Antibacterial/chemotherapeutic, gyrase inhibitor (quinolones).
Pharmacokinetics: After oral administration, Ciprobay is absorbed mainly from the small intestine, reaching peak serum concentrations 60-90 min later.
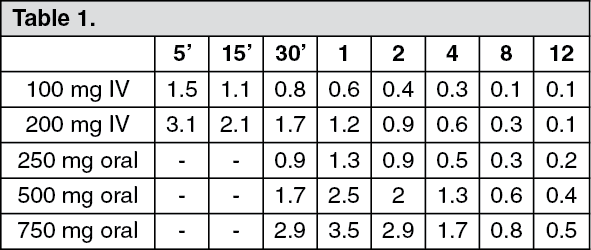
Table 1 shows serum concentrations (in mg/L) after repeated administration following a 30-min short infusion and following oral administration of Ciprobay. Table 1 shows the time from end of infusion or ingestion of tablets (hr). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In steady state, the volume of distribution of Ciprobay is 2-3 L/kg.
Since the protein-binding of Ciprobay is low (20-30%), and since the substance is present in plasma largely in a non-ionized form, almost the entire dose administered can diffuse freely into the extravascular space. In this way the concentrations in certain body fluids and tissues can clearly exceed the corresponding serum levels.
Ciprobay is excreted essentially unchanged, the bulk being eliminated by the renal route.
Renal clearance is between 3 and 5 mL/min kg, the total clearance is 8-10 mL/min kg. Ciprobay undergoes both glomerular filtration and tubular excretion. (See Table 2.)
Click on icon to see table/diagram/image
The concentrations in the bile are high, but only a small proportion of the administered dose (approximately 1%) is excreted by the biliary route.
The half-life of Ciprobay is between 3 and 5 hrs, both after oral and after IV administration.
Since Ciprobay is excreted not only renally but also to a considerable extent via the intestine, only severely impaired kidney function results in prolonged serum half-lives of up to 12 hrs.
Bioavailability: After oral administration, Ciprobay is absorbed rapidly and well (bioavailability approximately 70-80%).
Toxicology: Acute Toxicity: The acute toxicity of Ciprobay after oral administration can be classified as very low. Depending on the individual species, the LD
50 after IV infusion is 125-290 mg/kg. (See Table 3.)
Click on icon to see table/diagram/image
Subacute Tolerability Studies Over 4 Weeks: Oral Administration: Doses up to and including 100 mg/kg were tolerated without damage by rats. Pseudoallergic reactions due to histamine release were observed in dogs.
Parenteral Administration: In the highest dose group in each case (rats 80 mg/kg and monkeys 30 mg/kg), ciprofloxacin-containing crystals were found in the urine sediment. There were also changes in individual renal tubules, with typical foreign body reactions due to crystal-like precipitates.
The tubular changes observed should not (as in the case of aminoglycosides) be interpreted as a primary toxic effect of Ciprobay, but as secondary inflammatory foreign-body reactions due to the precipitation of a crystalline complex in the distal renal tubule system (see also the Subchronic and Chronic Tolerability Studies).
Subchronic Tolerability Studies Over 3 Months: Oral Administration: All doses up to and including 500 mg/kg were tolerated without damage by rats.
In monkeys, crystalluria and changes in the renal tubules were observed in the highest dose group (135 mg/kg).
Parenteral Administration: Although the changes in the renal tubules observed in rats were in some cases very slight, they were present in every dose group. In monkeys, they were found only in the highest dose group (18 mg/kg) and were associated with slightly reduced erythrocyte counts and haemoglobin values.
Chronic Tolerability Studies Over 6 Months: Oral Administration: Doses up to and including 500 and 30 mg/kg were tolerated without damage by rats and monkeys, respectively. Changes in the distal renal tubules were again observed in some monkeys in the highest-dose group (90 mg/kg).
Parenteral Administration: In monkeys, slightly elevated urea and creatinine concentrations and changes in the distal renal tubules were recorded in the highest-dose group (20 mg/kg).
Studies on Reproduction Toxicology: Fertility Studies in Rats: Fertility, the intrauterine and postnatal development of the young, and the fertility of the F
1 generation were not affected by Ciprobay.
Embryotoxicity Studies: These yielded no evidence of any embryotoxic or teratogenic action of Ciprobay.
Perinatal and Postnatal Development in Rats: No effects on the perinatal or postnatal development of the animals were detected. At the end of the rearing period histological investigations did not bring to light any sign of articular damage in the young.
Special Tolerability Studies: It is known from comparative studies in animals, both with the older gyrase inhibitors (eg, nalidixic and pipemidic acid) and the more recent ones (eg, norfloxacin and ofloxacin), that this substance class produces a characteristic damage pattern. Kidney damage, cartilage damage in weight-bearing joints of immature animals and eye damage may be encountered.
Renal Tolerability: The crystallization observed in the animal studies occurred preferentially under pH conditions that do not apply in man.
Compared to rapid injection, a slow infusion of Ciprobay reduces the danger of crystal precipitation.
The precipitation of crystals in the renal tubules does not immediately and automatically lead to kidney damage. In the animal studies, damage occurred only after high doses, with correspondingly high levels of crystalluria. For example, although they always caused crystalluria, even high doses were tolerated over 6 months without damage and without foreign body reactions occurring in individual distal renal tubules.
Damage to the kidneys without the presence of crystalluria has not been observed. The renal damage observed in the animal studies should not, therefore, as is the case with the aminoglycosides, be regarded as a primary toxic action of Ciprobay on the kidney tissue, but as typical secondary inflammatory foreign body reactions due to the precipitation of a crystalline complex of ciprofloxacin, magnesium and protein.
Articular Tolerability Studies: As is also known for other gyrase inhibitors, at high concentrations Ciprobay causes damage to the large, weight-bearing joints in immature animals.
The extent of the cartilage damage varies according to age, species and dose; the damage can be reduced by taking the weight off the joints. Studies with mature animals (rat, dog) found no evidence of cartilage lesions.
Studies Aimed at Excluding Cataractogenic Effects: On the basis of the investigations, it may be stated from a toxicological point of view that Ciprobay treatment does not involve any risk of cataract induction, particularly because in parenteral administration maximal bioavailability can be assumed and the duration of administration was 6 months.
Mutagenicity: In view of the mechanism of action of the gyrase inhibitors, a whole series of additional mutagenicity studies, going beyond what is required, was carried out to exclude the possibility of DNA-damaging effects and of any mutagenic activity of Ciprobay. No evidence was found for any mutagenic effects of the drug.
Microbiology: During the proliferation phase of a bacterium, a segmental twisting and untwisting of the chromosomes take place. An enzyme called DNA gyrase plays a decisive part in this process. Ciprobay inhibits this DNA gyrase in a way that arrests the bacterial metabolism, since vital information can no longer be read from the bacterial chromosome.
Ciprobay is extraordinarily effective
in vitro against virtually all gram-negative pathogens, including
Pseudomonas aeruginosa. It is also effective against gram-positive pathogens eg, Staphylococci and Streptococci. Anaerobes are generally less susceptible.
Ciprobay has a rapid bactericidal action, not only in the proliferation phase but also in the resting phase.
Resistance to Ciprobay develops slowly and in stages (multiple-step type).
Plasmid-mediated resistance development of the kind that occurs with β-lactam antibiotics, aminoglycosides and tetracyclines has not been observed with Ciprobay. It is of clinical interest that plasmid-carrying bacteria are also completely sensitive to Ciprobay.
On account of its special mode of action, Ciprobay does not suffer from general parallel resistance to other important, chemically different, active substance groups eg, β-lactam antibiotics, aminoglycosides, tetracyclines, macrolide and peptide antibiotics, sulfonamides, trimethoprim or nitrofuran derivatives. In its indication area, Ciprobay remains completely effective on pathogens resistant to the previously mentioned groups of antibiotics. Parallel resistance is observed within the group of gyrase inhibitors. However, because of the high primary sensitivity to Ciprobay shown by most organisms, parallel resistance is less pronounced with this drug. Ciprobay is thus also frequently effective on pathogens that are already resistant to the less effective gyrase inhibitors.
Because of its chemical structure, Ciprobay is completely effective on β-lactamase-forming bacteria.
Ciprobay can be used in combination with another antibiotic.
In vitro studies with usually sensitive pathogens, carried out using Ciprobay in combination with β-lactam antibiotics and aminoglycosides, have shown primarily additive or indifferent effects; synergistic increases in efficacy were relatively rare and antagonistic effects very rare.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image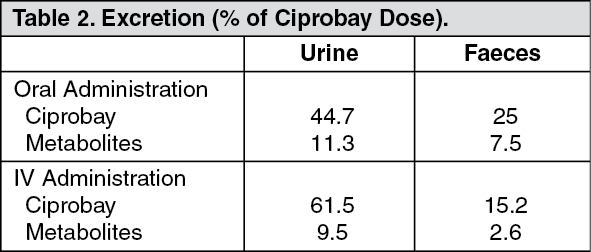 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image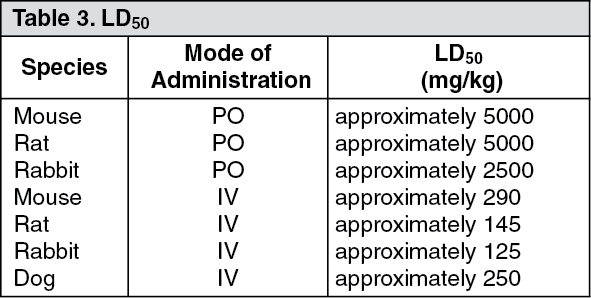 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out