The information highlighted (if any) are the most recent updates for this brand.
Each tablet contains 2 mg dienogest.
Excipients/Inactive Ingredients: Lactose monohydrate, Magnesium stearate, Maize starch, Povidone.
Pharmacotherapeutic group: Progestogens. ATC code: G03DB08.
Pharmacology: Pharmacodynamics: Dienogest is a nortestosterone derivative with no androgenic but rather an antiandrogenic activity of approximately one third of that of cyproterone acetate. Dienogest binds to the progesterone receptor of the human uterus with only 10% of the relative affinity of progesterone. Despite its low affinity to the progesterone receptor, dienogest has a strong progestogenic effect in vivo. Dienogest has no significant androgenic, mineralocorticoid or glucocorticoid activity in vivo.
Dienogest acts on endometriosis by reducing the endogenous production of oestradiol and thereby suppresses the trophic effects of estradiol on both the eutopic and ectopic endometrium. When given continuously, dienogest leads to a hypoestrogenic, hypergestagenic endocrine environment causing initial decidualization of endometrial tissue followed by atrophy of endometriotic lesions.
Data on efficacy: Superiority of dienogest over placebo was demonstrated in a 3-months study including 198 patients with endometriosis. Endometriosis-associated pelvic pain was measured on a Visual Analog Scale (0-100 mm). After 3 months of treatment with Dienogest 2 mg a statistically significant difference compared to placebo (Δ = 12.3 mm; 95%CI: 6.4 - 18.1; p<0.0001) and a clinically meaningful reduction of pain compared to baseline (mean reduction = 27.4 mm ± 22.9) were demonstrated.
After 3 months of treatment, reduction of endometriosis-associated pelvic pain by 50% or more without relevant increase of concomitant pain medication was achieved in 32.4% of patients on Dienogest 2 mg (placebo: 13.5%); a reduction of endometriosis-associated pelvic pain by 75% or more without relevant increase of concomitant pain medication was achieved in 18.6% of patients on Dienogest 2mg (placebo: 5.2%).
The open-label extension to this placebo-controlled study suggested a continued improvement of endometriosis-associated pelvic pain for a treatment duration of up to 15 months.
The placebo controlled results were supported by the results obtained in a 6 months active-controlled study versus a GnRH agonist including 252 patients with endometriosis.
Three studies including a total of 252 patients who received a daily dose of 2 mg dienogest demonstrated a substantial reduction of endometriotic lesions after 6 months of treatment.
Data on safety: Endogenous estrogen levels are moderately suppressed during treatment with Dienogest 2 mg.
Currently, long-term data on bone mineral density (BMD) and risk of fractures in users of Dienogest 2 mg are not available.
No significant changes of the mean values of standard laboratory parameters (including haematology, blood chemistry, liver enzymes, lipids and HbA1C) were observed during treatment with Dienogest 2 mg.
Safety in adolescents: The safety of dienogest with respect to BMD was investigated in an uncontrolled clinical trial over 12 months in 111 adolescent women with clinically suspected or confirmed endometriosis. The mean relative change in BMD of the lumbar spine from baseline was -1.2%. In a subset of the patients with decreased BMD a follow-up measurement was performed 6 months after end of treatment and showed an increase in BMD towards pretreatment levels.
Pharmacokinetics: Absorption: Orally administered dienogest is rapidly and almost completely absorbed. Peak serum concentrations of 47 ng/ml are reached at about 1.5 hours after single ingestion. Bioavailability is about 91%. The pharmacokinetics of dienogest are dose-proportional within the dose range of 1 - 8 mg.
Distribution: Dienogest is bound to serum albumin and does not bind to sex hormone binding globulin (SHBG) or corticoid binding globulin (CBG). 10% of the total serum drug concentration is present as free steroid, 90% is non-specifically bound to albumin.
The apparent volume of distribution (Vd/F) of dienogest is 40 l.
Metabolism: Dienogest is completely metabolized by the known pathways of steroid metabolism, with the formation of endocrinologically mostly inactive metabolites. Based on in vitro and in vivo studies, CYP3A4 is the major enzyme involved in the metabolism of dienogest. The metabolites are excreted very quickly so that in plasma unchanged dienogest is the dominating fraction.
The metabolic clearance rate from serum Cl/F is 64 ml/min.
Elimination: Dienogest serum levels decrease in two phases. The terminal disposition phase is characterized by a half-life of approximately 9-10 hours. Dienogest is excreted in form of metabolites which are excreted at a urinary to faecal ratio of about 3:1 after oral administration of 0.1 mg/kg. The half-life of urinary metabolites excretion is 14 hours. Following oral administration approximately 86% of the dose administered is eliminated within 6 days, the bulk of this amount excreted within the first 24 h, mostly with the urine.
Steady-state conditions: Pharmacokinetics of dienogest are not influenced by SHBG levels. Following daily ingestion drug serum levels increase about 1.24 fold reaching steady-state conditions after 4 days of treatment. The pharmacokinetics of dienogest after repeated administration of ENDOVELLE can be predicted from single dose pharmacokinetics.
Pharmacokinetics in Special Population: ENDOVELLE has not been studied specifically in renally impaired subjects.
ENDOVELLE has not been studied in subjects with hepatic impairment.
Toxicology: Preclinical safety data: Preclinical data reveal no special risks for humans based on conventional studies of repeated dose toxicity, genotoxicity, carcinogenic potential and toxicity to reproduction. However, it should be borne in mind that sex steroids can promote the growth of certain hormone-dependent tissues and tumours.
Treatment of endometriosis.
Posology: The dosage of ENDOVELLE is one tablet daily without any break, taken preferably at the same time each day with some liquid as needed. The tablet can be taken with or without food.
Tablets must be taken continuously without regard to vaginal bleeding. When a pack is finished the next one should be started without interruption.
There is no experience with ENDOVELLE treatment >15 months in patients with endometriosis. Treatment can be started on any day of the menstrual cycle.
Any hormonal contraception needs to be stopped prior to initiation of ENDOVELLE. If contraception is required, non-hormonal methods of contraception should be used (e.g. barrier method).
Management of missed tablets: The efficacy of ENDOVELLE may be reduced in the event of missed tablets, vomiting and/or diarrhea (if occurring within 3-4 hours after tablet taking). In the event of one or more missed tablets, the woman should take one tablet only, as soon as she remembers, and should then continue the next day at her usual time. A tablet not absorbed due to vomiting or diarrhea should likewise be replaced by one tablet.
Additional information on special populations: Paediatric population: ENDOVELLE is not indicated in children prior to menarche.
Dienogest has been studied in children ≥12 years and adolescents for up to 12 months of therapy.
Geriatric population: There is no relevant indication for use of ENDOVELLE in the Geriatric population.
Patients with hepatic impairment: ENDOVELLE is contraindicated in patients with present or past severe hepatic disease (see Contraindications).
Patients with renal impairment: There are no data suggesting the need for a dosage adjustment in patients with renal impairment.
Method of administration: For oral use.
Acute toxicity studies performed with dienogest did not indicate a risk of acute adverse effects in case of inadvertent intake of a multiple of the daily therapeutic dose. There is no specific antidote. A daily intake of 20-30 mg dienogest (10 to 15 times higher dose than in ENDOVELLE) over 24 weeks of use was very well tolerated.
ENDOVELLE not be used in the presence of any of the conditions listed as follows, which are partially derived from information on other progesteron-only preparations. Should any of the conditions appear during the use of ENDOVELLE, treatment must be discontinued immediately: active venous thromboembolic disorder; arterial and cardiovascular disease, past or present (e.g. myocardial infarction, cerebrovascular accident, ischemic heart disease); diabetes mellitus with vascular involvement; presence or history of severe hepatic disease as long as liver function values have not returned to normal; presence or history of liver tumours (benign or malignant); known or suspected sex hormone-dependent malignancies; undiagnosed vaginal bleeding; hypersensitivity to the active substance or to any of the excipients listed in Description.
As ENDOVELLE is a progestogen-only preparation it can be assumed that the special warnings and precautions for use of progestogen-only preparations are also valid for the use of ENDOVELLE although not all of the warnings and precautions are based on respective findings in the clinical studies with dienogest.
If any of the conditions/risk factors mentioned as follows is present or deteriorates, an individual risk-benefit analysis should be done before treatment with ENDOVELLE can be started or continued.
Serious uterine bleeding: Uterine bleeding, for example in women with adenomyosis uteri or uterine leiomyomata, may be aggravated with the use of ENDOVELLE. If bleeding is heavy and continuous over time, this may lead to anemia (severe in some cases). In the event of anemia, discontinuation of ENDOVELLE should be considered.
Changes in bleeding pattern: The majority of patients treated with dienogest experience changes in their menstrual bleeding pattern (see Adverse Reactions).
Circulatory disorders: From epidemiological studies there is little evidence for an association between progestogen-only preparations and an increased risk of myocardial infarction or cerebral thromboembolism. Rather, the risk of cardiovascular and cerebral events is related to increasing age, hypertension, and smoking. In women with hypertension the risk of stroke may be slightly enhanced by progestogen-only preparations.
Although not statistically significant, some studies indicate that there may be a slightly increased risk of venous thromboembolism (deep venous thrombosis, pulmonary embolism) associated with the use of progestogen-only preparations. Generally recognized risk factors for venous thromboembolism (VTE) include a positive personal or family history (VTE in a sibling or a parent at a relatively early age), age, obesity, prolonged immobilization, major surgery or major trauma. In case of long-term immobilization it is advisable to discontinue the use of ENDOVELLE (in the case of elective surgery at least four weeks in advance) and not to resume treatment until two weeks after complete remobilization.
The increased risk of thromboembolism in the puerperium must be considered.
Treatment should be stopped at once if there are symptoms of an arterial or venous thrombotic event or suspicion thereof.
Tumours: A meta-analysis from 54 epidemiological studies reported that there is a slightly increased relative risk (RR = 1.24) of having breast cancer diagnosed in women who are currently using oral contraceptives (OCs), mainly using estrogen-progestogen preparations. The excess risk gradually disappears during the course of the 10 years after cessation of combined OC (COC) use. Because breast cancer is rare in women under 40 years of age, the excess number of breast cancer diagnoses in current and recent COC users is small in relation to the overall risk of breast cancer. The risk of having breast cancer diagnosed in users of progestogen-only preparations is possibly of similar magnitude to that associated with COC. However, for progestogen-only preparations, the evidence is based on much smaller populations of users and so is less conclusive than that for COCs. These studies do not provide evidence for causation. The observed pattern of increased risk may be due to an earlier diagnosis of breast cancer in OC users, the biological effects of OCs or a combination of both. The breast cancers diagnosed in users of OCs tend to be less advanced clinically than the cancers diagnosed in those who have never used OCs.
In rare cases, benign liver tumours, and even more rarely, malignant liver tumours have been reported in users of hormonal substances such as the one contained in ENDOVELLE. In isolated cases, these tumours have led to life-threatening intra-abdominal haemorrhages. A hepatic tumour should be considered in the differential diagnosis when severe upper abdominal pain, liver enlargement or signs of intra-abdominal haemorrhage occur in women taking ENDOVELLE.
Osteoporosis: Changes in bone mineral density (BMD).
The use of dienogest in adolescents over a treatment period of 12 months was associated with a decrease in bone mineral density (BMD) in the lumbar spine. The mean relative change in BMD from baseline to the end of treatment (EOT) was -1.2%.
Repeated measurement at 6 months after the EOT in a subgroup with decreased BMD values showed a trend towards recovery.
Loss of BMD is of particular concern during adolescence and early adulthood, a critical period of bone accretion. It is unknown if BMD decrease in this population will reduce peak bone mass and increase the risk for fracture in later life (see Dosage & Administration and Pharmacology: Pharmacodynamics under Actions).
In patients who are at an increased risk of osteoporosis a careful risk-benefit assessment should be performed before starting ENDOVELLE because endogenous estrogen levels are moderately decreased during treatment with ENDOVELLE (see Pharmacology: Pharmacodynamics under Actions).
Adequate intake of calcium and Vitamin D, whether from the diet or from supplements, is important for bone health in women of all ages.
Other conditions: Patients who have a history of depression should be carefully observed and the drug should be discontinued if the depression recurs to a serious degree.
Dienogest generally does not appear to affect blood pressure in normotensive women. However, if a sustained clinically significant hypertension develops during the use of ENDOVELLE, it is advisable to withdraw ENDOVELLE and treat the hypertension.
Recurrence of cholestatic jaundice and/or pruritus which occurred first during pregnancy or previous use of sex steroids necessitates the discontinuation of ENDOVELLE.
Dienogest may have a slight effect on peripheral insulin resistance and glucose tolerance. Diabetic women, especially those with a history of gestational diabetes mellitus, should be carefully observed while taking ENDOVELLE.
Chloasma may occasionally occur, especially in women with a history of chloasma gravidarum. Women with a tendency to chloasma should avoid exposure to the sun or ultraviolet radiation whilst taking ENDOVELLE.
Pregnancies that occur among users of progestogen-only preparations used for contraception are more likely to be ectopic than are pregnancies among users of combined oral contraceptives.
Therefore, in women with a history of extrauterine pregnancy or an impairment of tube function, the use of ENDOVELLE should be decided on only after carefully weighing the benefits against the risks.
Persistent ovarian follicles (often referred to as functional ovarian cysts) may occur during the use of ENDOVELLE. Most of these follicles are asymptomatic, although some may be accompanied by pelvic pain.
Lactose: Each ENDOVELLE tablet contains lactose monohydrate. Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Effects on ability to drive and use machines: Not known.
Pregnancy: There is limited data from the use of dienogest in pregnant women.
Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity (see Pharmacology: Toxicology: Preclinical safety data under Actions).
ENDOVELLE must not be administered to pregnant women because there is no need to treat endometriosis during pregnancy.
Lactation: Treatment with ENDOVELLE during lactation is not recommended.
It is unknown whether dienogest is excreted in human milk. Data in animals have shown excretion of dienogest in rat milk.
A decision must be made whether to discontinue breast-feeding or to abstain from ENDOVELLE therapy taking into account the benefit of breast-feeding for the child and the benefit of therapy for the woman.
Fertility: Based on the available data, ovulation is inhibited in the majority of patients during treatment with dienogest. However, ENDOVELLE is not a contraceptive.
If contraception is required a non-hormonal method should be used (See Dosage & Administration).
Based on available data, the menstrual cycle returns to normal within 2 months after cessation of treatment with ENDOVELLE.
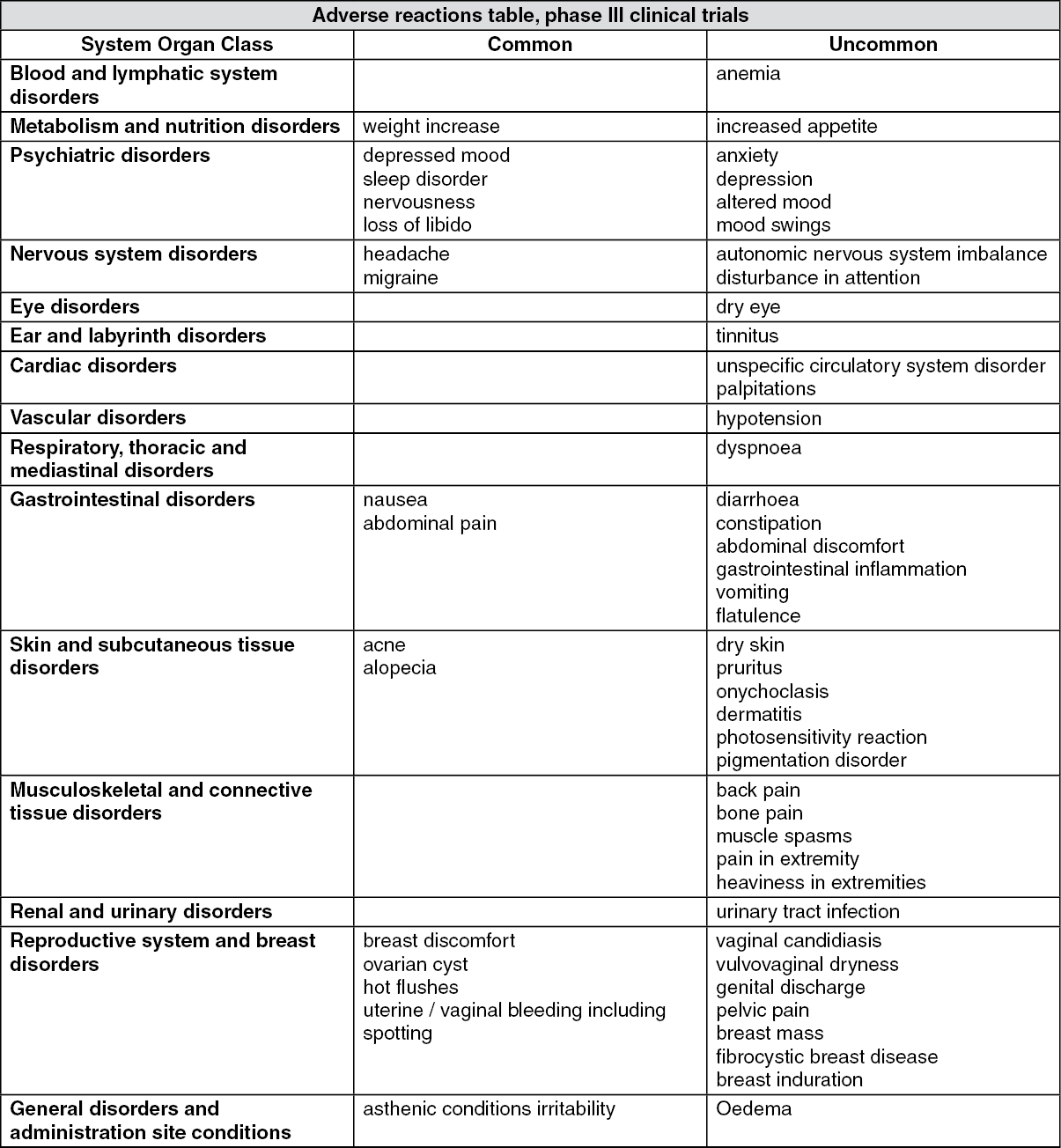
Undesirable effects are more common during the first months after the start of treatment with ENDOVELLE, and subside with continued treatment. There may be changes in bleeding pattern, such as spotting, irregular bleeding or amenorrhea. The following undesirable effects have been reported in users of Dienogest 2mg tablets.
The most frequently reported undesirable effects under treatment with Dienogest 2 mg are headache (6.6%) and breast discomfort (5.3%).
In addition, the majority of patients treated with dienogest experience changes in their menstrual bleeding pattern. Menstrual bleeding patterns were assessed systematically using patient diaries and were analyzed using the WHO 90 days reference period method. During the first 90 days of treatment with Dienogest 2mg the following bleeding patterns were observed (n=290; 100%): Amenorrhea (1.7%), infrequent bleeding (27.2%), frequent bleeding (13.4%), irregular bleeding (35.2%), prolonged bleeding (38.3%), normal bleeding, i.e. none of the previous categories (19.7%). During the fourth reference period the following bleeding patterns were observed (n=149; 100%): Amenorrhea (28.2%), infrequent bleeding (24.2%), frequent bleeding (2.7%), irregular bleeding (21.5%), prolonged bleeding (4.0%), normal bleeding, i.e. none of the previous categories (22.8%). Changes in menstrual bleeding patterns were only occasionally reported as adverse event by the patients (See adverse event table).
The frequencies of adverse drug reactions (ADRs) by MedDRA system organ classes (MedDRA SOCs) reported with Dienogest 2 mg are summarized in the table as follows. Within each frequency grouping, undesirable effects are presented in order of decreasing frequency. Frequencies are defined as common (≥1/100 to <1/10) and uncommon (≥1/1,000 to <1/100). (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Note: The prescribing information of concomitant medication should be consulted to identify potential interactions.
Effects of other medication on ENDOVELLE: Progestogens including dienogest are metabolized mainly by the cytochrome P450 3A4 system (CYP3A4) located both in the intestinal mucosa and in the liver. Therefore, inducers or inhibitors of CYP3A4 may affect the progestogen drug metabolism.
An increased clearance of sex hormones due to enzyme induction may reduce the therapeutic effect of ENDOVELLE and may result in undesirable effects e.g. changes in the uterine bleeding profile.
A reduced clearance of sex hormones due to enzyme inhibition may increase the exposure to dienogest and may result in undesirable effects.
Substances increasing the clearance of sex hormones (diminished efficacy by enzyme-induction), e.g.: phenytoin, barbiturates, primidone, carbamazepine, rifampicin, and possibly also oxcarbazepine, topiramate, felbamate, griseofulvin, and products containing St. John's wort (Hypericum perforatum).
Enzyme induction can already be observed after a few days of treatment. Maximum enzyme induction is generally seen within a few weeks. After cessation of drug therapy enzyme induction may be sustained for about 4 weeks.
The effect of the CYP 3A4 inducer rifampicin was studied in healthy postmenopausal women. Co-administration of rifampicin with estradiol valerate/dienogest tablets led to significant decreases in steady state concentrations and systemic exposures of dienogest and estradiol. The systemic exposure of dienogest at steady state, measured by AUC (0-24h), was decreased by 83%.
Substances with variable effects on the clearance of sex hormones: When co-administered with sex hormones, many combinations of HIV protease inhibitors and non-nucleoside reverse transcriptase inhibitors, including combinations with HCV inhibitors can increase or decrease plasma concentrations of the progestin. The net effect of these changes may be clinically relevant in some cases.
Substances decreasing the clearance of sex hormones (enzyme inhibitors): Dienogest is a substrate of cytochrome P450 (CYP) 3A4.
The clinical relevance of potential interactions with enzyme inhibitors remains unknown.
Concomitant administration of strong CYP3A4 inhibitors can increase plasma concentrations of dienogest.
Coadministration with the strong CYP3A4 enzyme inhibitor ketoconazole resulted in a 2.9-fold increase of AUC (0-24h) at steady state for dienogest. Concomitant administration of the moderate inhibitor erythromycin increased the AUC (0-24h) of dienogest at steady state by 1.6-fold.
Effects of dienogest 2mg on other medication: Based on in vitro inhibition studies, a clinically relevant interaction of dienogest with the cytochrome P450 enzyme mediated metabolism of other medication is unlikely.
Interaction with food: A standardized high fat meal did not affect the bioavailability of dienogest 2 mg.
Laboratory tests: The use of progestogens may influence the results of certain laboratory tests, including biochemical parameters of liver, thyroid, adrenal and renal function, plasma levels of (carrier) proteins (e.g. corticosteroid binding globulin and lipid/lipoprotein fractions), parameters of carbohydrate metabolism and parameters of coagulation and fibrinolysis. Changes generally remain within the normal laboratory range.
Incompatibilities: Not applicable.
Store below 30°C in the outer carton to protect from light.
Shelf-life: 3 years.
G03DB08 - dienogest ; Belongs to the class of pregnadien derivative progestogens used in progestogenic hormone preparations.
Endovelle tab 2 mg
1 × 28's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out