Each 5 mL of prefilled syringe contains Fulvestrant 250 mg, Benzyl alcohol 10% w/v, Alcohol (Ethanol 96%) 10% w/v, Benzyl Benzoate 15% w/v, Castor Oil q.s.
Pharmacology: Many breast cancers have estrogen receptors, and the growth of these tumors can be stimulated by estrogen. Fulvestrant is an estrogen receptor antagonist that binds to the estrogen receptor in a competitive manner with affinity comparable to that of estradiol. Fulvestrant downregulates the estrogen receptor protein in human breast cancer cells.
In vitro studies demonstrated that fulvestrant is a reversible inhibitor of the growth of tamoxifen-resistant, as well as estrogen-sensitive human breast cancer (MCF-7) cell lines. In in vivo tumor studies, fulvestrant delayed the establishment of tumors from xenografts of human breast cancer MCF-7 cells in nude mice. Fulvestrant inhibited the growth of established MCF-7 xenografts and of tamoxifen-resistant breast tumor xenografts.
Pharmacodynamics: In a clinical study in postmenopausal women with primary breast cancer treated with single doses of fulvestrant 15-22 days prior to surgery, there was evidence of increasing downregulation of estrogen receptor with increasing dose. This was associated with a dose-related decrease in the expression of the progesterone receptor, an estrogen-regulated protein. These effects on the estrogen receptor pathway were also associated with a decrease in Ki67 labeling index, a marker of cell proliferation.
Pharmacokinetics: Absorption: After administration of fulvestrant long-acting intramuscular injection, fulvestrant is slowly absorbed and maximum plasma concentrations (Cmax) are reached after about 5 days. Administration of fulvestrant 500 mg regimen achieves exposure levels at, or close to, steady state within the first month of dosing (mean [CV]: AUC 475 [33.4%] ng·days/ml, Cmax 25.1 [35.3%] ng/ml, Cmin 16.3 [25.9%] ng/ml, respectively). At steady state, fulvestrant plasma concentrations are maintained within a relatively narrow range with up to an approximately 3-fold difference between maximum and trough concentrations. After intramuscular administration, the exposure is approximately dose proportional in the dose range 50 to 500 mg.
Distribution: Fulvestrant is subject to extensive and rapid distribution. The large apparent volume of distribution at steady state (Vdss) of approximately 3 to 5 l/kg suggests that distribution is largely extravascular. Fulvestrant is highly (99%) bound to plasma proteins. Very low density lipoprotein (VLDL), low density lipoprotein (LDL), and high density lipoprotein (HDL) fractions are the major binding components. No interaction studies were conducted on competitive protein binding. The role of sex hormone-binding globulin (SHBG) has not been determined.
Metabolism: The metabolism of fulvestrant has not been fully evaluated, but involves combinations of a number of possible biotransformation pathways analogous to those of endogenous steroids. Identified metabolites (includes 17-ketone, sulphone, 3-sulphate, 3- and 17-glucuronide metabolites) are either less active or exhibit similar activity to fulvestrant in anti-oestrogen models. Studies using human liver preparations and recombinant human enzymes indicate that CYP3A4 is the only P450 isoenzyme involved in the oxidation of fulvestrant, however, non-P450 routes appear to be more predominant in vivo. In vitro data suggest that fulvestrant does not inhibit CYP450 isoenzymes.
Elimination: Fulvestrant is eliminated mainly in metabolised form. The major route of excretion is via the faeces, with less than 1% being excreted in the urine. Fulvestrant has a high clearance, 11±1.7 ml/min/kg, suggesting a high hepatic extraction ratio. The terminal half-life (t½) after intramuscular administration is governed by the absorption rate and was estimated to be 50 days.
Special populations: In a population pharmacokinetic analysis of data from phase 3 studies, no difference in fulvestrant pharmacokinetic profile was detected with regard to age (range 33 to 89 years), weight (40-127 kg) or race.
Renal impairment: Mild to moderate impairment of renal function did not influence the pharmacokinetics of fulvestrant to any clinically relevant extent.
Hepatic impairment: The pharmacokinetics of fulvestrant has been evaluated in a single-dose clinical study conducted in women with mild to moderate hepatic impairment (Child-Pugh class A and B). A high dose of a shorter duration intramuscular injection formulation was used. There was up to about 2.5-fold increase in AUC in women with hepatic impairment compared to healthy women. In patients administered fulvestrant, an increase in exposure of this magnitude is expected to be well tolerated. Women with severe hepatic impairment (Child-Pugh class C) were not evaluated.
Fulvestrant is indicated as monotherapy for the treatment of estrogen receptor positive, locally advanced or metastatic breast cancer in postmenopausal women not previously treated with endocrine therapy, or with disease relapse on or after adjuvant anti-estrogen therapy, or disease progression on anti-estrogen therapy.
In combination with palbociclib for the treatment of hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative locally advanced or metastatic breast cancer in women who have received prior endocrine therapy.
In pre- or perimenopausal women, the combination treatment with palbociclib should be combined with a luteinizing hormone releasing hormone (LHRH) agonist.
Adult females (including the elderly): The recommended dose is 500 mg at intervals of one month, with an additional 500 mg dose given two weeks after the initial dose.
When fulvestrant is used in combination with palbociclib, please also refer to the prescribing information of palbociclib.
Prior to the start of treatment with the combination of fulvestrant plus palbociclib, and throughout its duration, pre/perimenopausal women should be treated with LHRH agonists according to local clinical practice.
Paediatric patient: Fulvestrant is not recommended for use in children or adolescents, as safety and efficacy have not been established in this age group.
Renal Impairment: No dose adjustments are recommended for patients with mild to moderate renal impairment (creatinine clearance ≥ 30 ml/min). Safety and efficacy have not been evaluated in patients with severe renal impairment (creatinine clearance < 30 ml/min), and, therefore, caution is recommended in these patients.
Hepatic Impairment: No dose adjustments are recommended for patients with mild to moderate hepatic impairment. However, as fulvestrant exposure may be increased, fulvestrant should be used with caution in these patients. There are no data in patients with severe hepatic impairment.
MODE OF ADMINISTRATION: Fulvestrant should be administered as two consecutive 5 ml injections by slow intramuscular injection (1-2 minutes/injection), one in each buttock (gluteal area).
Caution should be taken if injecting fulvestrant at the dorsogluteal site due to the proximity of the underlying sciatic nerve.
For detailed instructions for administration, see Special precautions for disposal and other handling under Cautions for Usage.
There are isolated reports of overdose with fulvestrant in humans. If overdose occurs, symptomatic supportive treatment is recommended. Animal studies suggest that no effects other than those related directly or indirectly to antiestrogenic activity were evident with higher doses of fulvestrant.
Hypersensitivity to the active substance (fulvestrant), or to any of the excipients e.g. Benzyl alcohol, Alcohol (Ethanol 96%), Benzyl benzoate and Castor oil.
Pregnancy and lactation.
Severe hepatic impairment.
Fulvestrant should be used with caution in patients with mild to moderate hepatic impairment. Fulvestrant should be used with caution in patients with severe renal impairment (creatinine clearance < 30 ml/min).
Due to the intramuscular route of administration, fulvestrant should be used with caution if treating patients with bleeding diatheses, thrombocytopenia or those taking anticoagulant treatment.
Thromboembolic events are commonly observed in women with advanced breast cancer and have been observed in clinical studies with fulvestrant. This should be taken into consideration when prescribing fulvestrant to patients at risk.
Injection site related events including sciatica, neuralgia, neuropathic pain, and peripheral neuropathy have been reported with fulvestrant injection. Caution should be taken while administering fulvestrant at the dorsogluteal injection site due to the proximity of the underlying sciatic nerve.
There are no long-term data on the effect of fulvestrant on bone. Due to the mechanism of action of fulvestrant, there is a potential risk of osteoporosis.
The efficacy and safety of fulvestrant (either as monotherapy or in combination with palbociclib) have not been studied in patients with critical visceral disease.
When fulvestrant is combined with palbociclib, please also refer to the prescribing information of palbociclib.
Interference with estradiol antibody assays: Due to the structural similarity of fulvestrant and estradiol, fulvestrant may interfere with antibody based-estradiol assays and may result in falsely increased level of estradiol.
EFFECTS ON ABILITY TO DRIVE AND USE MACHINES: Fulvestrant has no or negligible influence on the ability to drive or use machines. However, since asthenia has been reported very commonly with fulvestrant, caution should be observed by those patients who experience this adverse reaction when driving or operating machinery.
Women of childbearing potential: Patients of childbearing potential should be advised to use effective contraception while on treatment.
Pregnancy: Fulvestrant is contraindicated in pregnancy. Fulvestrant has been shown to cross the placenta after single intramuscular doses in rat and rabbit. Studies in animals have shown reproductive toxicity including an increased incidence of foetal abnormalities and deaths. If pregnancy occurs while taking fulvestrant, the patient must be informed of the potential hazard to the foetus and potential risk for loss of pregnancy.
Breast-feeding: Breast-feeding must be discontinued during treatment with fulvestrant. Fulvestrant is excreted in milk in lactating rats. It is not known whether fulvestrant is excreted in human milk. Considering the potential for serious adverse reactions due to fulvestrant in breast-fed infants, use during lactation is contraindicated.
Fertility: The effects of fulvestrant on fertility in humans has not been studied.
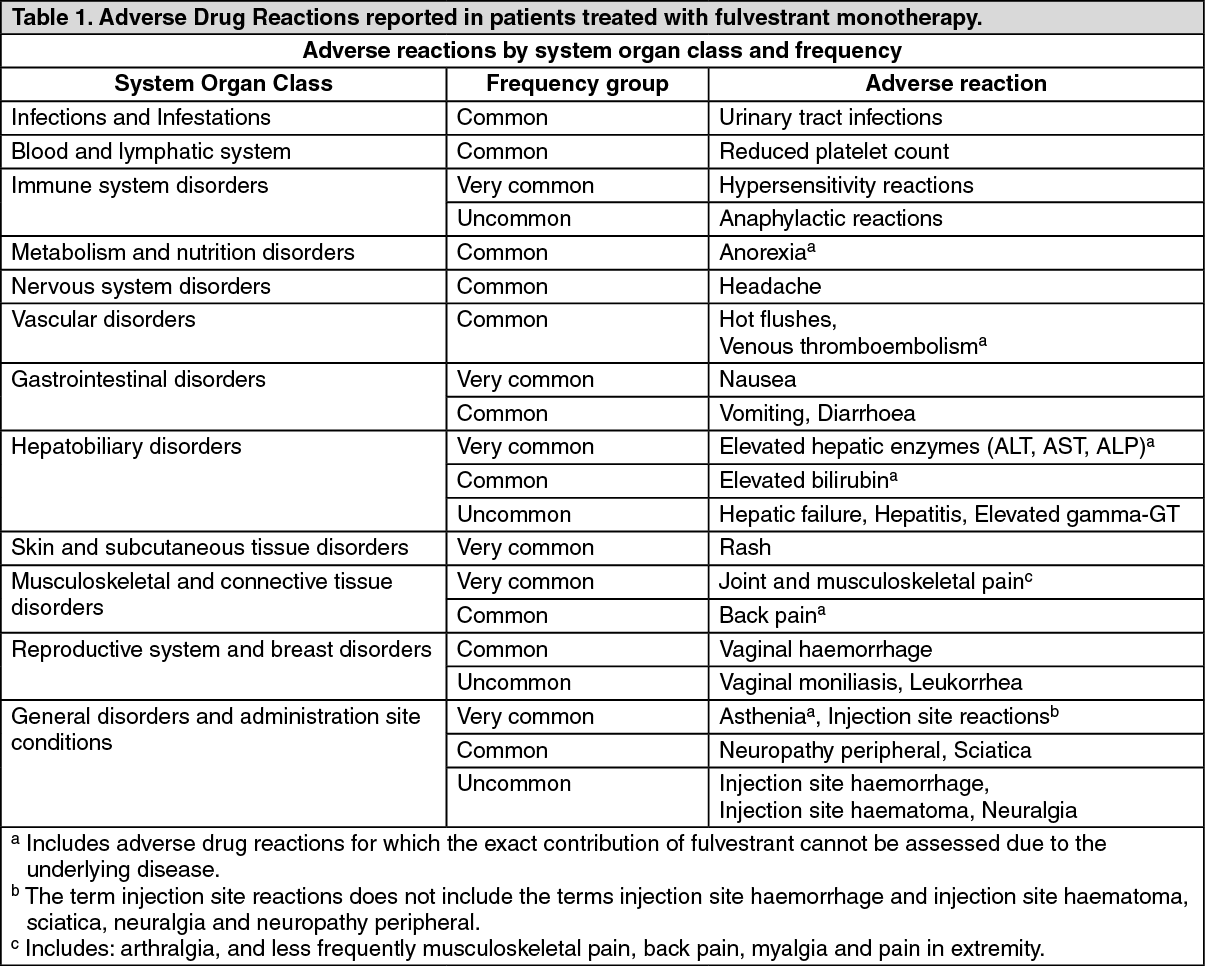
Monotherapy: In the pooled dataset of fulvestrant monotherapy, the most frequently reported adverse reactions were injection site reactions, asthenia, nausea, and increased hepatic enzymes (ALT, AST, ALP).
Tabulated list of adverse reactions: Adverse reactions listed as follows are classified according to frequency and System Organ Class (SOC). Frequency groupings are defined according to the following convention: Very common (≥ 1/10), Common (≥ 1/100 to < 1/10), Uncommon (≥ 1/1,000 to < 1/100). Within each frequency grouping adverse reactions are reported in order of decreasing seriousness. (See Table 1.)
 Click on icon to see table/diagram/image
Combination therapy with palbociclib:
Click on icon to see table/diagram/image
Combination therapy with palbociclib: The most common (≥ 20%) adverse reactions of any grade reported in patients receiving fulvestrant in combination with palbociclib were neutropenia, leukopenia, infections, fatigue, nausea, anaemia, stomatitis, diarrhoea, and thrombocytopenia.
The most common (≥ 2%) Grade ≥ 3 adverse reactions were neutropenia, leukopenia, anaemia, infections, AST increased, thrombocytopenia and fatigue. (See Table 2.)
Click on icon to see table/diagram/image
A clinical interaction study of fulvestrant with midazolam (substrate of CYP 3A4) demonstrated that fulvestrant does not inhibit CYP 3A4.
Clinical interaction studies of fulvestrant with rifampicin (inducer of CYP 3A4) and ketoconazole (inhibitor of CYP 3A4) showed no clinically relevant change in fulvestrant clearance.
Dose adjustment is therefore not necessary in patients who are receiving fulvestrant and CYP 3A4 inhibitors or inducers concomitantly.
SPECIAL PRECAUTIONS FOR DISPOSAL AND OTHER HANDLING: Instructions for administration: Administer the injection according to local guidelines for performing large volume intramuscular injections.
NOTE: Due to the proximity of the underlying sciatic nerve, caution should be taken if administering fulvestrant at the dorsogluteal injection site (see Precautions).
Warning: Do not autoclave safety needle before use. Hands must remain behind the needle at all times during use and disposal.
For each of the two syringes: Remove glass syringe barrel from blister tray and check that it is not damaged.
Peel open the safety needle (Terumo SurGuard) outer packaging.
Hold the syringe upright on the ribbed part. With the other hand, take hold of the cap and carefully tilt back and forth until the cap disconnects and can be pulled off. Remove the cap. To maintain sterility do not touch the syringe tip.
Attach the safety needle to the Luer-Lok and twist until firmly seated.
Check the needle is locked to the Luer connector.
Transport filled syringe to point of administration.
Move the safety sheath away from the needle and toward the syringe barrel, prior to removing the needle cap.
Parenteral solutions must be inspected visually for particulate matter and discolouration prior to administration.
Remove the needle cap. Pull shield straight off needle to avoid damaging needle point.
Expel excess gas from the syringe.
Administer intramuscularly slowly (1-2 minutes/injection) into the buttock. For user convenience, the needle bevel-up position is oriented to the lever arm.
After injection, use a one-handed technique to activate the safety mechanism using any of the two methods. (Activation is verified by an audible and/or tactile "click" and can be visually confirmed.)
NOTE: Activate away from self and others. Listen for click and visually confirm needle tip is fully covered.
Disposal: Pre-filled syringes are for single use only.
Any unused product or waste material should be disposed of in accordance with local requirements.
Store in a refrigerator (2°C to 8°C). Do not freeze.
Store the pre-filled syringe in the original package in order to protect from light.
L02BA03 - fulvestrant ; Belongs to the class of anti-estrogens. Used in treatment of neoplastic diseases.
Eranfu soln for inj 250 mg/5 mL
2 × 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image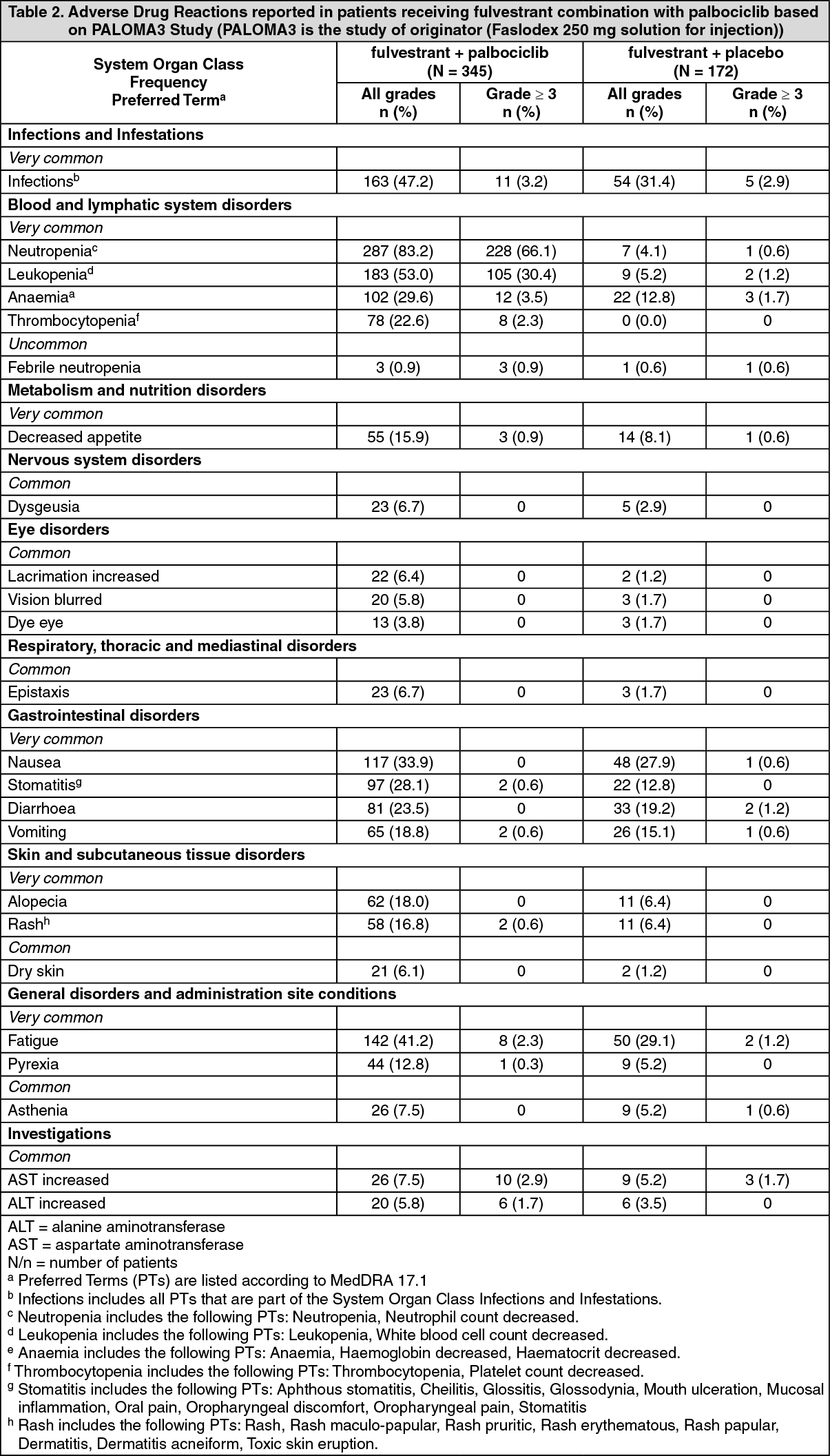 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
