Pharmacotherapeutical group: Platelet aggregation inhibitors excluding heparin.
ATC Code: B01AC/04.
Pharmacology: Pharmacodynamics: Mechanism of Action: Clopidogrel is a prodrug that is metabolized to the active form, (thiol derivative) that inhibits platelet aggregation by selectively and irreversibly binding to the adenosine diphosphate (ADP) P2Y12 receptor on platelets. This binding prevents activation of the ADP-mediated glycoprotein GPIIb/IIIa complex, which is necessary for platelet aggregation. This action is irreversible for the remainder of the platelet lifespan (7 to 10 days).
Pharmacodynamic Properties: Dose dependent inhibition of platelet aggregation can be seen 2 hours after single oral doses of clopidogrel. Repeated doses of 75 mg per day inhibit ADP-induced platelet aggregation from the first day, and inhibition reaches steady state between Day 3 and Day 7. At steady state, the average inhibition level observed with a dose of 75 mg clopidogrel per day was between 40% and 60%. Platelet aggregation and bleeding time gradually returned to baseline values after treatment was discontinued, generally in about 5 days.
Clinical Studies: The clinical evidence for the safety and efficacy in preventing vascular ischemic events has been evaluated in two randomized, double-blind, placebo-controlled trials: the CAPRIE study (Clopidogrel vs Aspirin in Patients at Risk of Ischemic Events), a comparison of clopidogrel to aspirin, and the CURE study (Clopidogrel in Unstable Angina to Prevent Recurrent Ischemic Events), a comparison of clopidogrel to placebo, both given in combination with aspirin and other standard therapy.
The CAPRIE trial was a 19,185 patients, randomized, double-blind, parallel-group study comparing clopidogrel (75 mg) daily to aspirin (325 mg daily).
In patients with recent myocardial infarction (within 35 days), recent ischemic stroke (within 6 months) or established peripheral arterial disease. Patients received randomized treatment for an average of 1.91 years (maximum of 3 years).
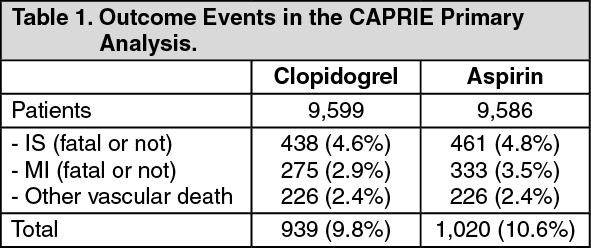
The trial's primary outcome was the time to first occurrence of new ischemic stroke (fatal or not), new myocardial infarction (fatal or not), or other vascular death. Deaths not easily attributable to nonvascular causes were all classified as vascular. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
As shown in the table, clopidogrel was associated with a lower incidence of outcome events of every kind. The overall risk reduction (9.8% vs. 10.6%) was 8.7%, p = 0.045. Similar results were obtained when all-cause mortality and all-cause strokes were counted instead of vascular mortality and ischemic strokes (risk reduction 6.9%). In patients who survived an on-study stroke or myocardial infarction, the incidence of subsequent events was again lower in the clopidogrel group. The curves showing the overall event rate are shown in Figure 1. The event curves separated early and continued to diverge over the 3-year follow-up period. (See Figure 1.)
Click on icon to see table/diagram/image
Long-term administration of clopidogrel to patients with atherosclerotic vascular disease is more effective than aspirin in reducing the combined risk of ischemic stroke, myocardial infarction, or vascular death. The overall safety profile of clopidogrel is at least as good as that of medium-dose aspirin.
The CURE study included 12,562 patients with acute coronary syndrome without ST-segment elevation (unstable angina or non-Q-wave myocardial infarction) and presenting within 24 hours of onset of the most recent episode of chest pain or symptoms consistent with ischemia.
Patients were required to have either ECG changes compatible with new ischemia (without ST-segment elevation) or elevated cardiac enzymes or troponin I or T to at least twice the upper limit of normal. Patients were randomized to receive clopidogrel (300 mg loading dose followed by 75 mg/day), (n=6,259) or placebo (n=6,303), and were treated for 3 to 12 months. Patients also received aspirin (75-325 mg once daily) and other standard therapies such as heparin (oral anticoagulants e.g. warfarin and long-term NSAIDs were not permitted). The use of GP IIb/IIIa inhibitors was not permitted for three days prior to randomization. The number of patients experiencing the primary outcome (CV death, MI, or stroke) was 582 (9.30%) in the clopidogrel-treated group and 719 (11.41%) in the placebo-treated group, a 20% relative risk reduction (95% CI of 10%-28%; p=0.00009) for the clopidogrel group (see Table 2).
At the end of 12 months, the number of patients experiencing the co-primary outcome (CV death, MI, stroke or refractory ischemia) was 1035 (16.54%) in the clopidogrel group and 1187 (18.83%) in the placebo group, a 14% relative risk reduction (95% CI of 6%-21%, p=0.0005) for the clopidogrel group (see Table 2).
Click on icon to see table/diagram/image
In the clopidogrel group, each component of the two primary endpoints (CV death, MI, stroke, refractory ischemia) occurred less frequently than in the placebo group. The benefits of clopidogrel were apparent as early as the first 24 hours after randomization and maintained throughout the course of the trial up to 12 months (see Figure 2).
Click on icon to see table/diagram/image
In CURE, the use of clopidogrel was associated with a lower incidence of CV death, MI or stroke in patient populations with different characteristics are shown in Figure 3. The benefits associated with clopidogrel tablets were independent of the use of other acute and long-term cardiovascular therapies, such as heparin/LMWH (low molecular weight heparin), IV glycoprotein IIb/IIIa (GP IIb/IIIa inhibitors), lipid-lowering drugs, beta-blockers, and ACE-inhibitors. The efficacy of clopidogrel was observed independently of the dose of aspirin (75-325 mg once daily). (See Figure 3.)
Click on icon to see table/diagram/image
The data show the consistency of the benefit of clopidogrel.
The use of clopidogrel in CURE was associated with a decrease in the use of thrombolytic therapy (71 patients [1.1%] in the clopidogrel group, 126 patients [2%] in the placebo group; relative risk reduction of 43%, p=0.0001), and GPIIb/IIIa inhibitors (369 patients [5.9%] in the clopidogrel group, 454 patients [7.2%] in the placebo group; relative risk reduction of 18%, p=0.003). There were significantly more patients with major bleeding in the clopidogrel group than in the placebo group (3.7% vs. 2.7%, relative risk 1.38, p=0.001), but there were not significantly more patients with episodes of life-threatening bleeding (2.1% vs. 1.8%, p=0.13) or hemorrhagic strokes.
In patients with acute ST-segment elevation MI, safety and efficacy of clopidogrel have been evaluated in 2 randomised, placebo-controlled, double-blind studies, Clopidogrel as Adjunctive Reperfusion Therapy (CLARITY) and Clopidogrel and Metoprolol in Myocardial Infarction Trial (COMMIT).
The CLARITY trial included 3,491 patients presenting within 12 hours after the onset of a ST-elevation MI and planned for thrombolytic therapy. Patients received clopidogrel (300 mg loading dose, followed by 75 mg once daily, n=1,752) or placebo (n=1,739), both in combination with ASA (150 to 325 mg as a loading dose, followed by 75 to 162 mg/day, a fibrinolytic agent and, when appropriate, heparin. The patients were followed for 30 days. The primary endpoint was the occurrence of the composite of an occluded infarct-related artery on the predischarge angiogram, or death or recurrent MI before coronary angiography. For patients who did not undergo angiography, the primary endpoint was death or recurrent myocardial infarction by Day 8 or by hospital discharge whichever came first. A total of 99.7% of patients received fibrinolytics (fibrin specific: 68.8%, non-fibrin specific: 31.1%), 89.5% heparin, 78.7% beta blockers, 54.7% ACE inhibitors and 63% statins.
Fifteen percent (15.0%) of patients in the clopidogrel group and 21.7% in the placebo group reached the primary endpoint, representing an absolute reduction of 6.7% in the rate and a 36% odds reduction in favor of clopidogrel (95% CI: 24, 47%; p < 0.001), mainly related to a reduction in occluded infarct-related arteries. This benefit was consistent across all prespecified subgroups including patients' age and gender, infarct location, and type of fibrinolytic or heparin used.
COMMIT trial included 45,852 patients presenting within 24 hours of the onset of the symptoms of suspected MI with supporting ECG abnormalities (i.e. ST elevation, ST depression or left bundle-branch block). Patients received clopidogrel (75 mg/day, n=22,961) or placebo (n=22,891), in combination with ASA (162 mg/day), for 28 days or until hospital discharge. The co-primary endpoints were death from any cause and the first occurrence of re-infarction, stroke or death. The population included 54.5% patients who received fibrinolytics.
Clopidogrel significantly reduced the relative risk of death from any cause by 7% (p=0.029), and the relative risk of the combination of re-infarction, stroke or death by 9% (p=0.002), representing an absolute reduction of 0.5% and 0.9%, respectively. This benefit was consistent across age, gender and with or without fibrinolytics, and was observed as early as 24 hours.
The ACTIVE-W and ACTIVE-A studies, separate trials in the ACTIVE program, included patients with atrial fibrillation (AF) who had at least one risk factor for stroke. Based on enrollment criteria, physicians enrolled patients in ACTIVE-W if they were candidates for vitamin K antagonist (VKA) therapy (such as warfarin). The ACTIVE-A study included patients who could not receive VKA therapy because they were unable or unwilling to receive the treatment.
The ACTIVE-W study demonstrated that anticoagulant treatment with vitamin K antagonists was more effective than with clopidogrel and ASA.
The ACTIVE-A study (n=7,554) was a multicenter, randomized, double-blind, placebo-controlled study which compared clopidogrel (75 mg once daily) + ASA (n=3,772) to placebo + ASA (n=3,782). The recommended dose for ASA was 75 to 100 mg/day. Patients were treated for up to 5 years.
A total of 23.0% of patients received anti-arrhythmics, 52.1% beta-blockers, 54.6% ACE inhibitors, and 25.4% statins.
The number of patients who reached the primary endpoint (time to first occurrence of stroke, MI, non-CNS systemic embolism or vascular death) was 832 (22.1%) in the group treated with clopidogrel + ASA and 924 (24.4%) in the placebo + ASA group (relative risk reduction of 11.1%; 95%CI of 2.4% to 19.1%; p=0.013), primarily due to a large reduction in the incidence of strokes. Strokes occurred in 296 (7.8%) patients receiving clopidogrel + ASA and 408 (10.8%) patients receiving placebo + ASA (relative risk reduction of 28.4%; 95%CI, 16.8% to 38.3%; p=0.00001).
Pharmacokinetics: After repeated 75 mg oral doses of clopidogrel, plasma concentrations of the parent compound, which has no platelet inhibiting effect, are very low and are generally below the quantification limit (0.00025 mg/L) beyond 2 hours after dosing.
Effect of Food: Administration of clopidogrel with meals did not significantly modify the bioavailability of active form, (thiol derivative).
Absorption and Distribution: Clopidogrel is rapidly absorbed after oral administration of repeated doses of 75 mg clopidogrel (base), with peak plasma levels (3 mg/L) of the main circulating metabolite occurring approximately 1 hour after dosing. The pharmacokinetics of the main circulating metabolite are linear (plasma concentrations increased in proportion to dose) in the dose range of 50 to 150 mg of clopidogrel. Absorption is at least 50% based on urinary excretion of clopidogrel metabolites.
Clopidogrel and the main circulating metabolite bind reversibly
in vitro to human plasma proteins (98% and 94%, respectively). The binding is nonsaturable
in vitro up to a concentration of 100 µg/mL.
Metabolism: Clopidogrel is extensively metabolised by the liver by two main metabolic pathways: One mediated by esterases and leading to hydrolysis into its inactive carboxylic acid derivative (85% of circulating metabolites), and one mediated by multiple cytochromes P450 enzymes. Clopidogrel is first metabolised to a 2-oxo-clopidogrel intermediate metabolite. Subsequent metabolism of the 2-oxo-clopidogrel intermediate metabolite results in formation of the active metabolite, a thiol derivative of clopidogrel.
In vitro, this metabolic pathway is mediated by CYP3A4, CYP2C19, CYP1A2 and CYP2B6. The active thiol metabolite binds rapidly and irreversibly to platelet receptors, thus inhibiting platelet aggregation for the lifespan of the platelet.
The C
max of the active metabolite is twice as high following a single 300 mg clopidogrel loading dose as it is after four days of 75 mg maintenance dose. C
max occurs approximately 30 to 60 minutes after dosing.
Elimination: Following an oral dose of
14C-labelled clopidogrel in man, approximately 50% was excreted in the urine and approximately 46% in the feces in the 120-hour interval after dosing. After a single oral dose of 75 mg, clopidogrel has a half-life of approximately 6 hours. The half-life of the active metabolite is approximately 30 minutes. The elimination half-life of the main circulating (inactive) metabolite was 8 hours after single and repeated administration.
Special Populations: Geriatric Patients: Plasma concentrations of the main circulating metabolite are significantly higher in elderly (≥75 years) compared to young healthy volunteers but these higher plasma levels were not associated with differences in platelet aggregation and bleeding time. No dosage adjustment is needed for the elderly.
Renal impairment: After repeated doses of 75 mg clopidogrel per day in patients with moderate (creatinine clearance from 30 to 60 ml/minute) and severe (creatinine clearance from 5 to 15 ml/minute) renal impairment, inhibition of ADP-induced platelet aggregation was lower (25%) than that observed in healthy subjects, however, the prolongation of bleeding time was similar to that seen in healthy subjects receiving 75 mg of clopidogrel/day.
Hepatic impairment: After repeated doses of 75 mg clopidogrel per day for 10 days in patients with severe hepatic impairment, inhibition of ADP-induced platelet aggregation was similar to that observed in healthy subjects. The mean bleeding time prolongation was also similar in the two groups.
Pediatric population: Clopidogrel should not be used in children because safety and efficacy in children have not been established.
Gender: No significant difference was observed in the plasma levels of the main circulating metabolite between males and females. In a small study comparing men and women, less inhibition of ADP-induced platelet aggregation was observed in women, but there was no difference in prolongation of bleeding time. In the large, controlled clinical study (Clopidogrel vs. Aspirin in Patients at Risk of Ischemic Events; CAPRIE), the incidence of clinical outcome events, other adverse clinical events, and abnormal clinical laboratory parameters was similar in men and women.
Race: The prevalence of CYP2C19 alleles that result in intermediate and poor CYP2C19 metabolism differs according to race/ethnicity. From literature limited data in Asian populations are available to assess the clinical implication of genotyping of the CYP on clinical outcome events.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image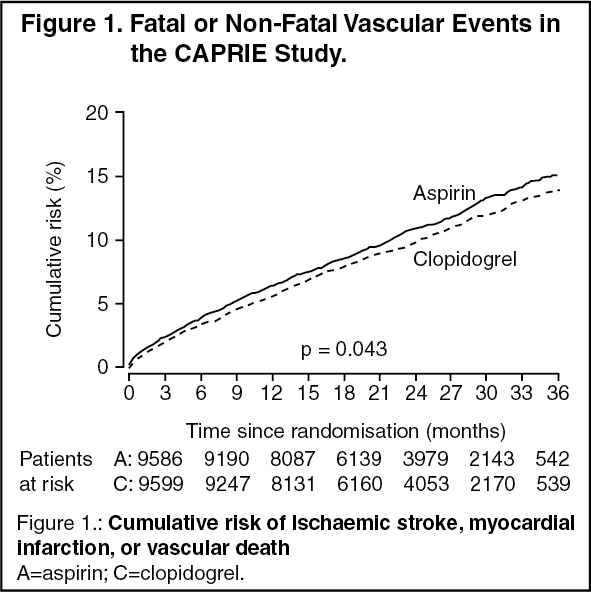 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image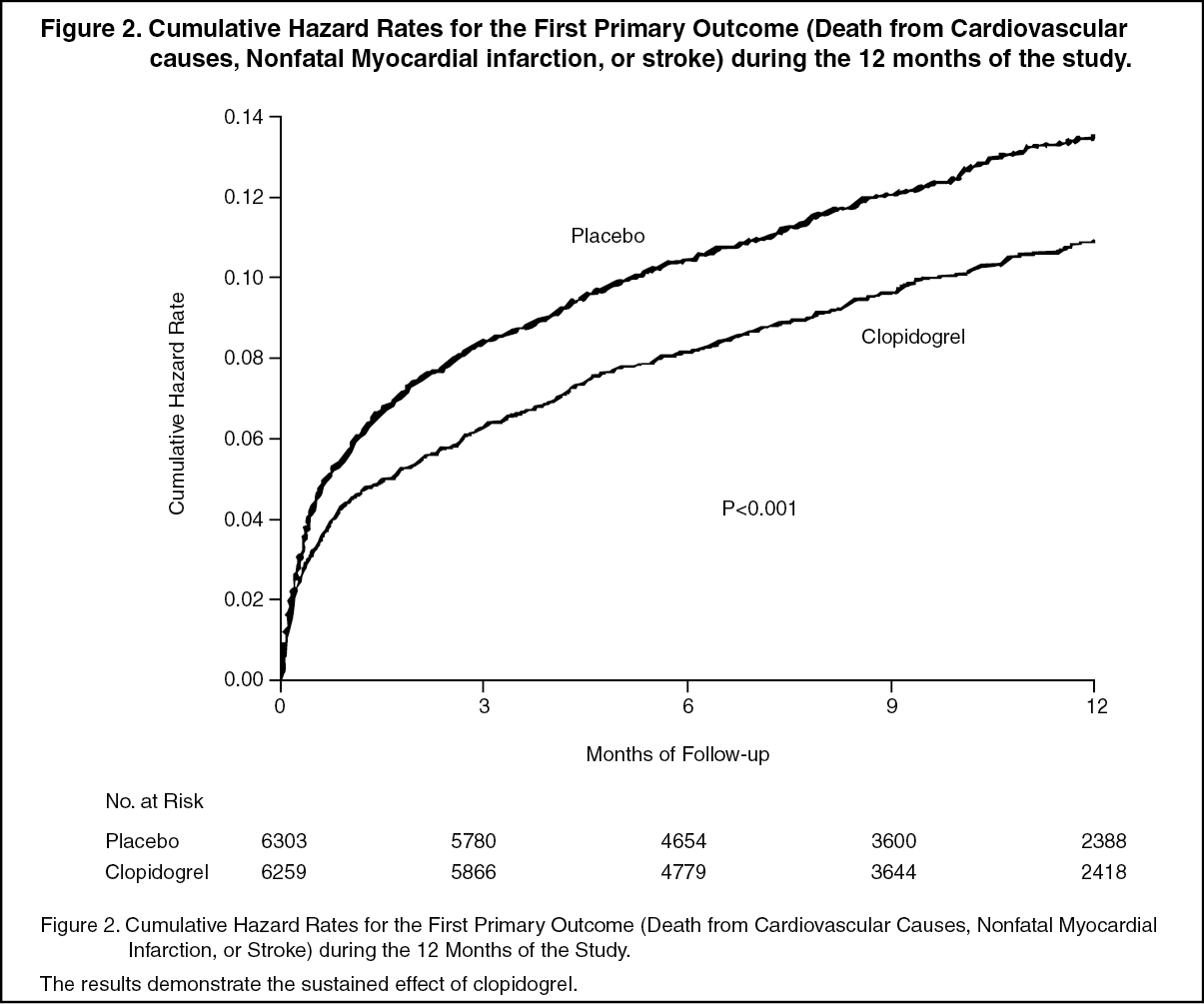 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image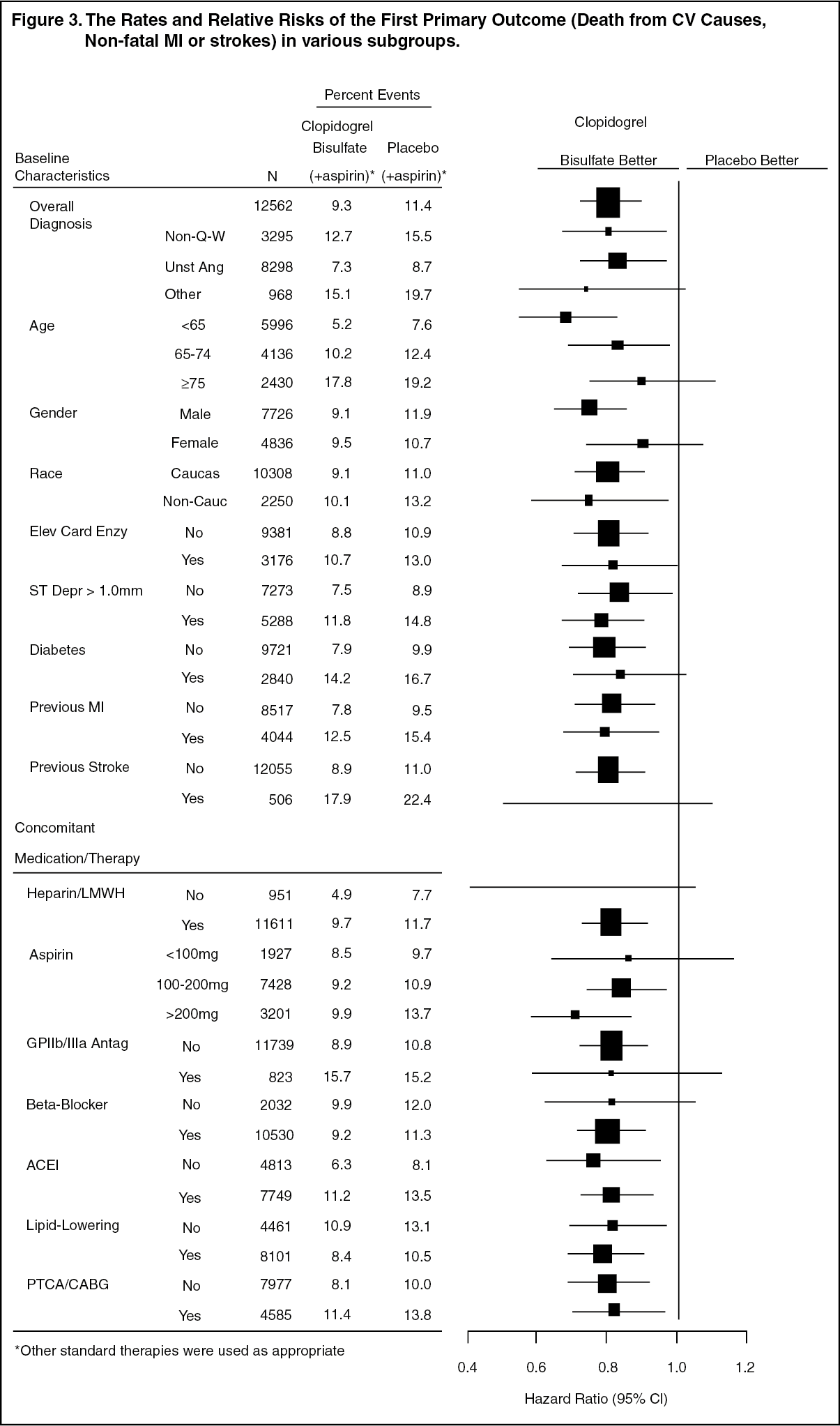 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image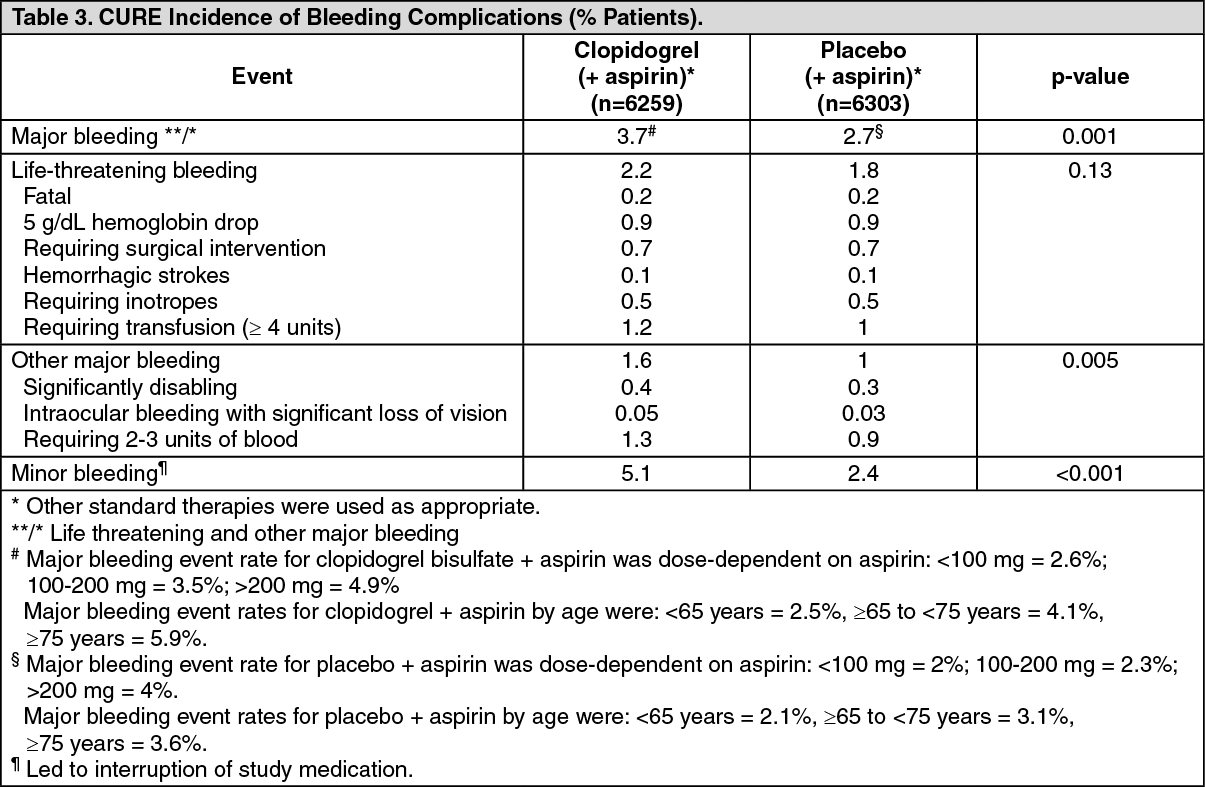 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
