Adverse reactions to enalapril usually are mild and transient. Enalapril usually is well tolerated.
Nervous System Effects: Headache and dizziness occur in about 5% of patients receiving enalapril alone for hypertension.
Gl Effects: Diarrhea and nausea occur in about 1-2% of patients with hypertension receiving enalapril. Abdominal pain, vomiting, stomatitis, and dyspepsia occur in 0.5-2% of patients receiving enalapril.
Cardiovascular Effects: The most frequent adverse effect is hypotension which occurs in about 1-2% of patients with hypertension and in about 5-7% of those with congestive heart failure.
Renal Effects: Deterioration in renal function, manifested as transient increases in BUN and serum creatinine concentrations, has occurred in about 20% of patients with renovascular hypertension, especially those with renal-artery stenosis. This effect was usually reversible following discontinuance of enalapril and/or diuretic therapy.
Dermatologic and Sensitivity Reactions: The most frequent adverse effect is rash, (1.5%) and is usually maculopapular.
Pruritus, (0.5-2%) and alopecia (0.5-1%).
Angioedema of the face, lips, tongue, larynx, glottis, or extremities has occurred in patients receiving ACE inhibitor therapy, including enalapril. (See Contraindications.)
Effects on Potassium: Although small increases (i.e., by an average of 0.2 mEq/L) in serum potassium concentrations frequently occur in patients receiving enalapril without a thiazide diuretic, hyperkalemia (i.e., increases to greater than 5.7 mEq/L) occurs in approximately 1 or 4% of patients with hypertension or congestive heart failure, respectively, receiving the drug.
Respiratory Effects: Cough has been reported in 1.3% and 2 % of patients receiving enalapril for hypertension and CHF respectively, and is reversible following discontinuance of the drug.
Other Adverse Effects: such as muscle cramps, pancreatitis, hepatitis or cholestatic jaundice, hepatic failure and impotence.


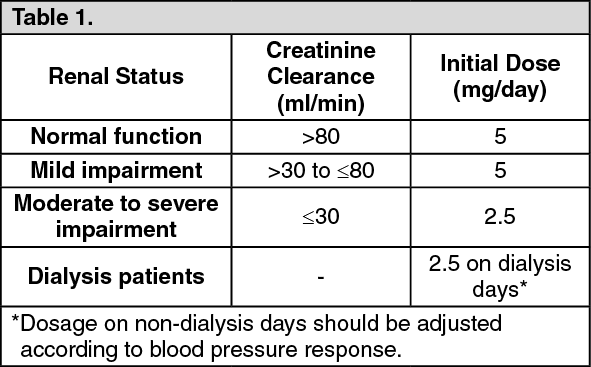 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image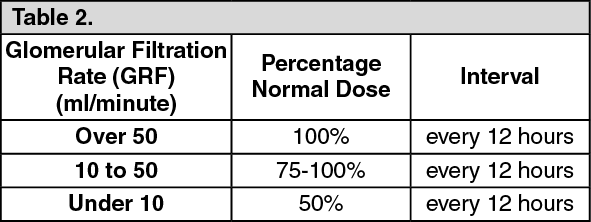 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out