Amlodipine besylate, benazepril HCl.
Each tablet contains amlodipine besylate 5 mg and benazepril HCl 10 mg.
Amlodipine besylate is a white to mildly yellow crystalline powder that is mildly soluble in water and barely soluble in ethanol. It is a besylate salt of amlodipine and is a type of calcium-channel blocker. Its chemical name is (R,S)3-ethyl-5-methyl-2-(2-aminoethoxymethyl)-4-(2-chlorophenyl)-1,4-dihydro-6-methyl-3,5-pyridinedicarboxylate benzenesulfonate. Its chemical formula is C20H25CIN2O5·C6H6O3S and has a molecular weight of 567.1.
Benazepril HCl is a white to grayish-white crystalline powder, which is soluble in water (>100 mg/mL), ethanol and methanol. Its active metabolite, benazeprilat, is a non-hydrogen sulfate angiotensin-converting enzyme (ACE) inhibitor. Its chemical name is 3-[[1(ethoxycarbonyl)-3-phenyl-(1S)-propyl]amino]-2,3,4,5-tetrahydro-2-oxo-1H-1-(3S)-benzazepine-1-acetic acid monohydrochloride. Its chemical formula is C24H28N2O5·HCl, with a molecular weight of 460.96.
Pharmacology: Pharmacodynamics: When given single-dose or multidose of benazepril ≥10 mg for 24 hrs, 80-90% suppression of ACE activity can be reached. After giving 10 mg for 4 hrs, the vasopressor response of extrinsic angiotensin I can be suppressed by 60-90%. When benazepril is given to mild to moderate hypertensive patients, blood pressure is lowered when measuring blood pressure in both seated and standing postures, and compensatory tachycardia will not occur. Patients with a loss of salt or body fluids might experience postural hypotension, but this condition is uncommon (see Hypotension under Warnings). For patients with high or low salt intake, no significant difference is found in the antihypertensive effects of benazepril. In healthy subjects, single-dose of benazepril will cause increase in renal blood flow, but the glomerular filtration rate is unaffected.
When giving antihypertensive patients therapeutic dosage of amlodipine, vascular dilation results. Both recumbent and standing blood pressure may be reduced and long-term use does not result in tachycardia or significant changes in plasma catecholamine concentration. Correlation between plasma concentration and efficacy may be observed in both young and old patients. Like other calcium-ion blockers, when treating patients with normal ventricular functions with amlodipine, hematodynamic measurements of heart functioning during rest and exercise indicate mild increases, but no significant effects on dP/dt, left ventricular diastolic pressure or body fluids are found. In hemodynamic studies, amlodipine with a dosage within the therapeutic limit was given to humans or animals, even with simultaneous administration of β-blockers, amlodipine will not produce negative muscular constriction. In both animals and humans, amlodipine will not affect function of the S-A node and atrioventricular conduction. In clinical trials, when patients with hypertension or angina were given amlodipine and β-blockers, no adverse reactions were observed in the electrocardiograms.
In 6 double-blind, placebo-controlled clinical studies examining >950 patients that received the amlodipine and benazepril formula, found that blood pressure can be lowered with 1 hr after taking Amtrel. The lowest point can be achieved within 2-8 hrs. A single-dose of Amtrel can maintain the blood-pressure lowering effects for 24 hrs. When taking benazepril 10-20 mg combined with amlodipine 2.5-10 mg, seated blood pressure (systolic/diastolic) can be reduce by 10-25/6-13 mmHg after 24 hrs.
The combination therapy can be effective for both Blacks and non-Blacks. In non-Blacks, both ingredients may lower blood pressure. In Blacks, however, the major antihypertensive effects come from amlodipine. In a placebo-controlled clinical trial, comparing the blood-pressure lowering effects of the combination formula (amlodipine and benazepril) and individual ingredient given separately, with non-Blacks as the subjects, results indicated that the formulated agent had additive antihypertensive effects, while synergistic effects were observed in few patients.
With long-term use, the maximum reduction of blood pressure usually occurs 1-2 weeks after Amtrel is administered. The blood pressure reduction can be maintained for at least 1 year. Sudden stoppage of Amtrel will not result in rapid increase of blood pressure.
Mechanism of Action: Contraction of the vascular smooth muscle and the myocardium requires specific ionic channels that transport calcium ions into the cells. Amlodipine is a calcium-ion inhibitor, which suppresses calcium ion from moving through the cell membrane into vascular smooth muscle or myocardium. However, this suppression is selective and is more effective with the smooth muscle than when compared to myocardium. Also, serum calcium-ion concentration will not be affected by amlodipine. In normal physiological pH, amlodipine is an ionic metabolite (pKa=8.6). Its binding and removal rate with calcium ion-channel receptors are gradual. Thus, its exerted effects are also gradual. Amlodipine is a peripheral vascular dilator and can directly act on vascular smooth muscles to cause lowered peripheral vascular resistance and reduced blood pressure.
In humans and animals, benazepril and benazeprilat can suppress ACE, and ACE can convert angiotensin I to angiotensin II, which is a vascular constricting substance. Angiotensin II can stimulate the adrenal cortex to secrete aldosterone. Suppression of ACE can reduce the plasma concentration of angiotensin II, causing reduced vasoconstrictive activity and decreased secretion of aldosterone. The latter substance can cause a microscopic increase of potassium concentration in the blood. After 56 weeks of treatment involving benazepril and amlodipine in hypertensive patients, the blood potassium concentration increased to 0.2 mEq/L. Removal of the negative feedback of angiotensin on renin may cause plasma renin to increase. In an animal study, benazepril had no suppressive effects on the vasopressor response of angiotensin II. Also, it did not affect the hemodynamics of neurotransmitters eg, acetylcholine, epinephrine or norepinephrine. The general belief of the antihypertensive mechanism of benazepril is the suppression of the renin-angiotensin-aldosterone system. Therefore, even in hypertensive patients with low renin level, benazepril still can reduce their blood pressure.
Pharmacokinetics: According to international clinical studies, the rate of absorption of benazepril and amlodipine formula in the body is not significantly different than taking them individually. In terms of individual administration, absorption will not be affected by food in the gastrointestinal tract. There are currently no reports of the effects of food on absorption of the formula. After taking Amtrel, plasma benazepril concentration peaks in 0.5-2 hrs and cleavage of the ester group (mainly occurs in the liver) occurs to be converted to its active metabolite (benazeprilat). The plasma concentration of the metabolite benazeprilat reaches its peak level in 1.5-4 hrs. Level of absorption for benazepril is at least 37%. The plasma concentration of amlodipine peaks in 6-12 hrs and its level of absorption is approximately 64-90%.
The volume distribution of amlodipine and benazeprilat is 21 L/kg and 0.7 L/kg, respectively. In the circulation, about 93% of amlodipine are bound to plasma proteins. The binding ratio of benazeprilat is slightly higher than amlodipine. In vitro studies found that the protein-binding level of benazeprilat was not affected by concentration, age and liver function.
Suppression of ACE activity is much higher in benazeprilat compared to benazepril and almost all benazepril are metabolized to become benazeprilat. Only small amounts of the original substance are found in the excreted urine; about 20% of benazeprilat are found, 8% are benazeprilat glucuronide and 4% are benazepril glucuronide. Amlodipine is mostly metabolized in the liver, and 10 % of the original structure and 60% of its metabolites are found in the urine. In patients with liver dysfunction, due to lowered clearance rate of amlodipine, the area under the plasma concentration-time curve (AUC) is increased by about 40-60%. Thus, dosage should be appropriately adjusted (see Dosage & Administration). Patients with renal dysfunction will not affect the pharmacokinetics of amlodipine.
The half-life for effective removal of benazeprilat and amlodipine is appproximately 10-11 hrs and 2 days, respectively. The 2 drugs can reach stable blood concentrations with 1 administration of Amtrel per day for 1 week. Removal of benzaprilat from the plasma is mainly through the kidneys. In normal individuals, however, bile removal accounts for 11-12% of total elimination of benazepril. For patients with renal dysfunction [creatinine clearance (CrCl) <30 mL], time for benazeprilat to reach its peak concentration and time to reach stability may both be prolonged (see Dosage & Administration). For patients with liver dysfunction, the pharmacokinetics of benazeprilat remains unchanged. Age will not affect the pharmacokinetics of benazepril and benazeprilat, while the removal rate of amlodipine will be lower in the elderly, causing peak blood concentration, half-life of removal and AUC to increase approximately 35-70%. Therefore, in the elderly, the dosage might need to be adjusted.
The effect dosage of amlodipine for the treatment of hypertension is 2.5-10 mg daily, while the daily dosage for benazepril is 10-80 mg. In a clinical trial involving a combined treatment of amlodipine 2.5-5 mg and benazepril 10-20 mg, the blood pressure reducing effects of amlodipine increased with increased dosage of amlodipine in all patient groups. In non-Black people, the blood-pressure lowering effects also increased with increased benazepril dosage. In all patient groups, edema caused by amlodipine was reduced.
Risks from benazepril are usually not associated with dosage. However, some risks of amlodipine are related with dosage (peripheral vascular edema), while others are not. Dosage-related risks, however, are more commonly seen. When benazepril is combined with amlodipine, the rate of edema will reduce. Thus, although amlodipine combined with benazepril contain side effects of both that are unrelated to dosage, the rate of edema is lower compared to using amlodipine alone.
In order to reduce risks carried with using the combined formula, it is only recommended in the following situations and Amtrel should not be used in the initial treatment of hypertension: When a single antihypertensive drug is ineffective and when amlodipine treatment does not reach the expected effects and no edema occurs.
Therapy Replacement: For convenience, patients taking amlodipine and benazepril in combination but in separate tablets may now take Amtrel alone, with the identical dosage as before.
Patients with Metabolic Dysfunction: When patients with a CrCl >30 mL/min/1.73 m2 (similar to serum creatinine concentration ≤3 mg/dL or 265 mM/L), dosage adjustment is not needed.
Patient with Severe Renal Dysfunction: The recommended initial dosage for benazepril is 5 mg and Amtrel is not recommended.
Children, Elderly, Weak and Patients with Liver Dysfunction: The recommended initial dosage for amlodipine, whether given alone or in combination, is 2.5 mg.
There are only a few case reports of amlodipine overdose. One (1) case reported no symptoms after taking 250 mg.
There are currently no reports on overdose of combined amlodipine and benazepril. In a few case reports of overdose involving benazepril and other ACE inhibitor drugs, no deaths occurred.
Hypersensitivity to benazepril, ACE inhibitors or amlodipine are prohibited from using Amtrel.
Anaphylactoid Reactions: ACE inhibitors can affect the metabolism of eicosanoid and polypeptides (including intrinsic bradykinin). When patients receive ACE inhibitor therapy, they might experience mild to severe side effects. These side effects usually occur in the 1st few doses. However, some do not experience side effects until after several months of treatment.
Vascular Edema: ACE inhibitors use might occasionally cause vascular edema, including the face, limbs, lips, tongue, glottis and throat. In a clinical trial performed in the United States, it was found that cases in the placebo control group did not develop symptoms of vascular edema, while 0.5% of patients receiving benazepril experienced vascular edema. Vascular edema related to the larynx can be life-threatening; if laryngeal stridor or vascular edema is observed in the face, tongue or glottis, Amtrel should be stopped and the patient should seek appropriate medical attention. When vascular edema occurs in the tongue, glottis or larynx and causing possible obstruction of the respiratory tract, proper treatment should be given immediately eg, SC epinephrine injection 1:1000 (0.3-0.5 mL) (see Adverse Reactions).
Antiallergy Therapy for Anaphylactoid Reactions: Two (2) patients experienced continuous life-threatening anaphylactoid reactions after receiving ACE inhibitor treatment and received antiallergic therapy involving hymenoptera venom.
Allergic Reaction Associated with Contact with Hemodialysis Membrane: Cases of allergy-like reactions were reported with the use of high-flux membranes in dialysis patients taking ACE inhibitors. Allergy-like reactions had occurred in patients who received low-density lipoprotein plasmapheresis therapy by absorbing dextran sulfate.
Increased Angina and/or Myocardial Infarction (MI): When patients with severe obstructive coronary arterial disease start taking calcium-ion blocker or increased its dosage, the frequency, duration and/or severity of angina and/or MI may increase. However, the incident rate of this is low and its mechanism is unclear.
Hypotension: Amtrel can cause generalized hypotension. Like other ACE inhibitors, benazepril has an extremely low chance of causing generalized hypotension in patients with simple hypertension. Generalized hypotension is more easily developed in patients with long-term diuretic use, patients that control dietary salt-intake, dialysis and who lose salt or body fluid due to diarrhea or vomiting. Before using Amtrel, lost body fluids and salt should be replenished first.
Due to the gradual vasodilating effect of amlodipine, the rate of developing acute hypotension is extremely rare with oral amlodipine use. However, when Amtrel is used concurrently with other peripheral vasodilators special caution should be taken, especially in patients with aortic stenosis.
Regardless of the relation with renal dysfunction, ACE inhibitors treatment in patients with congestive heart failure can cause excessive hypotension and subsequently result in oliguria, azotemia and acute renal failure or death (extremely rare). This type of patients should only receive Amtrel under strict medical monitoring. Careful follow-up should be performed when increasing the dosage of benazepril, or adding or increasing the dosage of diuretics. When hypotension occurs, patient should be recumbent. When necessary, IV transfusion of saline solution can be provided. Once blood pressure and body fluids are restored, Amtrel may be continued.
Neutropenia/Agranulocytopenia: Data have shown that usage of another ACE inhibitor, captopril, may result in agranulocytopenia and bone marrow suppression. The incidence is lower in patients with simple hypertension (<1/10,000), while the incidence is higher in patients with renal dysfunction (>1/10,000), especially in patients with collagen vascular disease eg, systemic lupus erythematosus (SLE) or scleroderma. Clinical trial data involving benazepril are insufficient in demonstrating that it will not cause agranulocytopenia similar to captopril. Thus, in patients with collagen vascular disease, the leukocyte count should be monitored, especially when the disease is related with renal dysfunction.
Fetus/Newborn Disease Incidence and Death Rate: In studies from around the world, many cases have demonstrated that ACE inhibitors use in pregnant women can cause disease or death of the fetus. Hence, when a woman determines to be pregnant, the patient should immediately stop taking Amtrel. ACE inhibitors use in the 2nd or 3rd trimester can result in damage to the fetus or newborn, including hypotension, improper development of the skull, anuria, reversible or irreversible renal failure and death. Also, reduced renal function of the fetus can result in nonproduction of amniotic fluid. Oligohydramnios is related to limb contracture and deformity, facial deformity and improper lung development of a fetus. Delayed uterus growth and permanent arterial fistula have been reported, although it is unclear whether they are caused by ACE inhibitors use.
At the present, there are no clinical trials involving Amtrel in pregnant women.
Liver Failure: Very few liver failures are related with ACE inhibitors. Symptoms can start with cholestic jaundice and worsen to fibrotic liver necrosis and sometimes even death. The mechanism for these symptoms is unclear. When patients receiving ACE inhibitors display jaundice or significant increase in liver enzymes, ACE inhibitors should be stopped and patients should receive appropriate medical care.
General: Patients with Renal Dysfunction: Patients with severe renal diseases should take Amtrel with caution. Patients with high susceptibility can expect that, when the renin-angiotensin-aldosterone system is suppressed by benazepril, corresponding changes in renal function can occur. Patients with severe congestive heart failure rely on operation of the renin-angiotensin-aldosterone system, so using ACE inihibitors (including benazepril) for treatment can cause oliguria, azotemia and acute renal failure or death. In a few reports studying patients with unilateral or bilateral renal stenosis, the results indicated that benazepril therapy increased blood urea nitrogen (BUN) and serum creatinine concentration. However, if benazepril was stopped or combined with diuretics, BUN and serum creatinine concentration can be restored to normal. If patients in this category were to receive treatment with Amtrel, intensive monitoring of renal function should be performed a few weeks before treatment starts. Hypertensive patients without significant symptoms of renal vascular disease can experience increased BUN and serum creatinine concentration after receiving benazepril therapy, but the symptoms are mild and temporary, and this is especially true when benazepril is given along with diuretics. Assessments of hypertensive patients should include renal function assessment (see Dosage & Administration).
Hyperkalemia: In a placebo-controlled clinical study performed in the United States, it was found that about 1.5% of patients that received a similar combination formula experienced hyperkalemia, but the increased potassium ion concentration in the serum can be reversed. Risk factors for developing hyperkalemia include: Renal dysfunction, diabetes and concurrent use of potassium-preserving diuretics, potassium supplements or salts containing potassium ion.
Congestive Heart Failure (CHF): Hemodynamic and clinical studies performed in the United States on New York Heart Association (NYHA) class II-III, CHF patients all indicated that amlodipine did not cause clinical worsening as measured by exercise tolerance tests, left ventricular rejection or symptomatic changes clinically. Overall, patients with CHF should take all calcium-ion blockers with caution.
Liver Failure: In patients with liver dysfunction as a result of liver cirrhosis, benazeprilat concentration in the body will not change. However, amlodipine is metabolized by the liver and its plasma half-life is as long as 56 hrs in patients with liver dysfunction. Therefore, extreme caution should be taken when patients with severe liver damage use Amtrel (see Warnings).
Cough: ACE inhibitors use can cause breakdown of intrinsic bradykinins, so persistent dry coughs can result. After amtrel is discontinued, however, the condition may be reversed. During the diagnostic process, the physician should distinguish between coughs stimulated by ACE inhibitors and general coughs.
Surgery/Anesthesia: When a patient uses agents that cause hypotension during surgery or under anesthesia, benazepril will block the synthesis of angiotensin II, causing compensatory release of renins. Hypotension caused by this mechanism may be recovered by supplementing body fluids.
Amtrel should not be used in the initial treatment of hypertension (see Dosage & Administration) and use only with a physician's prescription.
When using Amtrel, it should be noted that ACE inhibitors may cause agranulocytosis, especially in patients with renal dysfunction or collagen vascular diseas. Also, there is insuffivient evidence to demonstrate that similar risks will not occur with benazepril use (see Neutrophil/Agranulocyte under Warnings).
Carcinogenesis, Mutagenesis, Impairment of Fertility: In Study with Benazepril: No carcinogenicity was found when giving rats and mice benazepril 150 mg/kg/day for 104 weeks. With weight as the basis of calculation, this dosage exceeds 100 times the maximum recommended dosage for humans. When calculated with surface area of the body as the basis, this dosage is 9-18 times the maximum recommended dosage for humans. The bacterial Ames test, mutagenicity test of in vitro mammalian cell culture and tests of abnormal cell nucleus all showed no mutations. Within the dosage of 50-500 mg/kg/day (with weight as the basis of calculation, it is 38-375 times the maximum recommended dosage for humans; using surface area as the basis of calculation, it is 6-61 times the maximum recommended dosage for humans), benazepril does not cause adverse effects in male and female mice.
In Study with Amlodipine: Using the dosage of 0.5, 1.25 and 2.5 mg/kg/day, amlodipine was given to rodents daily for 2 years. Results revealed no risk of carcinogenicity. For mice (not applicable to rats), the maximum dosage is similar to the maximally tolerated dosage. Using surface area as the basis of calculation (mg/m2), the dosage given to mice is close to the maximum clinically recommended dosage. The same dosage given to rats is similar to twice the maximum recommended dosage clinically. Mutagenicity studies of amlodipine have indicated no drug-related effects in both the gene and chromosome level. When amlodipine 10 mg/kg/day is given to mice [calculated with surface area as the basis (mg/m2)], it is similar to 8 times the maximum recommended dosage for a 50 kg human), fertility is unaffected (the drug is given 64 days in male mice before mating and 14 days in female mice before mating).
When benazepril:amlodipine are given concurrently with the dosage of 15:7.5 mg/kg/day, no adverse effects are found in male and female mice before mating and during pregnancy.
Use in pregnancy: Pregnancy Category C (1st Trimester) and D (2nd and 3rd Trimesters): See Fetus/Newborn Disease Incidence and Death Rate under Warnings.
Use in lactation: Only minute amounts of benazepril and benazeprilat are secreted in the breast milk of breastfeeding women. Therefore, if the newborn consumes breast milk, <0.1% of the dosage received by the mother will be absorbed by the newborn.
It is currently unclear whether amlodipine may be found in the breast milk. Thus, it is recommended that when taking Amtrel for treatment, breastfeeding should stop.
Use in children: Safety and efficacy of Amtrel in children have yet to be established.
Use in the elderly: In clinical studies published in the United States, 19% were patients ≥65 years and 2% were patients ≥75 years; no differences have been reported in terms of safety and efficacy of Amtrel between young and elderly patients.
Use in pregnancy: Pregnancy Category C (1st Trimester) and D (2nd and 3rd Trimesters): Fetus/Newborn Disease Incidence and Death Rate: In studies from around the world, many cases have demonstrated that ACE inhibitors use in pregnant women can cause disease or death of the fetus. Hence, when a woman determines to be pregnant, the patient should immediately stop taking Amtrel. ACE inhibitors use in the 2nd or 3rd trimester can result in damage to the fetus or newborn, including hypotension, improper development of the skull, anuria, reversible or irreversible renal failure and death. Also, reduced renal function of the fetus can result in nonproduction of amniotic fluid. Oligohydramnios is related to limb contracture and deformity, facial deformity and improper lung development of a fetus. Delayed uterus growth and permanent arterial fistula have been reported, although it is unclear whether they are caused by ACE inhibitors use.
At the present, there are no clinical trials involving Amtrel in pregnant women.
Use in lactation: Only minute amounts of benazepril and benazeprilat are secreted in the breast milk of breastfeeding women. Therefore, if the newborn consumes breast milk, <0.1% of the dosage received by the mother will be absorbed by the newborn.
It is currently unclear whether amlodipine may be found in the breast milk. Thus, it is recommended that when taking Amtrel for treatment, breastfeeding should stop.
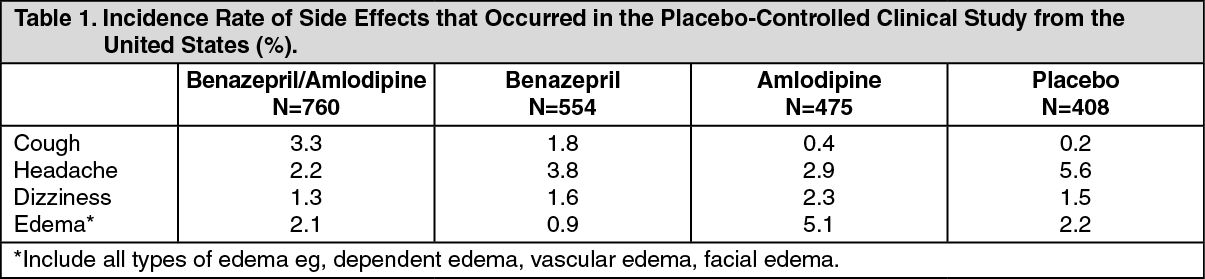
International studies have revealed that, in over 1600 hypertensive patients >500 received treatment with the formula of the same ingredients for at least 6 months and >400 received treatment for >1 year. Reports on side effects were mild and temporary, and these side effects had no correlation with age, gender, race and treatment duration. Approximately 4% of patients that received the combined formula and 3% of patients that received placebo stopped treatment due to side effects. Most common side effects were coughs and edema*. The following table indicates the more common side effects associated with the formula with the same ingredients as reported in the placebo-controlled clinical study from the United States. See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Patients that received only amlodipine had a higher rate of edema compared to patients taking the combination therapy and the difference has reached statistical significance. Edema and other side effects are related with the dosage of amlodipine, and are more common in females. The addition of benazepril decreased the rate of side effects and was uncorrelated with race (within the range of tested dosage). See Table 2.
Click on icon to see table/diagram/image
The following list depicts the possible side effects associated with the combination formula reported by the placebo-controlled clinical trials involving the formula with identical ingredients performed in the United States and side effects reported after Amtrel has been marketed:
Vascular Edema: Including the lips or face (see Vascular Edema under Warnings).
Systemic: Weakness, fatigue.
Central and Peripheral Nervous System: Insomnia, anxiety, shaking, decreased libido.
Skin: Facial hot flushes, rashes, skin nodules, dermatitis.
Gastrointestinal System: Dry mouth, nausea, abdominal pain, constipation, diarrhea, indigestion, esophagitis.
Metabolic and Nutrition: Hypokalemia.
Musculoskeletal System: Back pain, musculoskeletal pain, spasm.
Respiratory System: Laryngitis.
Urinary and Reproductive System: Impotence, frequent urination.
Other rare adverse effects not necessarily associated with Amtrel include chest pain, premature ventricular contraction, gout, neuritis, tinnitus and alopecia.
Fetus/Newborn Disease Incidence and Death Rate: See Warnings.
Diuretics: If a patient uses Amtrel and diuretics concurrently, extremely low blood pressure usually occurs in the initial stage of treatment. Patients taking Amtrel can stop using the diuretics or increase salt intake before taking Amtrel to reduce the chance of developing hypotension.
Potassium Supplements and Potassium-Preserving Diuretics: Benazepril can reduce loss from thiazide diuretics. Potassium-preserving diuretics (spironolactone, amiloride, triamterene, etc) or potassium supplements can increase risks of hyperkalemia. If this type of drug is used in combination, careful and frequent monitoring of the serum potassium concentration of the patient should be performed.
Lithium Agent: There are reports of increased blood lithium concentration and lithium toxicity when a patient takes lithium agent in the duration of ACE inhibitors use. When the concurrent use of lithium is necessary, caution should be taken and it is recommended to monitor for serum lithium concentration.
Others: When benazepril is concurrently taken with oral anticoagulants, β-adrenergic inhibitors, calcium-ion blockers, cimetidine, diuretics, digoxin, hydralazine or naproxen, no clinical evidences of major side effects from drug interactions have been reported.
In clinical trials, amlodipine can be safely used with thiazide diuretics, β-blockers, ACE inhibitors, long-acting nitrates, sublingual trinitroglycerin, digoxin, warfarin, nonsteroidal anti-inflammatory drugs, antibiotics and oral blood sugar reducing agents.
C09BB13 - benazepril and amlodipine ; Belongs to the class of ACE inhibitors and calcium channel blockers. Used in the treatment of cardiovascular diseases.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image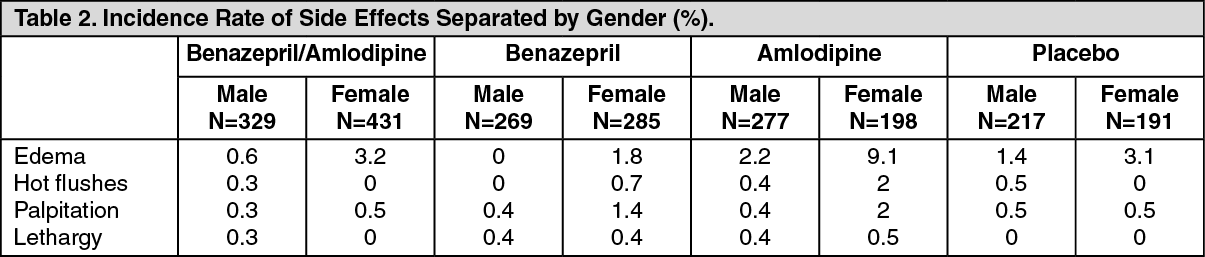 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out