The Erythropoiesis-stimulation agents (ESAs) may increase the risk of Serious Adverse Events, for example Hypertension, Lack of effect/efficacy (LOE), and Pure Red Blood Cell Aplasia (PRCA)
An incidence of Thrombotic vascular events (TVEs) should be carefully weighed against the benefits to be derived from treatment with Epoetin alfa particularly in patients with pre-existing risk factors for TVEs, including obesity and prior history of TVEs (Eg., deep venous thrombosis, pulmonary embolism and also the cancer patients
Pure Red Blood Cell Aplasia (PRCA): In Thailand have high report of Antibody-mediated pure red blood cell aplasia (PRCA) after administering Epoetin subcutaneous route in long term use of chronic renal failure patients. And also have an incidence of Pure Red Blood Cell Aplasia (PRCA) in patients with hepatitis C with interferon and ribavirin, when the erythropoiesis-stimulating agents (ESAs) are used concomitantly.
In chronic renal failure patients developing sudden lack of efficacy with decrease of hemoglobin and need for transfusion, a reticulocyte count should be obtained, and typical causes of non-response should be investigated. In case reticulocyte index less than 20,000/microliter or less than 0.5% with normal platelets and white blood cells the anti-erythropoietin antibodies and bone marrow testing should be performed to investigate the PRCA.
In case of PRCA patients should prompt to discontinue treatment with Epoetin and other ESA therapy because of the risk of cross-reaction.
Shock: Because shock may occur in rare case, sufficient monitoring should be made and if abnormality is recognized, the administration should be discontinued and proper treatments should be made.
Circulatory System: Rise in blood pressure, thrombosis of blood vessel contact region such as lachrymal duct and so on, and sometimes tachycardia may occur.
Hypertensive encephalopathy: Since hypertensive encephalopathy showing headache, consciousness disorder, seizure etc caused by sudden rise in the blood pressure is observed and cerebral hemorrhage may occur, administer with sufficient care monitoring the trend of blood pressure, hematocrit and so on.
Encephalopathy: as encephalopathy may occur, observe sufficiently and administration should be discontinued and appropriate treatment should be made in case abnormality is recognized.
Skin: Itch, rash, acne and so on may sometimes occur.
Liver: Hepatosis including AST, ALT, LDH, ALP, Total bilirubin, etc may sometimes occur. Abdominal pain can also occur.
Digestive system: Nausea, vomiting, anorexia, and diarrhea may sometimes occur. Abdominal pain can also occur.
Blood: Increase in leukocyte and eosinophil may sometimes occur. Decrease in granulocyte may sometimes occur in prematures. Serum potassium, BUN, creatinine and uric acid may sometimes increase. Rickets may sometimes occur in prematures. Incidence of Pure Red Cell Aplasia (PRCA) has been rarely reported among CRF patients with administration of erythropoietin preparation from months to years.
The others: Eyeground hemorrhage, splenomegaly, nasal hemorrhage, sometimes headache, dizziness, pyrexia, slight fever, feeling of flush, malaise, arthralgia, myalgia, bitter taste of mouth, convulsion and blepharedema may occur.
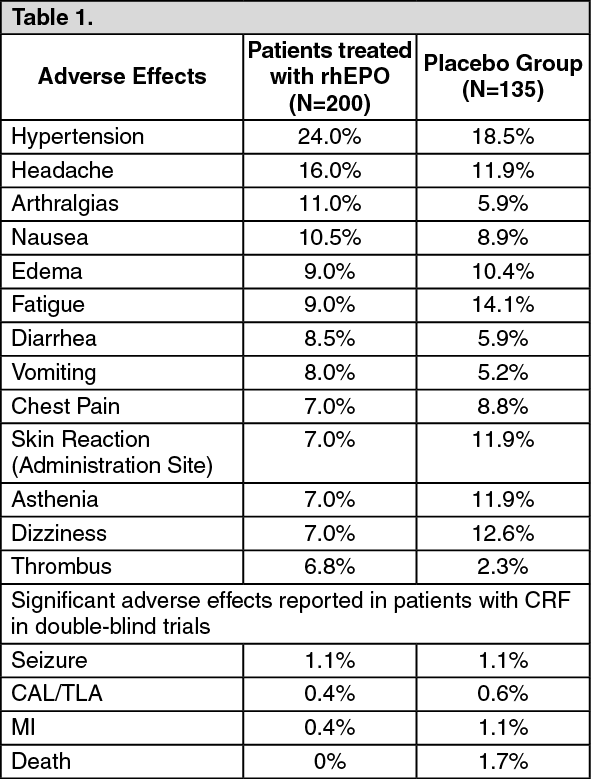
Espogen is generally well-tolerated. The adverse effects reported are frequent sequelae of CRF and may not necessarily attributable to erythropoietin therapy.
Chronic renal failure (CRF) patients: In double-blind, placebo-controlled studies involving over 300 patients with CRF, the events reported in greater than 5% of patients are as following table. (See Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In the clinical trials involving 567 patients on dialysis, the adverse effect reported most frequently were hypertension (0.75%), headache (0.40%), tachycardia (0.31%), nausea and vomiting (0.26%), clotted vascular access (0.25%), shortness of breath (0.14%), hyperkalemia (0.11%) and diarrhea. Other reported events occurred at a rate of less than 0.10% per patient per year. Events reported to have occurred within several hours of administration of rhEPO were rare, mild, and transient, and included flu-like symptoms such as arthralgias and myalgias. In all studies analyzed to date, rhEPO administration was generally well-tolerated irrespective of the route of administration.
Cancer patients: In double-blind, placebo-controlled studies of up to 3 months duration involving 131 cancer patients, adverse effects with an incidence of greater than 10% are as following table. (See Table 2.)
Click on icon to see table/diagram/image
Although some statistically significant difference between patients treated with rhEPO and placebo were noted, the overall adverse effects reported were consistent with the disease process of cancer. Even in a clinical trial in which patients (N = 72) were treated for up to 32 weeks with doses as high as 927U/kg, the adverse effects reported were consistent with progression of cancer. Based on comparable survival data, and on the percentage of patients treated with rhEPO and placebo who discontinued therapy due to death, disease progression or adverse effects (22% and 13%, respectively), the clinical results between two groups appeared to be similar. Available data from animal tumor models and measurement of proliferation of solid tumor cells from clinical biopsy specimens in response to rhEPO suggests rhEPO doesn't accelerate tumor growth. Nevertheless, the possibility the rhEPO may promote growth of some tumors, particularly myeloid tumors, cannot be excluded. A randomized comparative phase IV clinical trial is currently ongoing for further evaluation of this issue. The mean peripheral white blood cell count was unchanged following rhEPO therapy compared to placebo-treated group.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image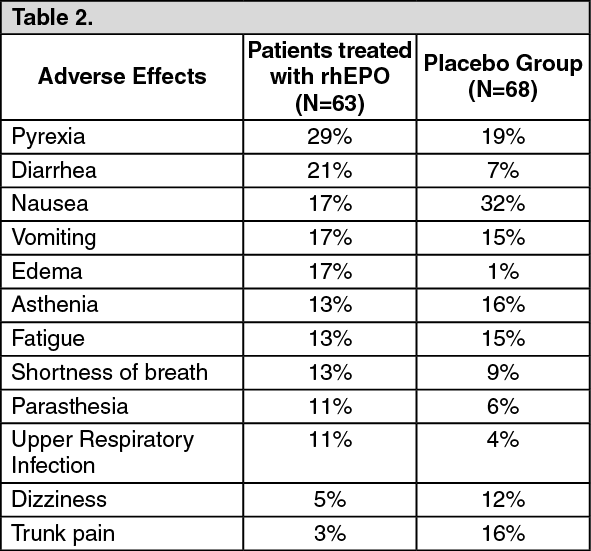 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out