In the rasagiline clinical program, overall 1,361 patients were treated with rasagiline for 3,076.4 patient years. In the double-blind, placebo-controlled studies, 529 patients were treated with rasagiline 1 mg/day for 212 patient years and 539 patients received placebo for 213 patient years.
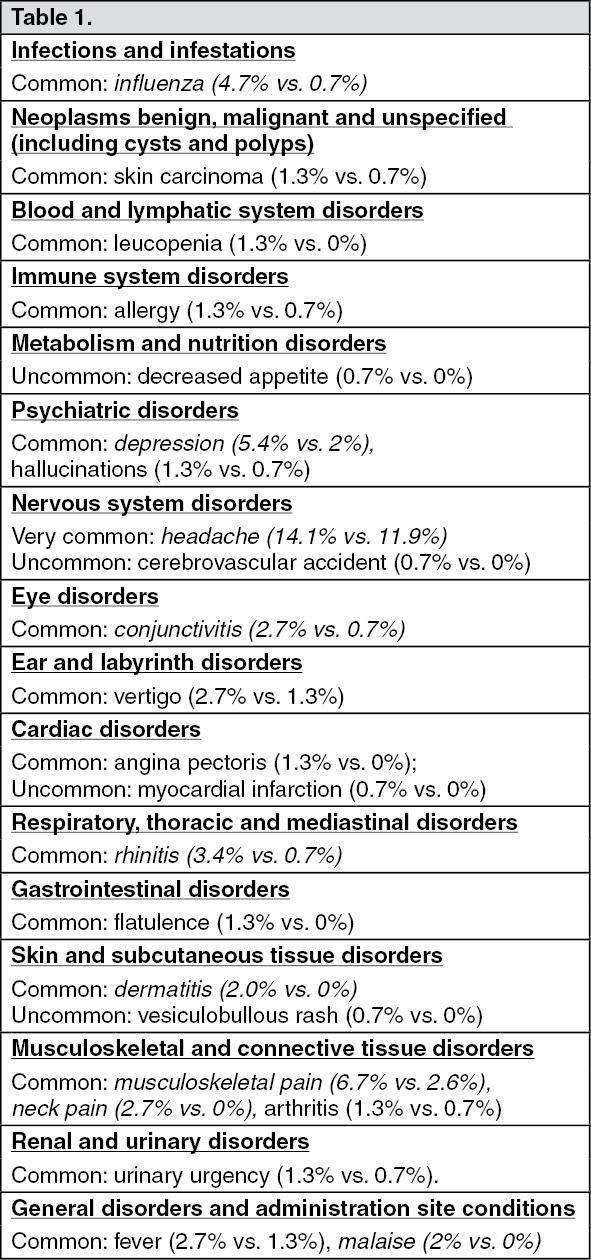
Monotherapy: The list as follows includes adverse reactions which were reported with a higher incidence in placebo-controlled studies, in patients receiving 1 mg/day rasagiline (rasagiline group n=149, placebo group n=151).
Adverse reactions with at least 2% difference over placebo are marked in
italics.
In parentheses is the adverse reaction incidence (% of patients) in rasagiline vs. placebo, respectively.
Adverse reactions are ranked under headings of frequency using the following conventions: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1000 to <1/100), rare (≥1/10000 to <1/1000), very rare (<1/10000). (See Table 1.)
 Click on icon to see table/diagram/image
Adjunct Therapy:
Click on icon to see table/diagram/image
Adjunct Therapy: The list as follows includes adverse reactions which were reported with a higher incidence in placebo-controlled studies in patients receiving 1 mg/day rasagiline (rasagiline group n=380, placebo group n=388). In parentheses is the adverse reaction incidence (% of patients) in rasagiline vs. placebo, respectively.
Adverse reactions with at least 2% difference over placebo are in
italics.
Adverse reactions are ranked under headings of frequency using the following conventions: very common (≥1/10), common (≥1/100, <1/10), uncommon (≥1/1000, <1/100), rare (≥1/10000, <1/1000), very rare (<1/10000). (See Table 2.)
Click on icon to see table/diagram/image
Parkinson's disease is associated with symptoms of hallucinations and confusion. In post-marketing experience, these symptoms have also been observed in Parkinson's disease patients treated with rasagiline.
Serious adverse reactions are known to occur with the concomitant use of SSRIs, SNRIs, tricyclic, tetracyclic antidepressants and MAO inhibitors. In the post-marketing period, cases of serotonin syndrome associated with agitation, confusion, rigidity, pyrexia and myoclonus have been reported by patients treated with antidepressants/SNRI concomitantly with rasagiline.
Rasagiline clinical trials did not allow concomitant use of fluoxetine or fluvoxamine with rasagiline, but the following antidepressants and doses were allowed in the rasagiline trials: amitriptyline ≤ 50 mg/daily, trazodone ≤ 100 mg/daily, citalopram ≤ 20 mg/daily, sertraline ≤ 100 mg/daily, and paroxetine ≤ 30 mg/daily. There were no cases of serotonin syndrome in the rasagiline clinical program in which 115 patients were exposed concomitantly to rasagiline and tricyclics and 141 patients were exposed to rasagiline and SSRIs/ SNRIs.
In the post-marketing period, cases of elevated blood pressure, including one report of hypertensive crisis associated with ingestion of unknown amounts of tyramine-rich foods, have been reported in patients taking rasagiline.
With MAO inhibitors there have been reports of drug interactions with the concomitant use of sympathomimetic medicinal products.
In post-marketing period there was one case of elevated blood pressure in a patient using the ophthalmic vasoconstrictor tetrahydrozoline hydrochloride while taking rasagiline.
Impulse control disorders: Pathological gambling, increased libido, hypersexuality, compulsive spending or buying, binge eating and compulsive eating can occur in patients treated with dopamine agonists and/or other dopaminergic treatment. A similar pattern of impulse control disorders has been reported post-marketing with rasagiline, which also included compulsions, obsessive thoughts and impulsive behaviour (see Precautions).
Excessive daytime sleepiness (EDS) and sudden sleep onset (SOS) episodes: Excessive daily sleepiness (hypersomnia, lethargy, sedation, sleep attacks, somnolence, and sudden onset of sleep) can occur in patients treated with dopamine agonists and/or other dopaminergic treatments. A similar pattern of excessive daily sleepiness has been reported post-marketing with rasagiline.
Cases of patients, treated with rasagiline and other dopaminergic medications, falling asleep while engaged in activities of daily living have been reported. Although many of these patients reported somnolence while on rasagiline with other dopaminergic medications, some perceived that they had no warning signs, such as excessive drowsiness, and believed that they were alert immediately prior to the event. Some of these events have been reported more than 1-year after initiation of treatment.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image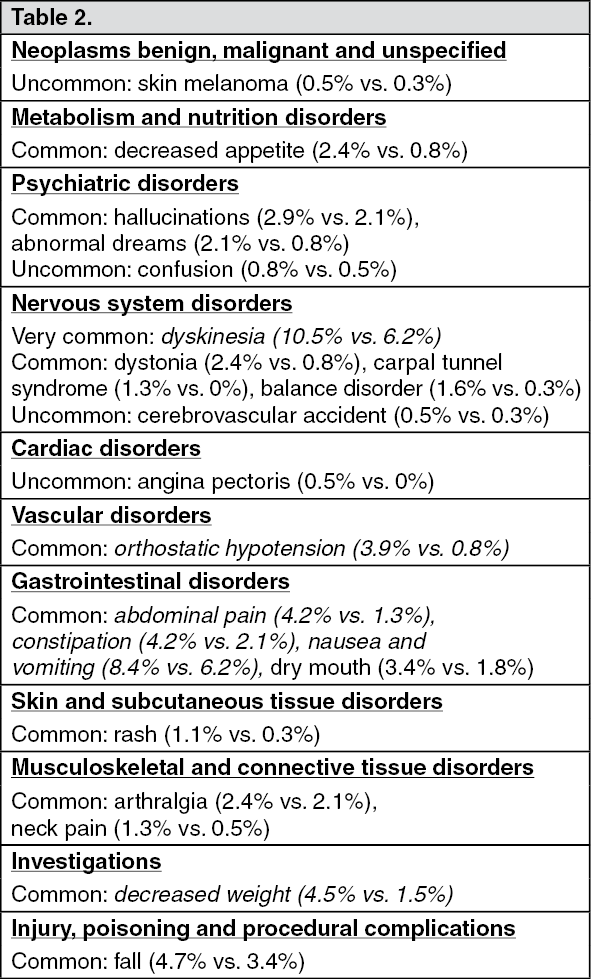 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out