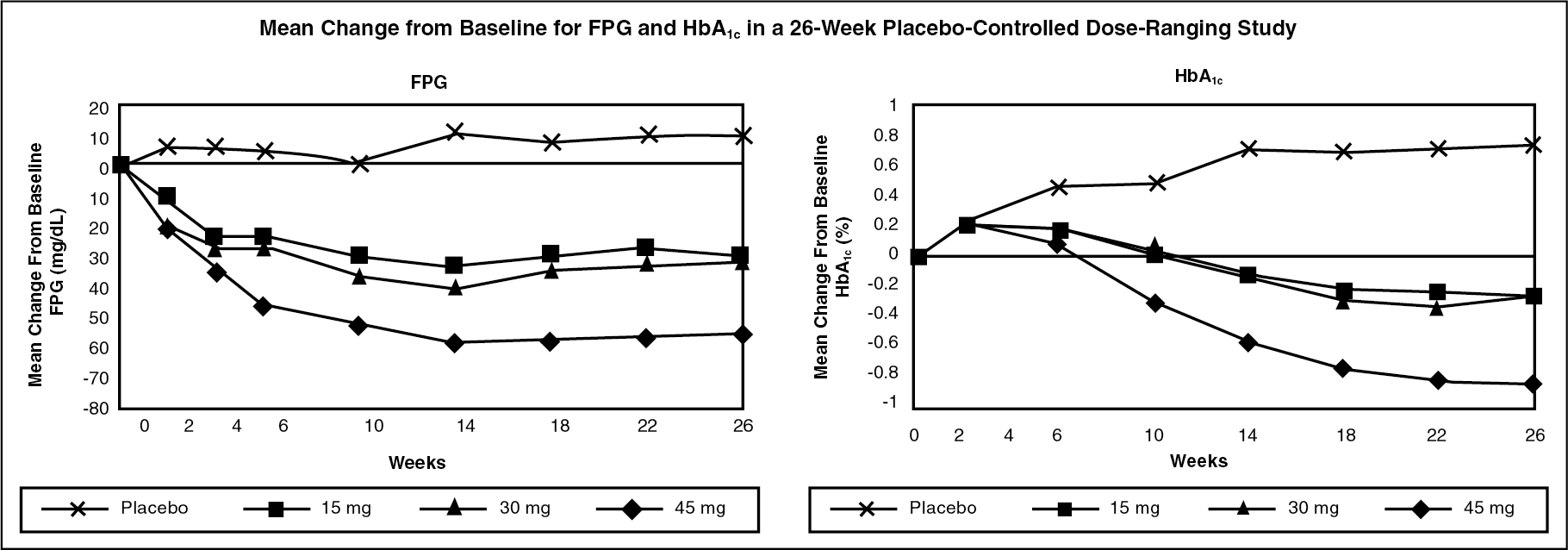
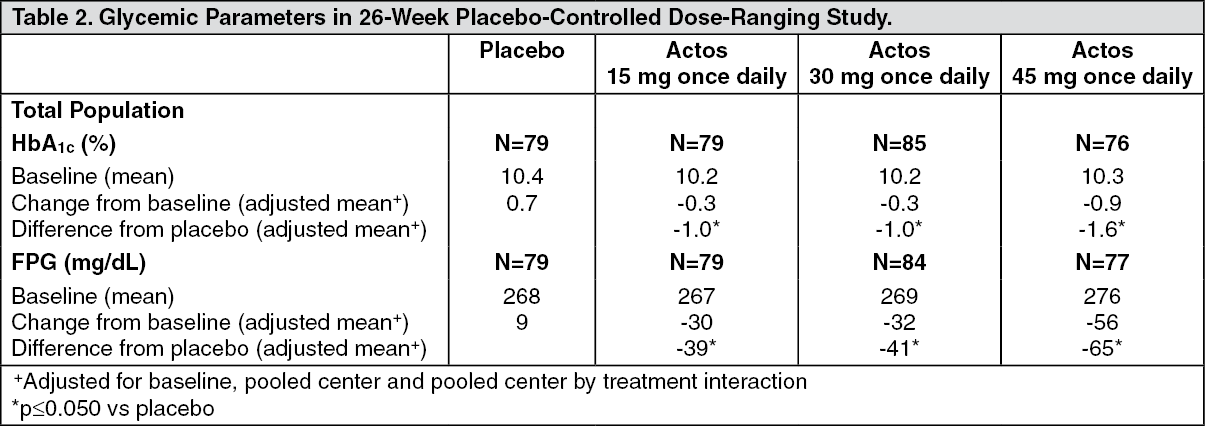
In a 26-week dose-ranging study, 408 patients with type 2 diabetes were randomized to receive 7.5 mg, 15 mg, 30 mg or 45 mg of Actos or placebo once daily. Therapy with any previous antidiabetic agent was discontinued 8 weeks prior to the double-blind period. Treatment with 15 mg, 30 mg and 45 mg of Actos produced statistically significant improvements in HbA1c and fasting plasma glucose (FPG) at endpoint compared to placebo (see Figure and Table 2).
The figure shows the time course for changes in FPG and HbA1c for the entire study population in this 26-week study. (See Figure.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTable 2 shows HbA1c and FPG values for the entire study population. (See Table 2.)
 Click on icon to see table/diagram/image
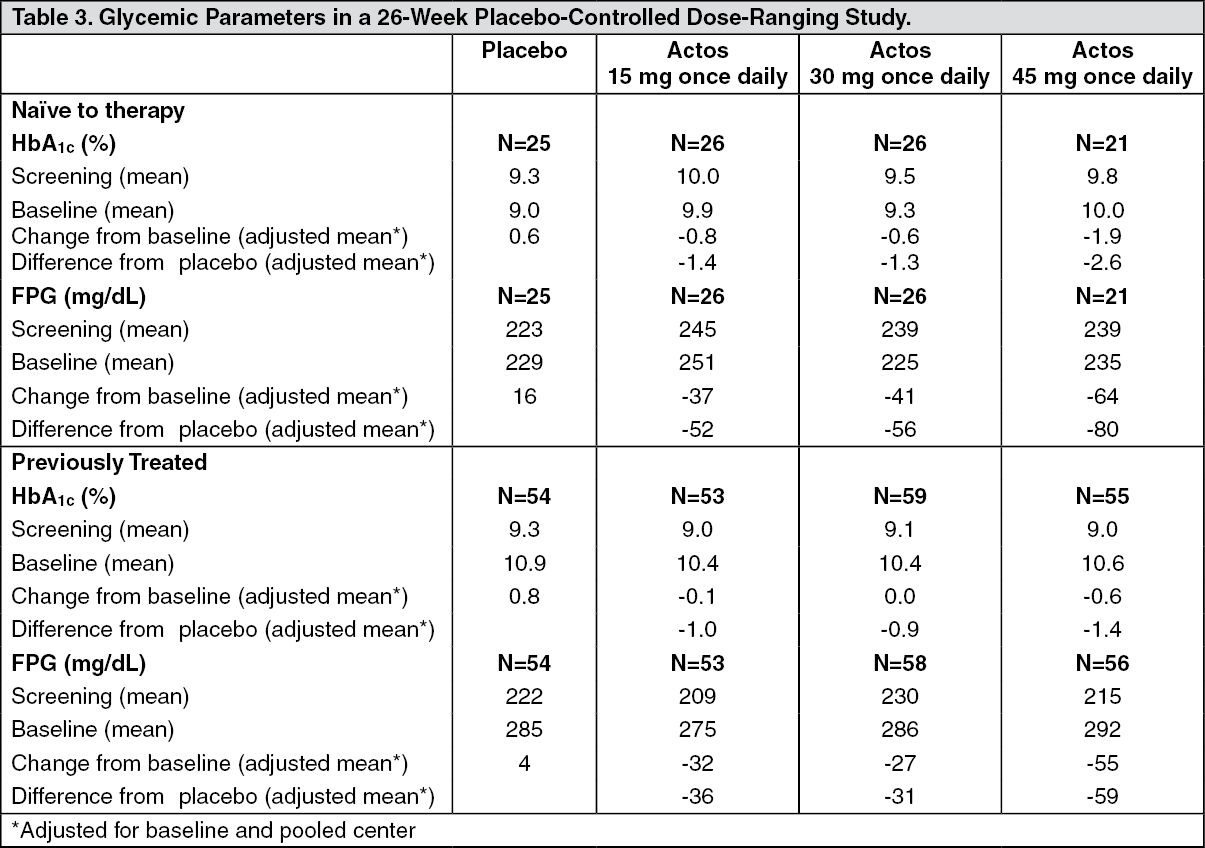
Click on icon to see table/diagram/imageThe study population included patients not previously treated with antidiabetic medication (naïve: 31%) and patients who were receiving antidiabetic medication at the time of study enrollment (previously treated: 69%). The data for the naïve and previously treated patient subsets are shown in Table 3. All patients entered an 8-week washout/run-in period prior to double-blind treatment. This run-in period was associated with little change in HbA1c and FPG values from screening to baseline for the naïve patients; however, for the previously treated group, washout from previous antidiabetic medication resulted in deterioration of glycemic control and increases in HbA1c and FPG. Although most patients in the previously treated group had a decrease from baseline in HbA1c and FPG with Actos, in many cases the values did not return to screening levels by the end of the study. The study design did not permit the evaluation of patients who switched directly to Actos from another antidiabetic agent. (See Table 3.)
 Click on icon to see table/diagram/image
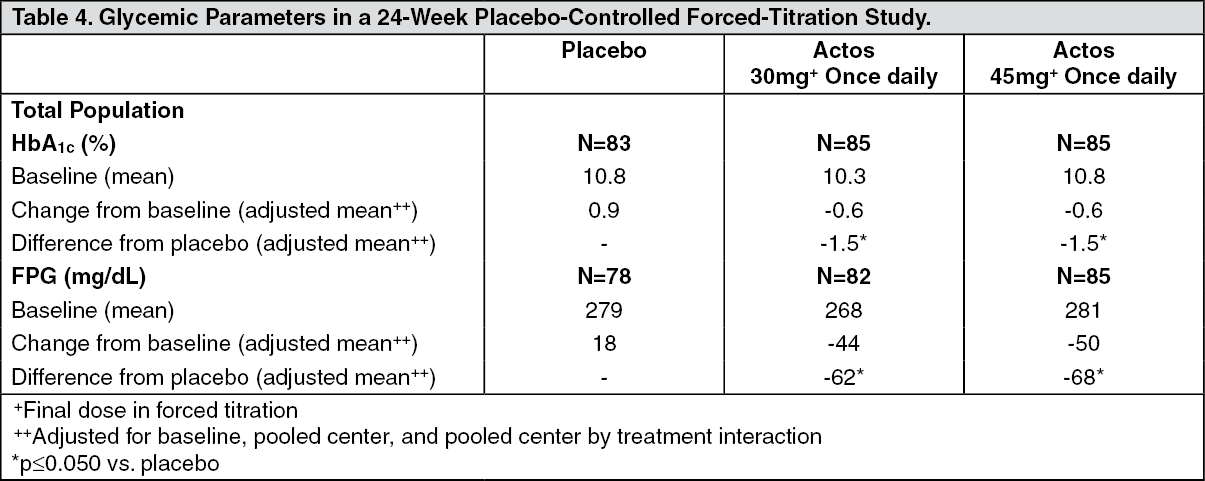
Click on icon to see table/diagram/imageIn a 24-week placebo-controlled study, 260 patients with type 2 diabetes were randomized to one of two forced-titration Actos treatment groups or a mock titration placebo group. Therapy with any previous antidiabetic agent was discontinued 6 weeks prior to the double-blind period. In one Actos treatment group, patients received an initial dose of 7.5 mg once daily. After four weeks, the dose was increased to 15 mg once daily and after another four weeks, the dose was increased to 30 mg once daily for the remainder of the study (16 weeks). In the second Actos treatment group, patients received an initial dose of 15 mg once daily and were titrated to 30 mg once daily and 45 mg once daily in a similar manner. Treatment with Actos, as described, produced statistically significant improvements in HbA1c and FPG at endpoint compared to placebo (see Table 4).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFor patients who had not been previously treated with antidiabetic medication (24%), mean values at screening were 10.1% for HbA1c and 238 mg/dL for FPG. At baseline, mean HbA1c was 10.2% and mean FPG was 243 mg/dL. Compared with placebo, treatment with Actos titrated to a final dose of 30 and 45 mg resulted in reductions from baseline in mean HbA1c of 2.3% and 2.6% and mean FPG of 63 and 95 mg/dL, respectively. For patients who had been previously treated with antidiabetic medication (76%), this medication was discontinued at screening. Mean values at screening were 9.4% for HbA1c and 216 mg/dL for FPG. At baseline, mean HbA1c was 10.7% and mean FPG was 290 mg/dL. Compared with placebo, treatment with Actos titrated to a final dose of 30 and 45 mg resulted in reductions from baseline in mean HbA1c of 1.3% and 1.4% and mean FPG of 55 and 60 mg/dL, respectively. For many previously treated patients, HbA1c and FPG had not returned to screening levels by the end of the study.
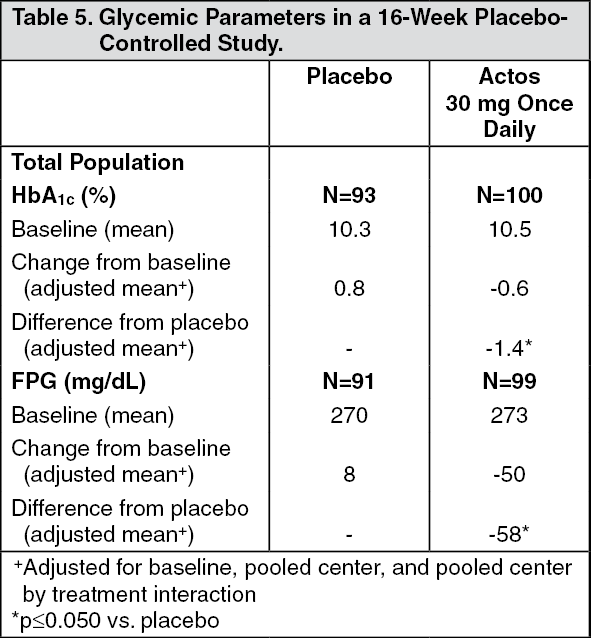
In a 16-week study, 197 patients with type 2 diabetes were randomized to treatment with 30 mg of Actos or placebo once daily. Therapy with any previous antidiabetic agent was discontinued 6 weeks prior to the double-blind period. Treatment with 30 mg of Actos produced statistically significant improvements in HbA1c and FPG at endpoint compared to placebo (see Table 5).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFor patients who had not been previously treated with antidiabetic medication (40%), mean values at screening were 10.3% for HbA1c and 240 mg/dL for FPG. At baseline, mean HbA1c was 10.4% and mean FPG was 254 mg/dL. Compared with placebo, treatment with Actos 30 mg resulted in reductions from baseline in mean HbA1c of 1.0% and mean FPG of 62 mg/dL. For patients who had been previously treated with antidiabetic medication (60%), this medication was discontinued at screening. Mean values at screening were 9.4% for HbA1c and 216 mg/dL for FPG. At baseline, mean HbA1c was 10.6% and mean FPG was 287 mg/dL. Compared with placebo, treatment with Actos 30 mg resulted in reductions from baseline in mean HbA1c of 1.3% and mean FPG of 46 mg/dL. For many previously treated patients, HbA1c and FPG had not returned to screening levels by the end of the study.
Combination Therapy: Three 16-week, randomized, double-blind, placebo-controlled clinical studies and three 24-week randomized, double-blind, dose-controlled clinical studies were conducted to evaluate the effects of Actos on glycemic control in patients with type 2 diabetes who were inadequately controlled (HbA1c ≥8%) despite current therapy with a sulfonylurea, metformin or insulin. Previous diabetes treatment may have been monotherapy or combination therapy.
Actos Plus Sulfonylurea Studies: Two clinical studies were conducted with Actos in combination with a sulfonylurea. Both studies included patients with type 2 diabetes on a sulfonylurea, either alone or in combination with another antidiabetic agent. All other antidiabetic agents were withdrawn prior to starting study treatment. In the first study, 560 patients were randomized to receive 15 mg or 30 mg of Actos or placebo once daily for 16 weeks in addition to their current sulfonylurea regimen. When compared to placebo at Week 16, the addition of Actos to the sulfonylurea significantly reduced the mean HbA1c by 0.9% and 1.3% and mean FPG by 39 mg/dL and 58 mg/dL for the 15 mg and 30 mg doses, respectively.
In the second study, 702 patients were randomized to receive Actos 30 mg or 45 mg once daily for 24 weeks in addition to their current sulfonylurea regimen. The mean reductions from baseline at week 24 in HbA1c were 1.55% and 1.67% for the 30 mg and 45 mg doses, respectively. Mean reductions from baseline in FPG were 51.5 mg/dL and 56.1 mg/dL.
The therapeutic effect of Actos in combination with sulfonylurea was observed in patients regardless of whether the patients were receiving low, medium or high doses of sulfonylurea.
Actos Plus Metformin Studies: Two clinical studies were conducted with Actos in combination with metformin. Both studies included patients with type 2 diabetes on metformin, either alone or in combination with another antidiabetic agent. All other antidiabetic agents were withdrawn prior to starting study treatment. In the first study, 328 patients were randomized to receive either 30 mg of Actos or placebo once daily for 16 weeks in addition to their current metformin regimen. When compared to placebo at Week 16, the addition of Actos to metformin significantly reduced the mean HbA1c by 0.8% and decreased the mean FPG by 38 mg/dL.
In the second study, 827 patients were randomized to receive either 30 or 45 mg of Actos once daily for 24 weeks in addition to their current metformin regimen. The mean reductions from baseline at week 24 in HbA1c were 0.8% and 1.01% for the 30- and 45-mg doses, respectively. Mean reductions from baseline in FPG were 38.2 and 50.7 mg/dL.
The therapeutic effect of Actos in combination with metformin was observed in patients regardless of whether the patients were receiving lower or higher doses of metformin.
Actos Plus Insulin Studies: Two clinical studies were conducted with Actos in combination with insulin. Both studies included patients with type 2 diabetes on insulin, either alone or in combination with another antidiabetic agent. All other antidiabetic agents were withdrawn prior to starting study treatment. In the first study, 566 patients receiving a median of 60.5 units per day of insulin were randomized to receive either 15 mg or 30 mg of Actos or placebo once daily for 16 weeks in addition to their insulin regimen. When compared to placebo at Week 16, the addition of Actos to insulin significantly reduced both HbA1c by 0.7% and 1% and FPG by 35 mg/dL and 49 mg/dL for the 15 mg and 30 mg dose, respectively.
In the second study, 690 patients receiving a median of 60.0 units per day of insulin received either 30 mg or 45 mg of Actos once daily for 24 weeks in addition to their current insulin regimen. The mean reductions from baseline at Week 24 in HbA1c were 1.17% and 1.46% for the 30 mg and 45 mg doses, respectively. Mean reductions from baseline in FPG were 31.9 mg/dL and 45.8 mg/dL. Improved glycemic control was accompanied by significant mean decreases from baseline in insulin dose requirements of 6% and 9.4% per day for the 30 mg and 45 mg dose, respectively.
The therapeutic effect of Actos in combination with insulin was observed in patients regardless of whether the patients were receiving lower or higher doses of insulin.
Pharmacokinetics: Serum concentrations of total pioglitazone (pioglitazone plus active metabolites) remain elevated 24 hours after once daily dosing. Steady-state serum concentrations of both pioglitazone and total pioglitazone are achieved within 7 days. At steady state, two of the pharmacologically active metabolites of pioglitazone, Metabolites III (M-III) and IV (M-IV), reach serum concentrations equal to or greater than pioglitazone. In both healthy volunteers and in patients with type 2 diabetes, pioglitazone comprises approximately 30% to 50% of the peak total pioglitazone serum concentrations and 20% to 25% of the total areas under the serum concentration-time curve (AUC).
Maximum serum concentration (Cmax), AUC and trough serum concentrations (Cmin) for both pioglitazone and total pioglitazone increased proportionally at doses of 15 mg and 30 mg per day. There is a slightly less than proportional increase for pioglitazone and total pioglitazone at a dose of 60 mg per day.
Absorption: Following oral administration, in the fasting state, pioglitazone is first measurable in serum within 30 minutes with peak concentrations observed within 2 hours. Food slightly delays the time to peak serum concentration to 3 to 4 hours, but does not alter the extent of absorption.
Distribution: The mean apparent volume of distribution (Vd/F) of pioglitazone following single-dose administration is 0.63 ± 0.41 (mean ± SD) L/kg of body weight. Pioglitazone is extensively protein bound (>99%) in human serum, principally to serum albumin. Pioglitazone also binds to other serum proteins, but with lower affinity. Metabolites M-III and M-IV also are extensively bound (>98%) to serum albumin.
Metabolism: Pioglitazone is extensively metabolized by hydroxylation and oxidation; the metabolites also partly convert to glucuronide or sulfate conjugates. Metabolites M-II and M-IV (hydroxy derivatives of pioglitazone) and M-III (keto derivative of pioglitazone) are pharmacologically active in animal models of type 2 diabetes. In addition to pioglitazone, M-III and M-IV are the principal drug-related species found in human serum following multiple dosing. At steady-state, in both healthy volunteers and in patients with type 2 diabetes, pioglitazone comprises approximately 30% to 50% of the total peak serum concentrations and 20% to 25% of the total AUC.
In vitro data demonstrate that multiple CYP isoforms are involved in the metabolism of pioglitazone. The cytochrome P450 isoforms involved are CYP2C8 and, to a lesser degree, CYP3A4 with additional contributions from a variety of other isoforms including the mainly extrahepatic CYP1A1. In vivo studies of pioglitazone in combination with P450 inhibitors and substrates have been performed (see Interactions). Urinary 6β-hydroxycortisol/cortisol ratios measured in patients treated with Actos showed that pioglitazone is not a strong CYP3A4 enzyme inducer.
Excretion and Elimination: Following oral administration, approximately 15% to 30% of the pioglitazone dose is recovered in the urine. Renal elimination of pioglitazone is negligible and the drug is excreted primarily as metabolites and their conjugates. It is presumed that most of the oral dose are excreted into the bile either unchanged or as metabolites and eliminated in the feces.
The mean serum half-life of pioglitazone and total pioglitazone ranges from 3 to 7 hours and 16 to 24 hours, respectively. Pioglitazone has an apparent clearance, CL/F, calculated to be 5 to 7 L/hr.
Special Populations: Renal Insufficiency: The serum elimination half-life of pioglitazone, M-III and M-IV remains unchanged in patients with moderate (creatinine clearance 30 to 60 mL/min) to severe (creatinine clearance <30 mL/min) renal impairment when compared to normal subjects. No dose adjustment in patients with renal dysfunction is recommended (see Dosage & Administration).
Hepatic Insufficiency: Compared with normal controls, subjects with impaired hepatic function (Child-Pugh grade B/C) have an approximate 45% reduction in pioglitazone and total pioglitazone mean peak concentrations but no change in the mean AUC values.
Actos therapy should not be initiated if the patients exhibits clinical evidence of active liver disease or serum transaminase levels (ALT) exceed 2.5 times the upper limit of normal (see Hepatic Effects under Precautions).
Elderly: In healthy elderly subjects, peak serum concentrations of pioglitazone and total pioglitazone are not significantly different, but AUC values are slightly higher and the terminal half-life values slightly longer than for younger subjects. These changes were not of a magnitude that would be considered clinically relevant.
Pediatrics: Pharmacokinetic data in the pediatric population are not available.
Gender: The mean Cmax and AUC values were increased 20% to 60% in females. As monotherapy and in combination with sulfonylurea, metformin or insulin, Actos improved glycemic control in both males and females. In controlled clinical trials, hemoglobin A1c (HbA1c) decreases from baseline were generally greater for females than for males (average mean difference in HbA1c 0.5%). Since therapy should be individualized for each patient to achieve glycemic control, no dose adjustment is recommended based on gender alone.
Ethnicity: Pharmacokinetic data among various ethnic groups are not available.
Drug-Drug Interaction: The following drugs were studied in healthy volunteers with a co-administration of Actos 45 mg once daily. Listed as follows are the results: Oral Contraceptives: Co-administration of Actos (45 mg once daily) and an oral contraceptive (1 mg norethindrone plus 0.035 mg ethinyl estradiol once daily) for 21 days, resulted in 11% and 11-14% decrease in ethinyl estradiol AUC (0-24 h) and Cmax, respectively. There were no significant changes in norethindrone AUC (0-24 h) and Cmax. In view of the high variability of ethinyl estradiol pharmacokinetics, the clinical significance of this finding is unknown.
Fexofenadine HCl: Co-administration of Actos for 7 days with 60 mg fexofenadine administered orally twice daily resulted in no significant effect on pioglitazone pharmacokinetics. Actos had no significant effect on fexofenadine pharmacokinetics.
Glipizide: Co-administration of Actos and 5 mg glipizide administered orally once daily for 7 days did not alter the steady-state pharmacokinetics of glipizide.
Digoxin: Co-administration of Actos with 0.25 mg digoxin administered orally once daily for 7 days did not alter the steady-state pharmacokinetics of digoxin.
Warfarin: Co-administration of Actos for 7 days with warfarin did not alter the steady-state pharmacokinetics of warfarin. Actos has no clinically significant effect on prothrombin time when administered to patients receiving chronic warfarin therapy.
Metformin: Co-administration of a single dose of metformin (1000 mg) and Actos after 7 days of Actos did not alter the pharmacokinetics of the single dose of metformin.
Midazolam: Administration of Actos for 15 days followed by a single 7.5 mg dose of midazolam syrup resulted in a 26% reduction in midazolam Cmax and AUC.
Ranitidine HCl: Co-administration of Actos for 7 days with ranitidine administered orally twice daily for either 4 or 7 days resulted in no significant effect on pioglitazone pharmacokinetics. Actos showed no significant effect on ranitidine pharmacokinetics.
Nifedipine ER: Co-administration of Actos for 7 days with 30 mg nifedipine ER administered orally once daily for 4 days to male and female volunteers resulted in least square mean (90% CI) values for unchanged nifedipine of 0.83 (0.73-0.95) for Cmax and 0.88 (0.8-0.96) for AUC. In view of the high variability of nifedipine pharmacokinetics, the clinical significance of this finding is unknown.
Ketoconazole: Co-administration of Actos for 7 days with ketoconazole 200 mg administered twice daily resulted in least square mean (90% CI) values for unchanged pioglitazone of 1.14 (1.06-1.23) for Cmax, 1.34 (1.26-1.41) for AUC and 1.87 (1.71-2.04) for Cmin.
Atorvastatin Calcium: Co-administration of Actos for 7 days with atorvastatin calcium (Lipitor) 80 mg once daily resulted in least square mean (90% CI) values for unchanged pioglitazone of 0.69 (0.57-0.85) for Cmax, 0.76 (0.65-0.88) for AUC and 0.96 (0.87-1.05) for Cmin. For unchanged atorvastatin, the least square mean (90% CI) values were 0.77 (0.66-0.9) for Cmax, 0.86 (0.78-0.94) for AUC and 0.92 (0.82-1.02) for Cmin.
Theophylline: Co-administration of Actos for 7 days with theophylline 400 mg administered twice daily resulted in no change in the pharmacokinetics of either drug.
Cytochrome P450: See Precautions.
Gemfibrozil: Concomitant administration of gemfibrozil (oral 600 mg twice daily), an inhibitor of CYP2C8, with pioglitazone (oral 30 mg) in 10 healthy volunteers pre-treated for 2 days prior with gemfibrozil (oral 600 mg twice daily) resulted in pioglitazone exposure (AUC0-24) being 226% of the pioglitazone exposure in the absence of gemfibrozil (see Interactions).
Rifampicin: Concomitant administration of rifampicin (oral 600 mg once daily), an inducer of CYP2C8 with pioglitazone (oral 30 mg) in 10 healthy volunteers pre-treated for 5 days prior with rifampicin (oral 600 mg once daily) resulted in a decrease in the AUC of pioglitazone by 54% (see Interactions).
Toxicology: Preclinical Safety Data: Carcinogenesis, Mutagenesis, Impairment of Fertility: A two-year carcinogenicity study was conducted in male and female rats at oral doses up to 63 mg/kg (approximately 14 times the maximum recommended human oral dose of 45 mg based on mg/m2). Drug-induced tumors were not observed in any organ except for the urinary bladder. Benign and/or malignant transitional cell neoplasm were observed in male rats at 4 mg/kg/day and above (approximately equal to the maximum recommended human oral dose based on mg/m2). A two-year carcinogenicity study was conducted in male and female mice at oral doses up to 100 mg/kg/day (approximately 11 times the maximum recommended human oral dose based on mg/m2). No drug-induced tumors were observed in any organ.
During prospective evaluation of urinary cytology involving more than 1800 patients receiving Actos in clinical trials up to one year in duration, no new cases of bladder tumors were identified. In two 3-year studies in which pioglitazone was compared to placebo or glyburide, there were 16/3656 (0.44%) reports of bladder cancer in patients taking pioglitazone compared to 5/3679 (0.14%) in patients not taking pioglitazone. After excluding patients in whom exposure to study drug was less than one year at the time of diagnosis of bladder cancer, there were six (0.16%) cases on pioglitazone and two (0.05%) on placebo.
Pioglitazone HCl was not mutagenic in a battery of genetic toxicology studies, including the Ames bacterial assay, a mammalian cell forward gene mutation assay (CHO/HPRT and AS52/XPRT), an in vitro cytogenetics assay using CHL cells, an unscheduled DNA synthesis assay, and an in vivo micronucleus assay.
No adverse effects upon fertility were observed in male and female rats at oral doses up to 40 mg/kg pioglitazone HCl daily prior to and throughout mating and gestation (approximately 9 times the maximum recommended human oral dose based on mg/m2).
Animal Toxicology: Heart enlargement has been observed in mice (100 mg/kg), rats (4 mg/kg and above) and dogs (3 mg/kg) treated orally with pioglitazone HCl (approximately 11, 1 and 2 times the maximum recommended human oral dose for mice, rats and dogs, respectively, based on mg/m2). In a one-year rat study, drug-related early death due to apparent heart dysfunction occurred at an oral dose of 160 mg/kg/day (approximately 35 times the maximum recommended human oral dose based on mg/m2). Heart enlargement was seen in a 13-week study in monkeys at oral doses of 8.9 mg/kg and above (approximately 4 times the maximum recommended human oral dose based on mg/m2), but not in a 52-week study at oral doses up to 32 mg/kg (approximately 13 times the maximum recommended human oral dose based on mg/m2).