


 Sign Out
Sign Out

PHARMACOLOGY: Pharmacodynamics: Mechanism of Action: AFSTYLA (INN: lonoctocog alfa) is a recombinant human protein that replaces the missing coagulation factor VIII needed for effective hemostasis. AFSTYLA is a single polypeptide chain with a truncated B-domain that allows for a covalent bridge to link the factor VIII heavy and light chains. AFSTYLA has demonstrated a higher VWF affinity relative to full-length rFVIII. VWF stabilizes factor VIII and protects it from degradation. Activated AFSTYLA has an amino acid sequence identical to endogenous FVIIIa.
Pharmacodynamic effects: The factor VIII/von Willebrand factor complex consists of two molecules (factor VIII and von Willebrand factor) with different physiological functions. When infused into a haemophiliac patient, factor VIII binds to von Willebrand factor in the patient's circulation. Activated factor VIII acts as a cofactor for activated factor IX, accelerating the conversion of factor X to activated factor X. Activated factor X converts prothrombin into thrombin. Thrombin then converts fibrinogen into fibrin and a clot can be formed.
Haemophilia A is an x-linked hereditary disorder of blood coagulation due to decreased levels of factor VIII and results in profuse bleeding into joints, muscles or internal organs, either spontaneously or as result of accidental or surgical trauma. By replacement therapy the plasma levels of factor VIII are increased, thereby enabling a temporary correction of the factor deficiency and correction of the bleeding tendencies.
Clinical efficacy and safety: Adult and adolescent population 12 - 65 years of age: Study 1001 determined the efficacy and safety in the prevention of bleeding events in prophylaxis, hemostatic efficacy in the control of bleeding events and during perioperative management. The study enrolled 175 previously treated patients (12 to 65 years of age) with severe haemophilia A (1 subject >60 years of age was enrolled) who accumulated a total of 14,306 EDs with rVIII-SingleChain. No patient developed an inhibitor or experienced an anaphylactic reaction.
Prophylaxis: 146 subjects were assigned to a prophylaxis regimen (median ABR, 1.14 (interquartile range: 0.0, 4.2)), 79 (54%) were assigned a 3-times per week regimen and 47 (32%) a 2-times per week regimen. Patients on prophylaxis 2- and 3-times per week were assigned median doses of 35 and 30 IU/kg per injection respectively with a median annual consumption across all prophylaxis regimens of 4,283 IU/kg year.
Treatment of bleeding: Of the 848 bleeding events observed during Study 1001, 93.5% were controlled with 2 or fewer injections. The median dose to treat a bleeding episode was 34.7 IU/kg.
Perioperative management (surgical prophylaxis): A total of 16 major surgical procedures were performed and assessed in 13 subjects in Study 1001. Hemostatic efficacy of rVIII-SingleChain in surgical prophylaxis was rated as excellent or good in all surgeries. No paediatric subjects <18 years of age were included in the surgery population.
Paediatric population <12 years of age: Study 3002 enrolled a total of 84 previously treated patients <12 years of age (35 <6 years of age and 49 6 to <12 years of age). The study participants accumulated a total of 5,239 EDs with rVIII-SingleChain. No patient developed an inhibitor or experienced an anaphylactic reaction.
Individualised prophylaxis: Of the 81 patients on prophylaxis (median ABR 3.69 (interquartile range: 0.00, 7.20)), 43 (53%) were assigned to a 2-times weekly regimen and 25 (31%) to a 3-times per week regimen. Patients on prophylaxis 2- and 3-times per week were assigned median doses of 35 and 32 IU/kg per injection respectively with a median annual consumption across all prophylaxis regimens of 4,109 IU/kg year.
Treatment of bleeding: Of the 347 bleeding events observed during Study 3002, 95.7% were controlled with 2 or fewer injections. The median dose used to treat a bleeding event was 27.6 IU/kg.
Of note, annualized bleeding rate (ABR) is not comparable between different factor concentrates and between different clinical studies.
Paediatric population: The European Medicines Agency has deferred the obligation to submit the results of studies with AFSTYLA in the treatment of hereditary factor VIII deficiency in previously untreated paediatric patients (PUPs) (see Dosage & Administration for information on paediatric use).
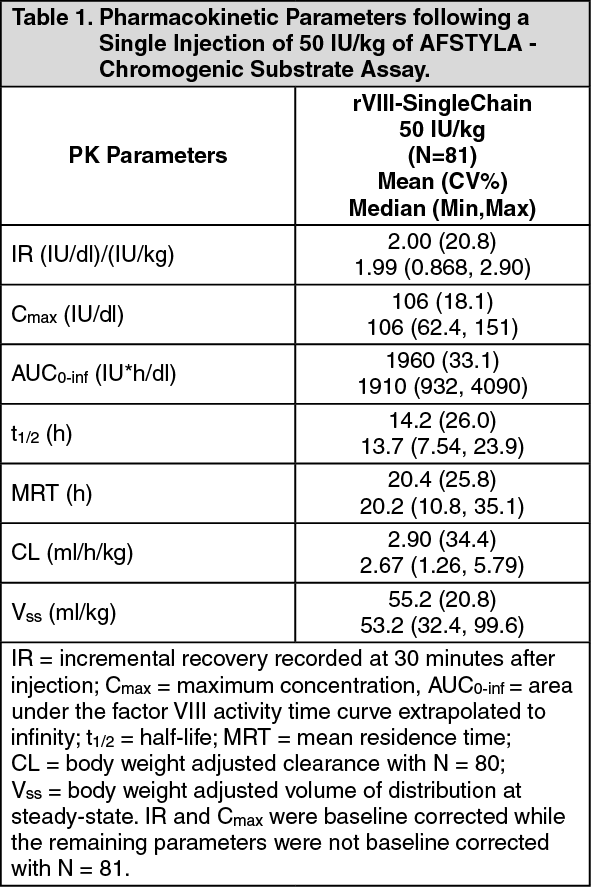
Pharmacokinetics: Adult population: The pharmacokinetics (PK) of AFSTYLA was evaluated in 81 previously treated adult subjects who had been diagnosed with severe haemophilia A with <1% factor VIII and with age from 18-60 years old, following an intravenous injection of 50 IU/kg.
The PK parameters were based on plasma factor VIII activity measured by the chromogenic substrate assay (for discrepancy in the factor VIII activity determined with one-stage clotting assay, please see Dosage & Administration). The PK profile obtained 3 to 6 months after the initial PK assessment was comparable with the PK profile obtained after the first dose. (See Table 1.)
 Click on icon to see table/diagram/image
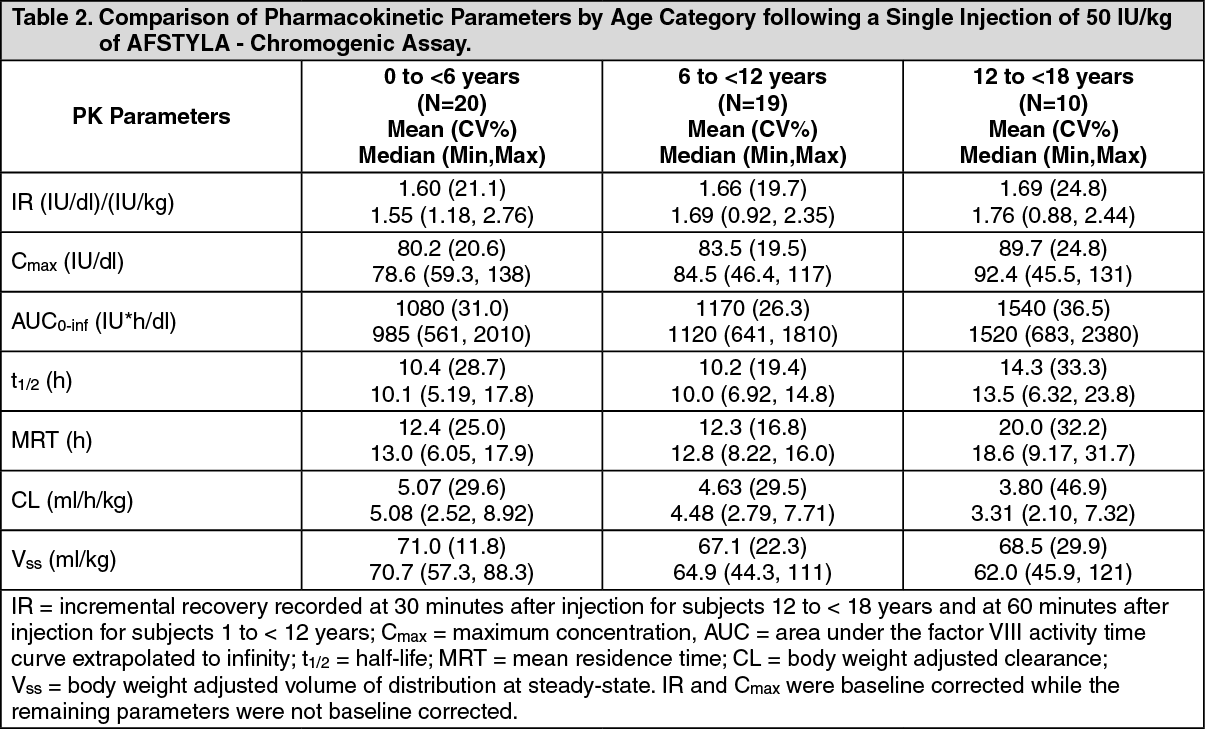
Click on icon to see table/diagram/imagePaediatric population: The pharmacokinetics (PK) of AFSTYLA were evaluated in 10 previously treated adolescents (12 to <18 years of age) and 39 previously treated children (0 to <12 years of age) following an intravenous injection of a single dose of 50 IU/kg. All patients had been diagnosed with severe haemophilia A with <1% factor VIII.
The PK parameters were based on plasma factor VIII activity measured by the chromogenic substrate assay (for discrepancy in the factor VIII activity determined with one-stage clotting assay, please see Dosage & Administration). (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageToxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, single and repeated dose toxicity studies, local tolerability and thrombogenicity assessments.