1 mg (0.01 ml) of enoxaparin corresponds approximately to 100 anti-Xa I.U.
For subcutaneous use, enoxaparin sodium injection should not be mixed with other injections or infusions.
Do not inject intramuscularly.
Subcutaneous administration technique: The prefilled syringes are ready-to-use. The air bubble from the syringe should not be expelled before the injection. The subcutaneous injection should preferably be made when the patient is lying down. Enoxaparin is administered in the subcutaneous cellular tissue of the anterolateral or posterolateral abdominal wall, alternately on the left and the right side. The injectable itself consists in introducing the needle perpendicularly and not tangentially, throughout its entire length into a fold of skin held between the thumb and index finger. The skin fold should be held throughout the injection. Do not rub the injection site after completion of the injection.
Prophylaxis of venous thromboembolism during surgical procedures, including cancer surgery: Enoxaparin sodium is given by subcutaneous injection; treatment is usually continued for 7 to 10 days or until the patient is ambulant.
Patients at low to moderate risk are given 20 mg (2000 units) once daily with the first dose about 2 hours pre-operatively.
In patients at high risk, such as those undergoing orthopedic surgery, the dose should be increased to 40 mg (4000 units) once daily with the initial dose given about 12 hours before the procedure. Alternatively, a dose of 30 mg (3000 units) may be given subcutaneously twice daily, starting within 12 to 24 hours after the operation. After hip replacement surgery, enoxaparin sodium may be continued in a dose of 40 mg (4000 units) once daily for a further 4-5 weeks.
For patients with a high venous thromboembolism (VTE) risk who undergo abdominal or pelvic surgery for cancer an extended thromboprophylaxis up to 4 weeks is recommended.
Prophylaxis of deep vein thrombosis (DVT) in medical patients with severely restricted mobility during acute illness: For the prophylaxis of deep vein thrombosis (DVT) in immobilised medical patients with acute medical conditions such as heart failure (NYHA class III or IV), acute respiratory failure, acute infections or acute rheumatic disease, the dose is 40 mg (4000 units) once daily for at least 6 days; treatment should be continued until the patient is fully ambulant up to a maximum of 14 days.
Treatment of established deep vein thrombosis with or without pulmonary embolism: The recommended dose is 1 mg/kg subcutaneously every 12 hours for 5 to 10 days. Afterward, the dosage is adjusted to 1.5 mg/kg subcutaneously once daily for up to 6 months. The benefit of anticoagulant therapy should be re-evaluated after 6 months of treatment.
Duration of therapy: Treatment with low-molecular-weight heparin should be quickly replaced by oral anticoagulant therapy, unless contraindicated. Treatment duration with LMWH should not exceed 10 days, including the time needed to reach the required oral anticoagulant effect, except when this is difficult to achieve. Oral anticoagulant treatment should therefore be initiated as soon as possible.
In the extended treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE) and prevention of its recurrence in patients with active cancer, physicians should carefully assess the individual thromboembolic and bleeding risks of the patient.
Prevention of thrombus formation in the extra-corporal circulation during hemodialysis: The recommended dose is 1 mg/kg. Enoxaparin should be introduced in the arterial line of the circuit at the beginning of the dialysis session. The effect of this dose is usually sufficient for a 4-hour session; in the event fibrin rings are found, a further dose of 0.5 to 1 mg/kg may be given. The dose should be reduced in patients at high risk of hemorrhage.
Treatment of unstable angina/non-Q-wave myocardial infarction during the acute stage, in combination with aspirin: A dose of 1 mg/kg should be given subcutaneously every 12 hours. The recommended treatment should be prescribed for a period of 2 to 8 days, until clinical stabilization of the patient. Enoxaparin should be administered concurrently with aspirin (100 to 325 mg daily per oral route).
Treatment of Acute ST-Segment Elevation Myocardial Infarction: In acute ST-elevation myocardial infarction the initial dose of enoxaparin is 30 mg (3000 units) intravenously, with a subcutaneous dose of 1 mg/kg given at the same time. Further dose of 1 mg/kg should be given subcutaneously every 12 hours for 8 days or until hospital discharge.
The first 2 subcutaneous doses should not exceed 100 mg (10000 units) each.
When administered in conjunction with a thrombolytic (fibrin-specific or non-fibrin specific), Enoxaparin Sodium should be given between 15 minutes before and 30 minutes after the start of fibrinolytic therapy.
Patients aged 75 years and older should be given subcutaneous doses only; the recommended dose is 0.75 mg/kg every 12 hours, with a maximum of 75 mg for each of first 2 doses.
Concomitant therapy: Unless contraindicated, all patients should receive aspirin (indefinitely).
For patients who undergo a percutaneous coronary intervention, an additional intravenous doses of 0.3 mg/kg should be given at the time of the procedure if the last subcutaneous dose was given more than 8 hours previously.
Special populations: Elderly: No dosage adjustment is necessary in preventive therapy. In curative therapy measurement of anti-Xa activity is recommended.
Children: Enoxaparin is not recommended for children.
Patients under 40 kg and over 100 kg weight: Particular clinical surveillance is necessary in order to adjust dosage if necessary. In all cases, strictly follow the Physician's prescription.
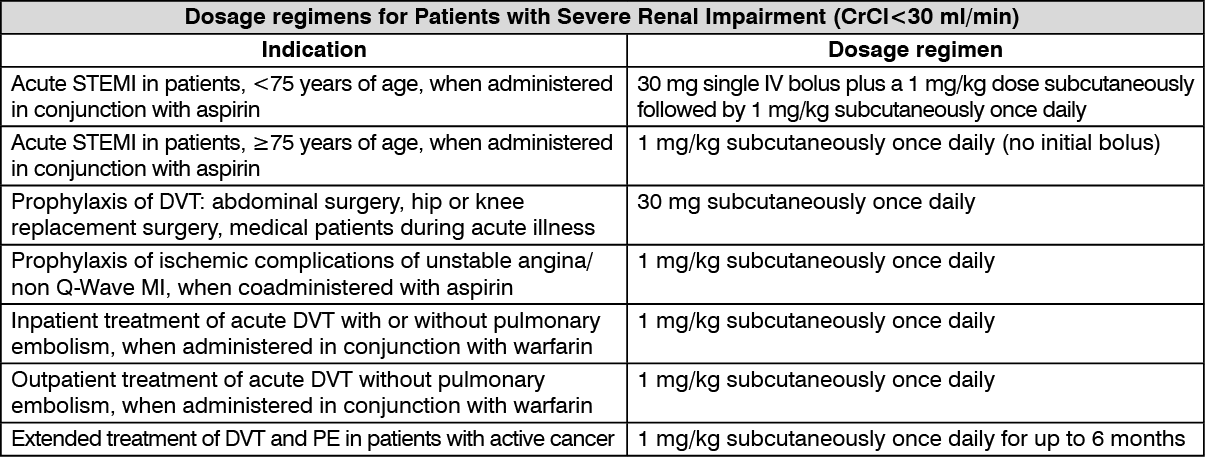
Renal impairment: Although no dose adjustment is recommended in patients with moderate (creatinine clearance 30 to 50 ml/min) and mild (creatinine clearance 50 to 80 ml/min) renal impairment, all such patients should be observed carefully for signs and symptoms of bleeding.
The recommended prophylaxis and treatment dosage regimens for patients with severe renal impairment (creatinine clearance <30 ml/min) are described in the table as follows. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out