


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of action: Enhertu, trastuzumab deruxtecan, is a HER2-targeted antibody-drug conjugate. The antibody is a humanised anti-HER2 IgG1 attached to deruxtecan, a topoisomerase I inhibitor (DXd) bound by a tetrapeptide-based cleavable linker. The antibody-drug conjugate is stable in plasma. The function of the antibody portion is to bind to HER2 expressed on the surface of certain tumour cells. After binding, the trastuzumab deruxtecan complex then undergoes internalisation and intracellular linker cleavage by lysosomal enzymes that are upregulated in cancer cells. Upon release, the membrane-permeable DXd causes DNA damage and apoptotic cell death. DXd, an exatecan derivative, is approximately 10 times more potent than SN-38, the active metabolite of irinotecan.
In vitro studies indicate that the antibody portion of trastuzumab deruxtecan, which has the same amino acid sequence as trastuzumab, also binds to FcγRIIIa and complement C1q. The antibody mediates antibody-dependent cellular cytotoxicity (ADCC) in human breast cancer cells that overexpress HER2. In addition, the antibody inhibits signalling through the phosphatidylinositol 3-kinase (PI3-K) pathway in human breast cancer cells that overexpress HER2.
Clinical efficacy: DESTINY-Breast03 (NCT03529110): The efficacy and safety of Enhertu were studied in DESTINY-Breast03, a multicentre, open-label, active-controlled, randomised, two-arm phase 3 study that enrolled patients with HER2-positive, unresectable or metastatic breast cancer who received prior trastuzumab and taxane therapy for metastatic disease or developed disease recurrence during or within 6 months of completing adjuvant therapy.
Archival breast tumour samples were required to show HER2 positivity defined as HER2 IHC 3+ or ISH-positive. The study excluded patients with a history of ILD/pneumonitis requiring treatment with steroids or ILD/pneumonitis at screening, patients with untreated and symptomatic brain metastases, patients with a history of clinically significant cardiac disease, and patients with prior treatment with an anti-HER2 antibody-drug conjugate in the metastatic setting. Patients were randomised 1:1 to receive either Enhertu 5.4 mg/kg (N=261) or trastuzumab emtansine 3.6 mg/kg (N=263) administered by intravenous infusion once every three weeks. Randomisation was stratified by hormone receptor status, prior treatment with pertuzumab, and history of visceral disease. Treatment was administered until disease progression, death, withdrawal of consent, or unacceptable toxicity.
The primary efficacy outcome measure was progression-free survival (PFS) as evaluated by blinded independent central review (BICR) according to Response Evaluation Criteria in Solid Tumours (RECIST v1.1). Overall survival (OS) was a key secondary efficacy outcome measure. PFS based on investigator assessment, confirmed objective response rate (ORR), and duration of response (DOR) were secondary endpoints.
Patient demographics and baseline disease characteristics were balanced between treatment arms. Of the 524 patients randomised, the baseline demographic and disease characteristics were: median age 54 years (range: 20 to 83); 65 years or older (20.2%); female (99.6%); Asian (59.9%), White (27.3%), Black or African American (3.6%); Eastern Cooperative Oncology Group (ECOG) performance status 0 (62.8%) or 1 (36.8%); hormone receptor status (positive: 51.9%); presence of visceral disease (73.3%); presence of brain metastases at baseline (15.6%); and 48.3% of patients received one line of prior systemic therapy in the metastatic setting. The percentage of patients who had not received prior treatment for metastatic disease was 9.5%. The percentage of patients who were previously treated with pertuzumab was 61.1%.
At the prespecified interim analysis for PFS based on 245 events (73% of total events planned for final analysis), the study showed a statistically significant improvement in PFS per BICR in patients randomised to Enhertu compared to trastuzumab emtansine. PFS by BICR data from the primary analysis (data cutoff 21 May 2021) and updated OS, ORR and DOR results from data cutoff 25 July 2022 are presented in Table 1. (See Table 1, Figures 1 and 2.)
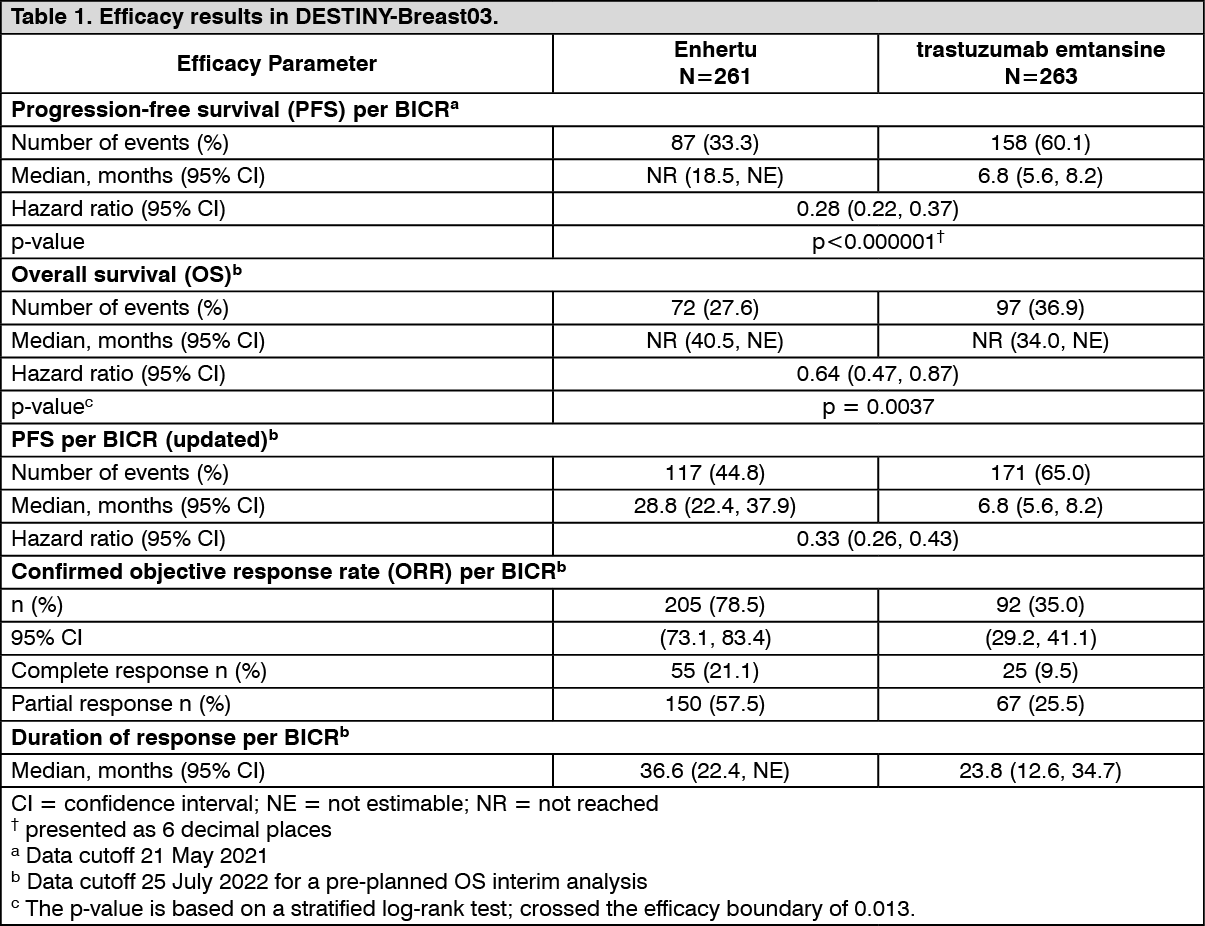 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image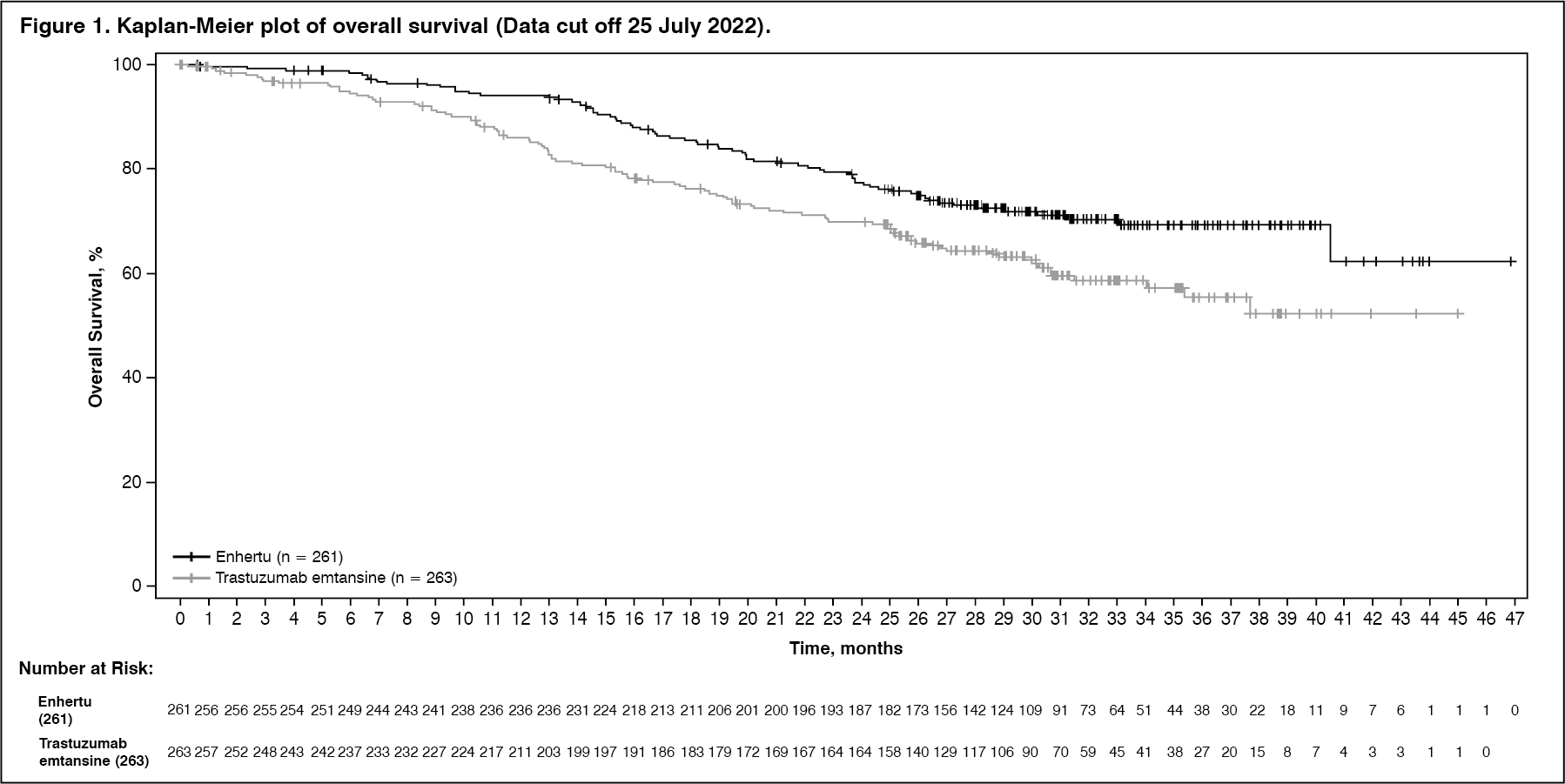 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image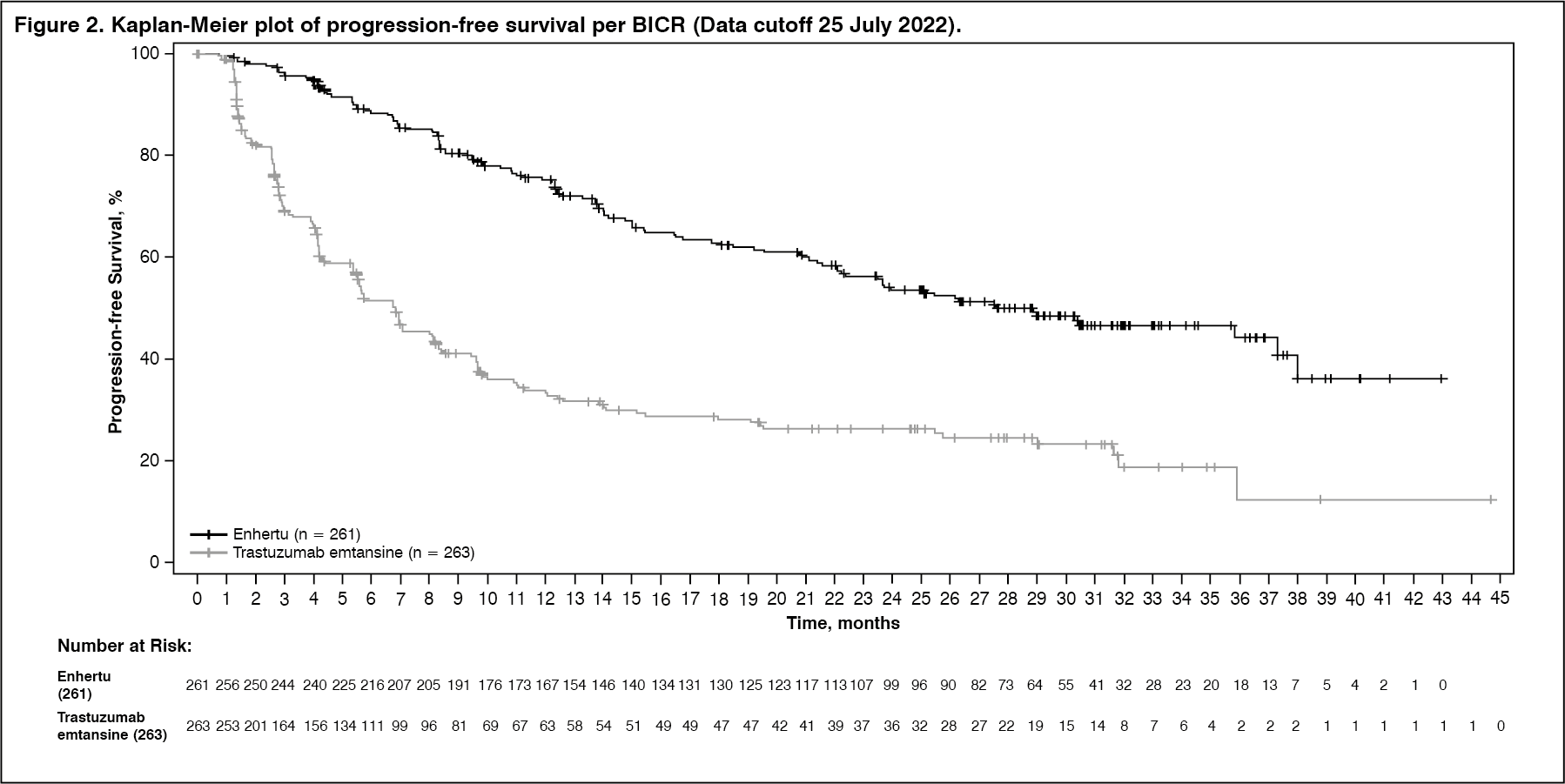 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSimilar PFS results were observed across prespecified subgroups including prior pertuzumab therapy, hormone receptor status, and presence of visceral disease.
DESTINY-Breast02 (NCT03523585): The efficacy and safety of Enhertu were evaluated in study DESTINY-Breast02, a Phase 3, randomised, multicentre, open-label, active-controlled study that enrolled patients with unresectable or metastatic HER2-positive breast cancer, who were resistant or refractory to prior T-DM1 therapy. Archival breast tumour samples were required to show HER2 positivity defined as HER2 IHC 3+ or ISH-positive. The study excluded patients with a history of ILD/pneumonitis requiring treatment with steroids or ILD/pneumonitis at screening, patients with untreated and symptomatic brain metastases and patients with a history of clinically significant cardiac disease. Patients were randomised 2:1 to receive either Enhertu 5.4 mg/kg (n=406) by intravenous infusion every three weeks, or treatment of physician's choice (n=202, trastuzumab plus capecitabine or lapatinib plus capecitabine). Randomisation was stratified by hormone receptor status, prior treatment with pertuzumab and history of visceral disease. Treatment was administered until disease progression, death, withdrawal of consent or unacceptable toxicity.
The primary efficacy outcome measure was progression-free survival (PFS) as assessed by blinded independent central review (BICR) based on RECIST v1.1. Overall survival (OS) was a key secondary efficacy outcome measure. PFS based on investigator assessment, confirmed objective response rate (ORR) and duration of response (DOR) were secondary objectives.
Demographic and baseline disease characteristics were similar between treatment arms. Of the 608 patients randomised, the median age was 54 years (range 22 to 88); female (99.2%); White (63.2%), Asian (29.3%), Black or African American (2.8%); Eastern Cooperative Oncology Group (ECOG) performance status 0 (57.4%) or 1 (42.4%); hormone receptor status (positive: 58.6%); presence of visceral disease (78.3%); presence of brain metastases at baseline (18.1%) and 4.9% of patients received one line of prior systemic therapy in the metastatic setting.
Efficacy results are summarised in Table 2 and Figures 3 and 4. (See Table 2, Figures 3 and 4.)
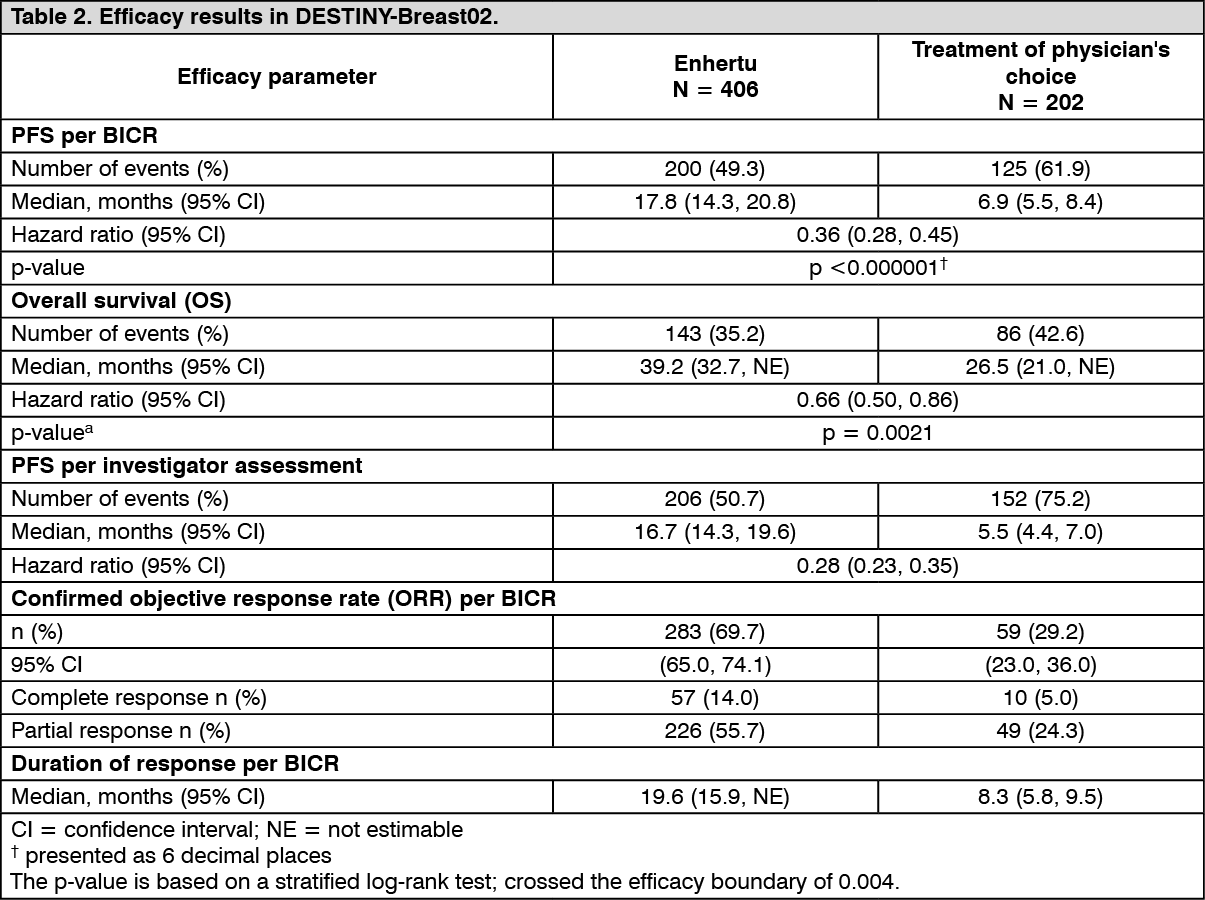 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image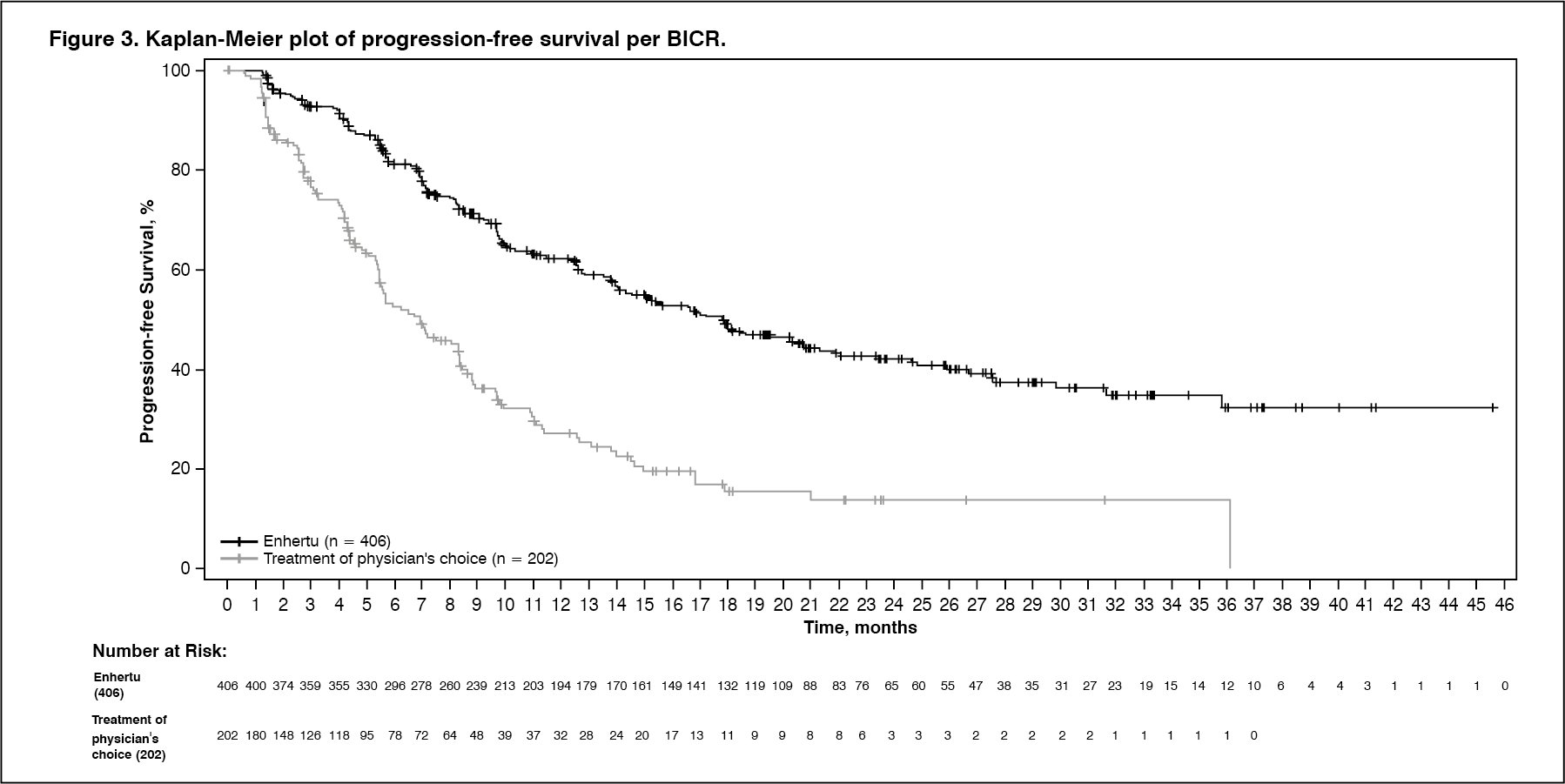 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image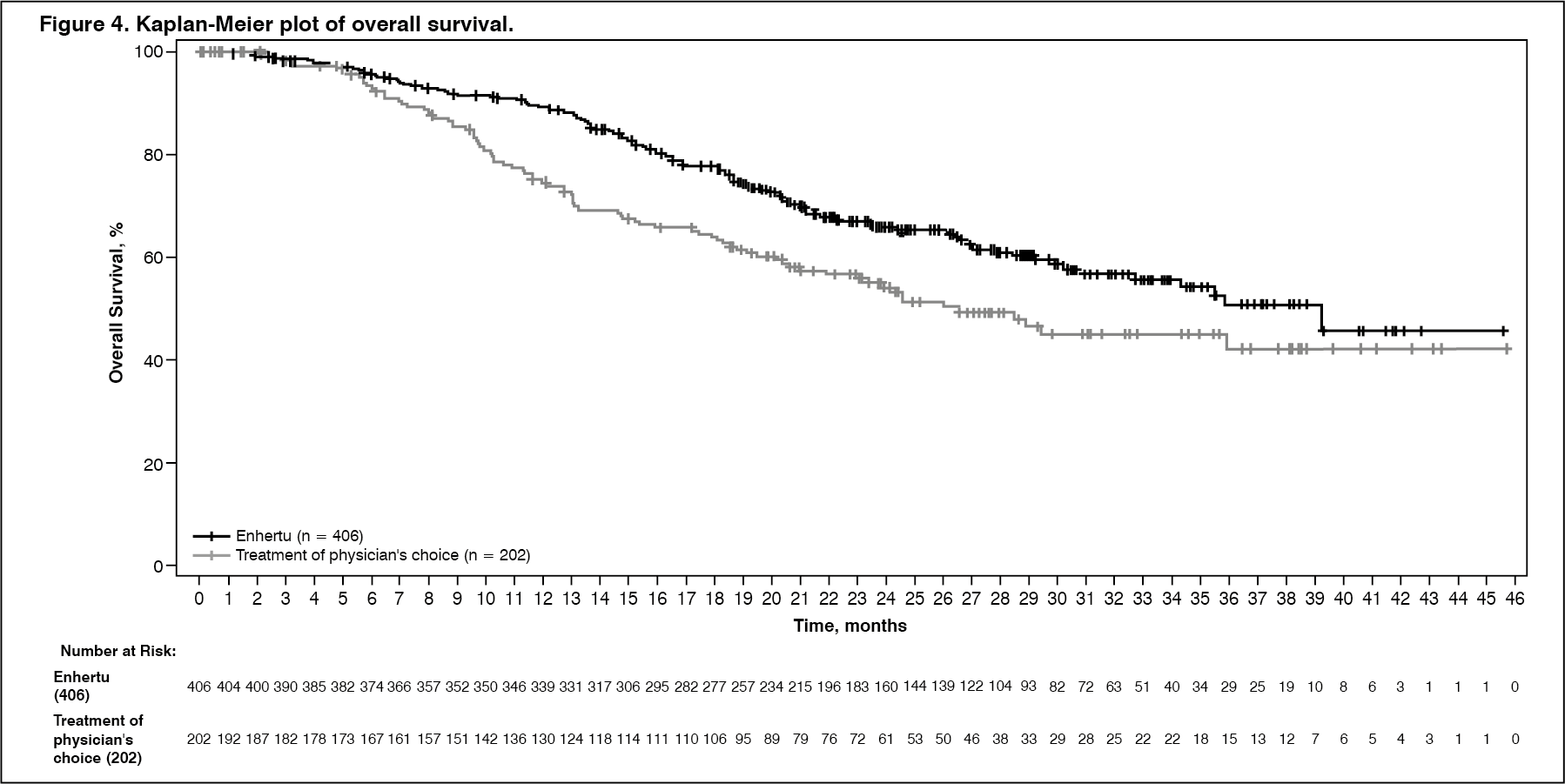 Click on icon to see table/diagram/image
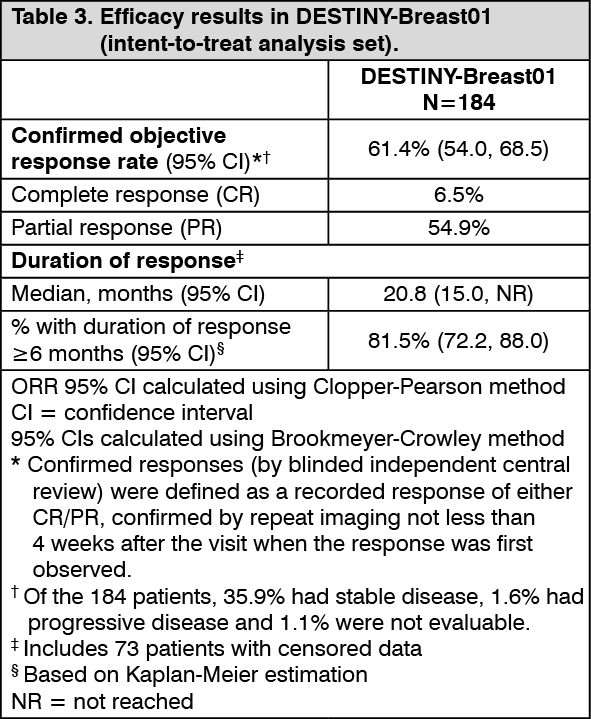
Click on icon to see table/diagram/imageDESTINY-Breast01 (NCT03248492): The efficacy and safety of Enhertu were studied in DESTINY-Breast01, a multicentre, open-label, single-arm Phase 2 study that enrolled patients with HER2-positive, unresectable and/or metastatic breast cancer who had received two or more prior anti-HER2-based regimens, including trastuzumab emtansine (100%), trastuzumab (100%) and pertuzumab (65.8%). Archival breast tumour samples were required to show HER2 positivity defined as HER2 IHC 3+ or ISH-positive. The study excluded patients with a history of treated ILD or ILD at screening, patients with untreated or symptomatic brain metastases, and patients with a history of clinically significant cardiac disease. Patients enrolled had at least 1 measurable lesion per RECIST v1.1.
Enhertu was administered by intravenous infusion at 5.4 mg/kg once every three weeks until disease progression, death, withdrawal of consent, or unacceptable toxicity. The primary efficacy outcome measure was confirmed objective response rate (ORR) according to RECIST v1.1 in the intent-to-treat (ITT) population as evaluated by independent central review (ICR). The secondary efficacy outcome measure was duration of response (DOR).
Of the 184 patients enrolled in DESTINY-Breast01, baseline demographic and disease characteristics were: median age 55 years (range: 28 to 96); 65 years or older (23.9%); female (100%); White (54.9%), Asian (38.0%), Black or African-American (2.2%); Eastern Cooperative Oncology Group (ECOG) performance status 0 (55.4%) or 1 (44.0%); hormone receptor status (positive: 52.7%); presence of visceral disease (91.8%); previously treated and stable brain metastases (13.0%); median number of prior therapies in the metastatic setting: 5 (range: 2 to 17); sum of diameters of target lesions (<5 cm: 42.4%, ≥5 cm: 50.0%).
An earlier analysis (median duration of follow-up 11.1 months [range: 0.7 to 19.9 months]) showed a confirmed objective response rate of 60.9% (95% CI: 53.4, 68.0) with 6.0% being complete responders and 54.9% being partial responders; 36.4% had stable disease, 1.6% had progressive disease and 1.1% were not evaluable. Median duration of response at that time was 14.8 months (95% CI: 13.8, 16.9) with 81.3% of responders having a response of ≥ 6 months (95% CI: 71.9, 87.8). Efficacy results from an updated data cutoff with median duration of follow-up of 20.5 months (range: 0.7 to 31.4 months) are shown in Table 3. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageConsistent anti-tumour activity was observed across prespecified subgroups based on prior pertuzumab therapy and hormone receptor status.
Pharmacokinetics: Absorption: Trastuzumab deruxtecan is administered intravenously. There have been no studies performed with other routes of administration.
Distribution: Based on population pharmacokinetic analysis, the volume of distribution of the central compartment (Vc) of trastuzumab deruxtecan and topoisomerase I inhibitor, DXd, were estimated to be 2.68 L and 28.0 L, respectively.
In vitro, the mean human plasma protein binding of DXd was approximately 97%.
In vitro, the blood to plasma concentration ratio of DXd was approximately 0.6.
Biotransformation: Trastuzumab deruxtecan undergoes intracellular cleavage by lysosomal enzymes to release the DXd.
The humanised HER2 IgG1 monoclonal antibody is expected to be degraded into small peptides and amino acids via catabolic pathways in the same manner as endogenous IgG.
In vitro metabolism studies in human liver microsomes indicate that DXd is metabolised mainly by CYP3A4 via oxidative pathways.
Elimination: Following intravenous administration of trastuzumab deruxtecan in patients with metastatic HER2-positive or HER2-low breast cancer, the clearance of trastuzumab deruxtecan in population pharmacokinetic analysis was calculated to be 0.4 L/day and the clearance of DXd was 18.4 L/h. In patients with locally advanced or metastatic gastric or GEJ adenocarcinoma, trastuzumab deruxtecan clearance was 20% higher than in patients with metastatic HER2-positive breast cancer. In cycle 3, the apparent elimination half-life (t½) of trastuzumab deruxtecan and released DXd was approximately 7 days. Moderate accumulation (approximately 35% in cycle 3 compared to cycle 1) of trastuzumab deruxtecan was observed.
Following intravenous administration of DXd to rats, the major excretion pathway was faeces via the biliary route. DXd was the most abundant component in urine, faeces, and bile. Following single intravenous administration of trastuzumab deruxtecan (6.4 mg/kg) to monkeys, unchanged released DXd was the most abundant component in urine and faeces. DXd excretion was not studied in humans.
In vitro interactions: Effects of Enhertu on the pharmacokinetics of other medicinal products: In vitro studies indicate DXd does not inhibit major CYP450 enzymes including CYP1A2, 2B6, 2C8, 2C9, 2C19, 2D6 and 3A. In vitro studies indicate that DXd does not inhibit OAT1, OAT3, OCT1, OCT2, OATP1B1, OATP1B3, MATE1, MATE2-K, P-gp, BCRP, or BSEP transporters.
Effects of other medicinal products on the pharmacokinetics of Enhertu: In vitro, DXd was a substrate of P-gp, OATP1B1, OATP1B3, MATE2-K, MRP1, and BCRP. No clinically meaningful interaction is expected with medicinal products that are inhibitors of MATE2-K, MRP1, P-gp, OATP1B, or BCRP transporters (see Interactions).
Linearity/non-linearity: The exposure of trastuzumab deruxtecan and released DXd when administered intravenously increased in proportion to dose in the 3.2 mg/kg to 8.0 mg/kg dose range (approximately 0.6 to 1.5 times the recommended dose) with low to moderate inter-subject variability. Based on population pharmacokinetic analysis, inter-subject variability in trastuzumab deruxtecan and DXd elimination clearances were 24% and 28%, respectively and for central volume of distribution were 16% and 55%, respectively. The intra-subject variability in trastuzumab deruxtecan and DXd AUC values (area under the serum concentration versus time curve) was approximately 8% and 14%, respectively.
Special populations: Based on population pharmacokinetic analysis, age (20-96 years), race, ethnicity, sex and body weight did not have a clinically meaningful effect on exposure of trastuzumab deruxtecan or released DXd.
Elderly: The population PK analysis showed that age (range: 20-96 years) did not affect the PK of trastuzumab deruxtecan.
Renal impairment: No dedicated renal impairment study was conducted. Based on population pharmacokinetic analysis including patients with mild (creatinine clearance [CLcr] ≥60 and <90 mL/min) or moderate (CLcr ≥30 and <60 mL/min) renal impairment (estimated by Cockcroft-Gault), the pharmacokinetics of the released DXd was not affected by mild or moderate renal impairment as compared to normal renal function (CLcr ≥90 mL/min).
Hepatic impairment: No dedicated hepatic impairment study was conducted. Based on population pharmacokinetic analysis, the impact of changes on pharmacokinetics of trastuzumab deruxtecan in patients with total bilirubin ≤1.5 times ULN, irrespective of AST level, is not clinically meaningful. There are insufficient data for patients with total bilirubin >1.5 to 3 times ULN, irrespective of AST level, to draw conclusions, and no data is available for patients with total bilirubin >3 times ULN, irrespective of AST level (see Dosage & Administration and Precautions).
Paediatric population: No studies have been conducted to investigate the pharmacokinetics of trastuzumab deruxtecan in children or adolescents.
Toxicology: Preclinical safety data: In animals, toxicities were observed in lymphatic and haematopoietic organs, intestines, kidneys, lungs, testes and skin following the administration of trastuzumab deruxtecan at exposure levels of the topoisomerase I inhibitor (DXd) below clinical plasma exposure. In these animals, antibody-drug conjugate (ADC) exposure levels were similar or above clinical plasma exposure.
DXd was clastogenic in both an in vivo rat bone marrow micronucleus assay and an in vitro Chinese hamster lung chromosome aberration assay and was not mutagenic in an in vitro bacterial reverse mutation assay.
Carcinogenicity studies have not been conducted with trastuzumab deruxtecan.
Dedicated fertility studies have not been conducted with trastuzumab deruxtecan. Based on results from general animal toxicity studies, trastuzumab deruxtecan may impair male reproductive function and fertility.
There were no animal reproductive or developmental toxicity studies conducted with trastuzumab deruxtecan. Based on results from general animal toxicity studies, trastuzumab deruxtecan and DXd were toxic to rapidly dividing cells (lymphatic/haematopoietic organs, intestine, or testes), and DXd was genotoxic, suggesting the potential for embryotoxicity and teratogenicity.