


 Sign Out
Sign Out

Antihemophilic Factor (AHF) potency (Factor VIII:C activity) is expressed nominally in International Units (IU) on the product label. Additionally, each vial of Alphanate also contains specific von Willebrand Factor:Ristocetin Cofactor (VWF:RCo) activity in IU for the treatment of VWD.
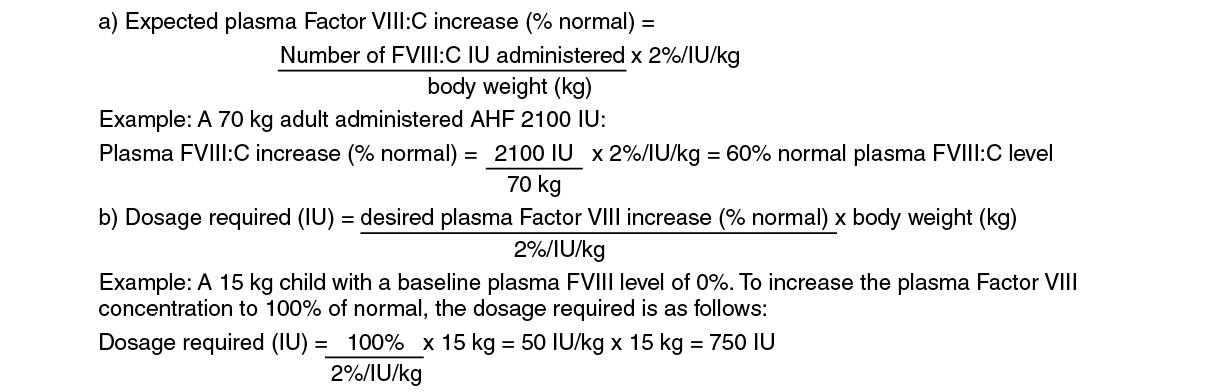
Hemophilia A: Dosing requirements and frequency of dosing is calculated on the basis of an expected initial response of 2% of normal FVIII:C increase per FVIII:C IU/kg body weight administered. The in vivo increase in plasma Factor VIII can therefore be estimated by multiplying the dose of AHF per kilogram of body weight (FVIII:C IU/kg) by 2%. Thus, an administered AHF dose of 50 IU/kg will be expected to increase the circulating Factor VIII level by 100% of normal (100 IU/dL). The following formulas and examples illustrate these principles: See equation.
 Click on icon to see table/diagram/image
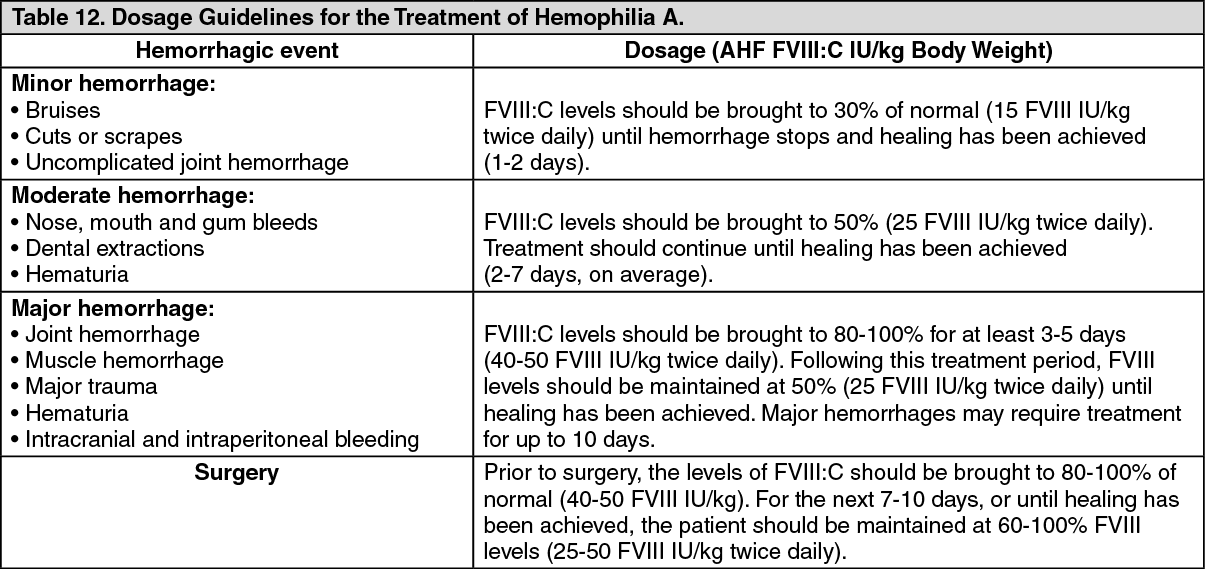
Click on icon to see table/diagram/imageThe following dosages are presented as general guidance as shown in Table 12. It should be emphasized that the dosage of Alphanate required for hemostasis must be individualized according to the needs of the patient, the severity of the deficiency, the severity of the hemorrhage, the presence of inhibitors, and the FVIII level desired. Adequacy of treatment must be judged by the clinical effects and situation and thus, the dosage may vary with individual cases. (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDosing requirements and frequency of dosing is calculated on the basis of an expected initial response of 2% FVIII:C increase per FVIII:C IU/kg body weight (i.e., 2% per IU/kg) and an average half-life for FVIII:C of 12 hours. If dosing studies have determined that a particular patient exhibits a lower than expected response, the dose should be adjusted accordingly. Failure to achieve the expected plasma FVIII:C level or to control bleeding after an appropriately calculated dosage may be indicative of the development of an inhibitor (an antibody to FVIII:C). Its presence should be documented and the inhibitor level quantitated by appropriate laboratory procedures. Treatment with AHF in such cases must be individualized.
Plasma factor VIII levels should be monitored periodically to evaluate individual patient response to the dosage regimen.
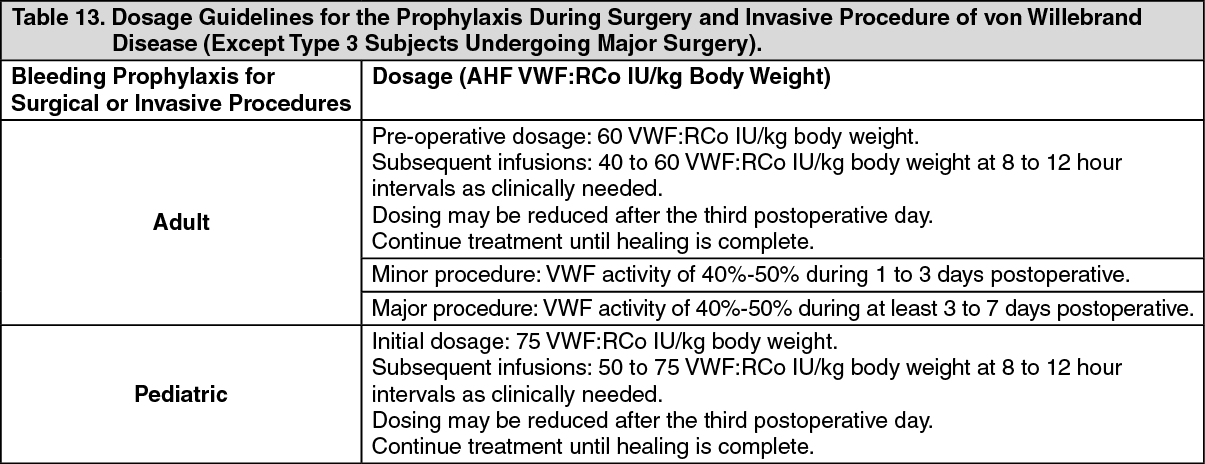
Von Willebrand Disease: Table 13 provides dosing guidelines for pediatric and adult patients with von Willebrand Disease.
The amount of specific VWF:RCo and nominal Factor VIII contained in each vial of Alphanate is indicated on the vial's label. The ratio of VWF:RCo to Factor VIII in Alphanate varies by lot, so dosage should be re-evaluated whenever lot selection is changed. (See Table 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image