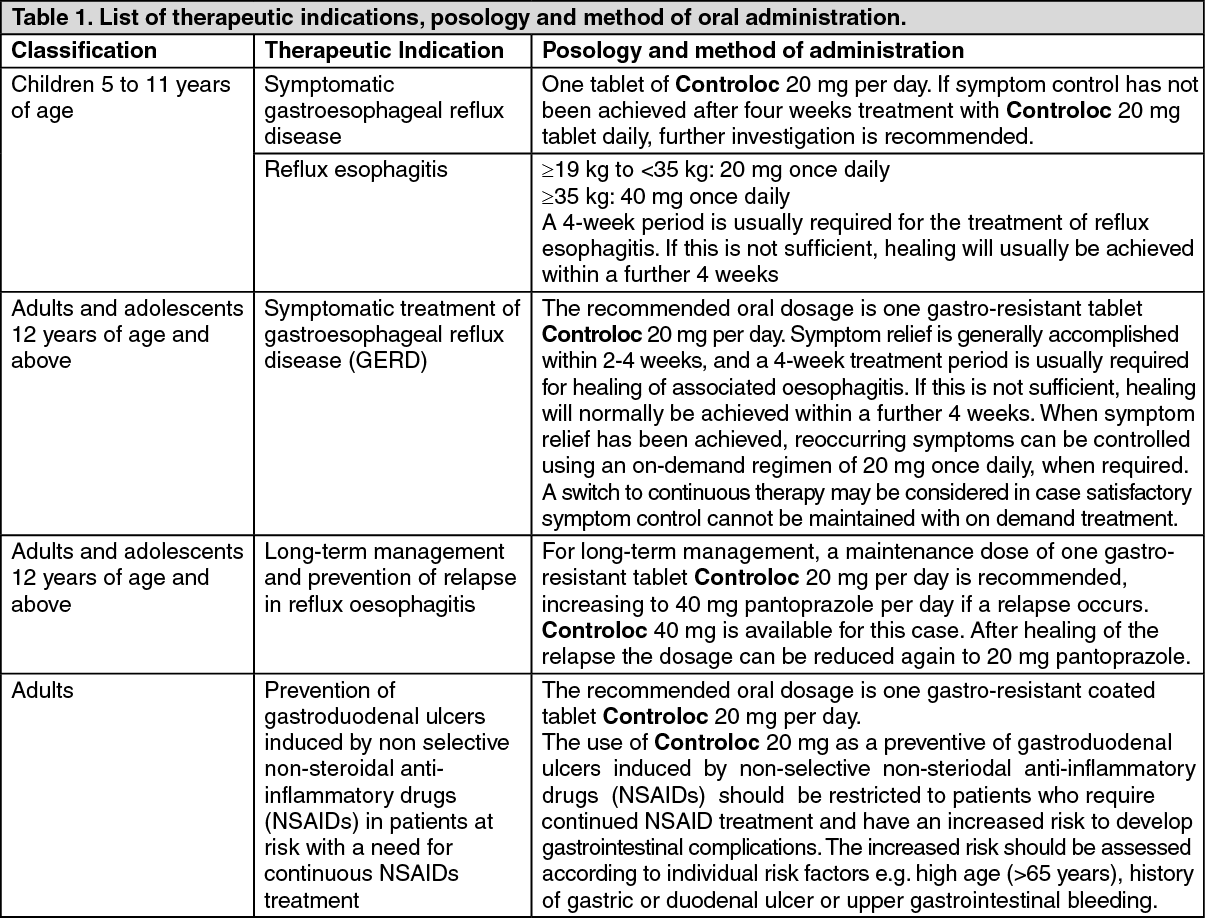
Controloc 20 mg tab: General instructions: Controloc 20 mg gastro-resistant tablets should not be chewed or crushed, and should be swallowed whole with some water. (See Table 1.)
 Click on icon to see table/diagram/image
Special Patient Populations: Elderly patients:
Click on icon to see table/diagram/image
Special Patient Populations: Elderly patients: No dose adjustment is necessary in elderly patients.
Pediatric patients: Controloc is not recommended for use in children below 5 years of age due to limited data on safety and efficacy in this age group.
Impaired hepatic function: A daily dose of 20 mg pantoprazole should not be exceeded in patients with severe liver impairment.
Impaired renal function: No dose adjustment is necessary patients with impaired renal function.
Controloc 40 mg tab: Tablets should not be chewed or crushed, and should be swallowed whole with some water. (See Table 2.)
Click on icon to see table/diagram/image
Special Patient Populations: Elderly patients: No dose adjustment is necessary in elderly patients.
Pediatric patients: Controloc is not recommended for use in children below 5 years of age due to limited data on safety and efficacy in this age group.
Impaired renal function: No dose adjustment is necessary in patients with impaired renal function.
Pantoprazole 40 mg must not be used in combination treatment (e.g. amoxicillin, clarithromycin) for eradication of
H. pylori in patients with impaired renal function, since currently no data are available on the efficacy and safety of pantoprazole in combination treatment for these patients.
Impaired hepatic function: A daily dose of 20 mg pantoprazole should not be exceeded in patients with severe liver impairment (see Precautions).
Pantoprazole 40 mg must not be used in combination treatment (e.g. amoxicillin, clarithromycin) for eradication of
H. pylori in patients with moderate to severe hepatic dysfunction since currently no data are available on the efficacy and safety of pantoprazole in combination treatment of these patients (see Precautions).
Controloc IV: The intravenous administration of Controloc i.v. is recommended only if oral application is not appropriate.
Recommended dosage: Duodenal ulcer, gastric ulcer, moderate and severe reflux esophagitis: The recommended intravenous dosage is one vial (40 mg pantoprazole) Controloc i.v. per day.
Long-term management of Zollinger-Ellison-Syndrome and other pathological hypersecretory conditions: Patients should start their treatment with a daily dose of 80 mg Controloc i.v.. Thereafter, the dosage can be titrated up or down as needed using measurements of gastric acid secretion to guide. With doses above 80 mg daily, the dose should be divided and given twice daily. A temporary increase of the dosage above 160 mg pantoprazole is possible but should not be applied longer than required for adequate acid control.
In case of rapid acid control is required, a starting dose of 2 x 80 mg Controloc i.v. is sufficient to manage a decrease of acid output into the target range (<10 mEq/h) within one hour in the majority of patients. Transition from Controloc i.v. to the oral formulation of Controloc should be performed as soon as it is clinically justified.
Method of administration and General instructions: A ready-to-use solution is prepared by injecting 10 ml of physiological sodium chloride solution into the vial containing the dry substance. This solution may be administered directly or may be administered after mixing with 100 ml physiological sodium chloride solution or 5% glucose.
After preparation the solution must be used within 12 hours.
Controloc i.v. should not be manufactured or mixed with solvents other than those stated.
As soon as oral therapy is possible, treatment with Controloc i.v. should be discontinued and 40 mg pantoprazole p.o. (by mouth) should be administered instead.
The drug should be administered intravenously over 2-15 minutes.
Keep the vial in the outer carton in order to protect from light.
Special Patient Populations: Paediatric patients: The experience in children is limited. Therefore, Controloc i.v. 40 mg powder for solution for injection is not recommended for use in patients below 18 years of age.
Impaired hepatic function: A daily dose of 20 mg pantoprazole (half a vial of 40 mg Controloc I.V.) should not be exceeded in patients with severe liver impairment (see Precautions).
In addition, pantoprazole 40 mg must not be used in combination treatment (e.g. amoxicillin, clarithromycin) for eradication of
H. pylori in patients with moderate to severe hepatic dysfunction since currently no data are available on the efficacy and safety of pantoprazole in combination treatment of these patients (see Precautions).
Impaired renal function: No dose adjustment is necessary in patients with impaired renal function.
In addition, pantoprazole 40 mg must not be used in combination treatment (e.g. amoxicillin, clarithromycin) for eradication of
H. pylori in patients with impaired renal function, since currently no data are available on the efficacy and safety of pantoprazole in combination treatment for these patients.
Elderly patients: No dose adjustment is necessary in elderly patients.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image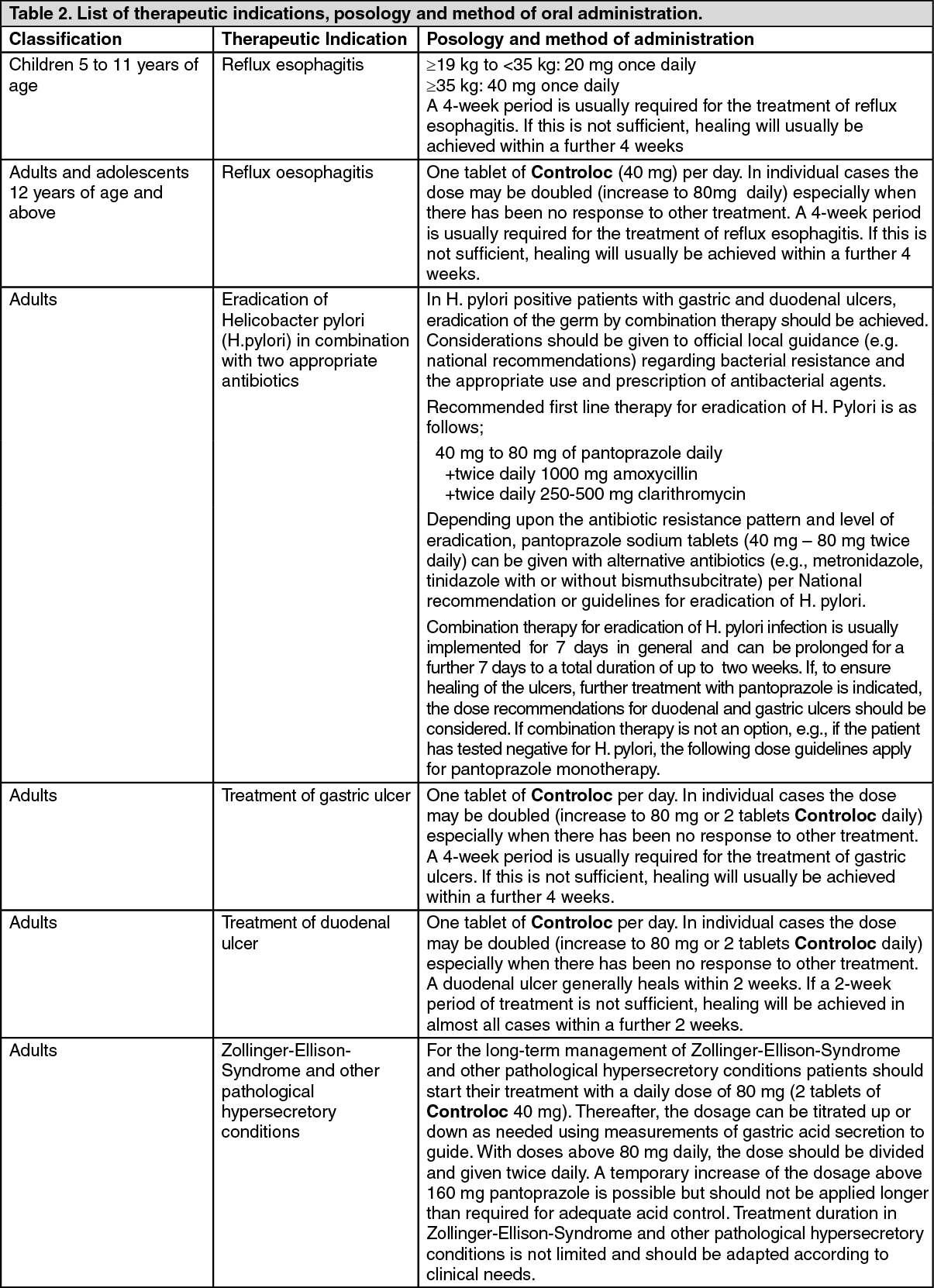 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
