Pharmacology: Pharmacodynamics: Mechanism of action: Favipiravir is a prodrug that is metabolized in cells to the active form favipiravir-ribosyl triphosphate form (favipiravir RTP), which selectively inhibits RNA polymerase involved in viral replication. Inhibitory concentration (IC
50) of favipiravir RTP on human RNA polymerase II was 905 μmol/L.
Pharmacodynamic effects: In vitro antiviral activity: Favipiravir showed antiviral activity against type A and type B influenza virus laboratory strains with an EC50 of 0.014-0.55 μg/mL.
The EC
50 against seasonal type A and type B influenza viruses including strains resistant to adamantane (amantadine and rimantadine), oseltamivir or zanamivir was 0.03-0.94 and 0.09-0.83 μg/mL, respectively.
The EC
50 against type A influenza viruses (including strains resistant to adamantane, oseltamivir or zanamivir) such as swine-origin type A and avian-origin type A including highly-pathogenic strains (including H5N1 and H7N9) was 0.06-3.53 μg/mL.
The EC
50 against type A and type B influenza viruses resistant to adamantane, oseltamivir and zanamivir was 0.09-0.47 μg/mL, and no cross resistance was observed.
Therapeutic effect in animal models: In mouse infection models inoculated with influenza viruses A (H7N9), A (H1N1) pdm09 or A (H3N2), decrease of virus titers in lung tissues was observed by a 5-day oral administration of favipiravir with a dose of 60 mg/kg/day. In mouse infection models inoculated with influenza viruses A (H3N2) or A (H5N1), therapeutic effect was observed by a 5-day oral administration of favipiravir with a dose of 30 mg/kg/day.
In a SCID mouse infection model inoculated with an influenza virus A (H3N2), therapeutic effect was observed by a 14-day oral administration of favipiravir with a dose of 30 mg/kg/day.
Resistance: No change of susceptibility of type A influenza viruses to favipiravir was observed after 30 passages in the presence of favipiravir, and no resistant viruses have been selected. In clinical studies including the global phase III study, information about emergence of favipiravir - resistant influenza viruses has not been obtained.
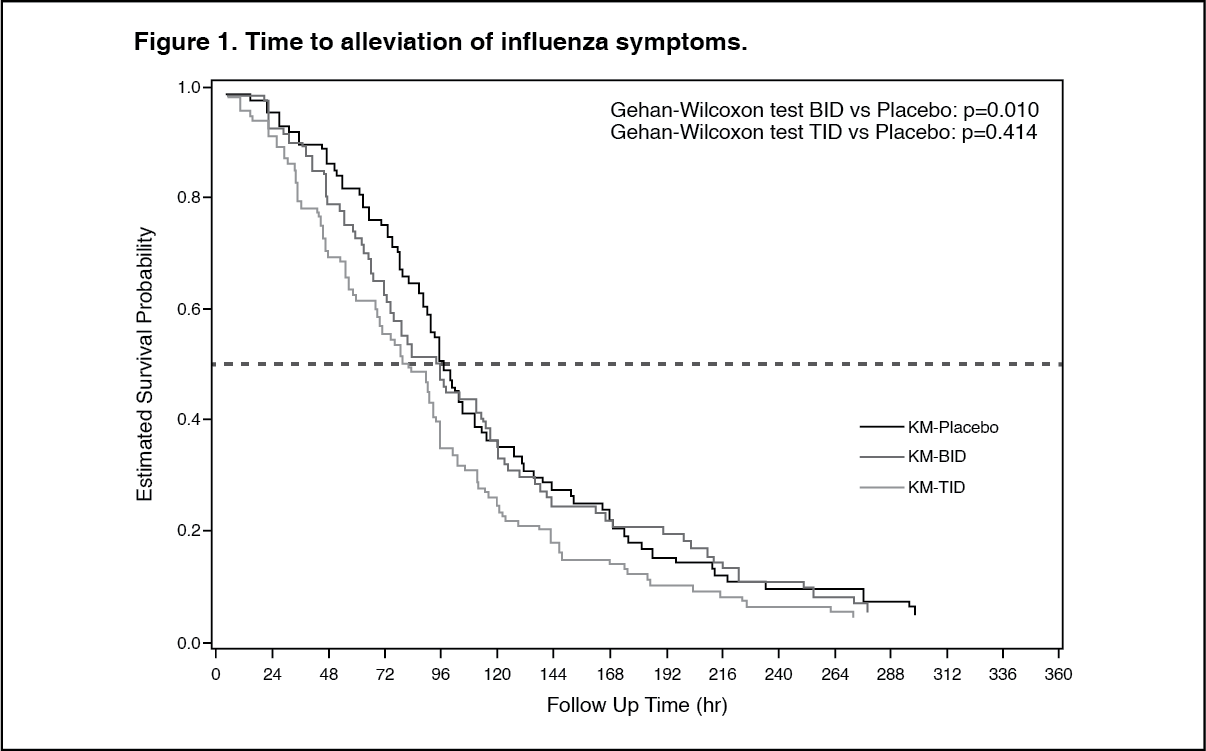
CLINICAL STUDIES: Results in non-Japanese: A placebo-controlled phase I/II study in type A or type B influenza patients was conducted (1800 mg/800 mg BID, oral administration of favipiravir 1800 mg twice daily for 1 day followed by 800 mg twice daily for 4 days; 2400 mg/600 mg TID, oral administration of favipiravir 2400mg + 600 mg + 600 mg for 1 day followed by 600 mg three times daily for 4 days)
Note 1. With regards to the primary endpoint
Note 2, favipiravir 1800 mg/800 mg BID (101 patients) demonstrated significant difference in time to alleviation of influenza symptoms compared to placebo (88 patients) (p=0.01, Gehan-Wilcoxon test), but favipiravir 2400 mg/600 mg TID (82 patients) failed to demonstrate significant difference (p=0.414, Gehan-Wilcoxon test). (See Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Note 1: The approved dosage of favipiravir is "1600 mg orally twice daily for 1 day followed by 600 mg orally twice daily for 4 days".
Note 2: Time required to alleviate 6 primary influenza symptoms (cough, sore throat, headache, nasal congestion, body aches and pains, fatigue [tiredness]) and body temperature.
Two placebo-controlled phase III studies in type A or type B influenza patients (oral administration of favipiravir 1800 mg twice daily for 1 day followed by 800 mg twice daily for 4 days [1800 mg/800 mg BID])
Note 3 with the primary endpoint: the time required to alleviate primary influenza symptoms
Note 4, were conducted (Study 1 and Study 2). The results are as follows. (See Table 1, Figures 2 and 3.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Note 3: The approved dosage of favipiravir is "1600 mg orally twice daily for 1 day followed by 600 mg orally twice daily for 4 days".
Note 4: Time required to alleviate 6 primary influenza symptoms (cough, sore throat, headache, nasal congestion, body aches and pains, fatigue [tiredness]) and resolution of fever. Alleviation was defined as all of the 6 influenza symptoms had been either absent or mild and fever had resolved, with both maintained for at least 21.5 hours.
Note 5: Peto-Peto-Prentice test.
Reference: Global phase III clinical study (adults): A global phase III clinical study of favipiravir (the dosage
Note 6 was different from the approved dosage for adults) versus oseltamivir phosphate (75 mg twice daily for 5 days) was conducted in patients with type A or type B influenza (640 patients [467 patients in Japan, 55 patients in Korea, and 118 patients in Taiwan]). The median time (95% CI) to alleviation of primary influenza symptoms
Note 7 was 63.1 hours (55.5, 70.4) for favipiravir group (377 patients) and 51.2 hours (45.9, 57.6) for oseltamivir phosphate group (380 patients). The hazard ratio (95% CI) of favipiravir to oseltamivir phosphate for time to alleviation of primary influenza symptoms was 0.818 (0.707, 0.948), and the efficacy of favipiravir was not demonstrated (p=0.007, log-rank test).
Note 6: 1200 mg + 400 mg on Day 1 followed by 400 mg twice daily for 4 days. The approved dosage of favipiravir is "1600 mg orally twice daily for 1 day followed by 600 mg orally twice daily for 4 days".
Note 7: Time required for 7 primary influenza symptoms (cough, sore throat, headache, nasal congestion, feeling feverish, body aches and pains, fatigue (tiredness)) to alleviate after the start of study drug administration (the time point when all symptoms were scored 1 or below). "Alleviation" was defined as the state where all of the scores graded by the investigator based on the record of the patient diary remain unchanged for 21.5 hours or longer all of the scores decrease to 1 or below.
Reference: Phase II clinical study in non-Japanese (adults): A placebo-controlled phase II study of favipiravir was conducted in patients with type A or type B influenza (1000 mg/400 mg BID, oral administration of favipiravir 1000 mg twice daily for 1 day followed by 400 mg twice daily for 4 days; 1200 mg/800 mg BID, oral administration of favipiravir 1200 mg twice daily for 1 day followed by 800 mg twice daily for 4 days; placebo, twice daily)
Note 8. The median time (95% CI) to alleviation of primary influenza symptoms
Note 9 was 100.4 hours (82.4, 119.8) for 1000 mg/400 mg BID group (88 patients), 86.5 hours (79.2, 102.1) for 1200 mg/800 mg BID group (121 patients), and 91.9 hours (70.3, 105.4) for placebo group (124 patients). There was no statistically significant difference between either favipiravir group and placebo group (p>0.05, Gehan-Wilcoxon test; A step-down approach was used to regulate the overall type I error rate for the multiple comparisons).
Note 8: The approved dosage of favipiravir is "1600 mg orally twice daily for 1 day followed by 600 mg orally twice daily for 4 days".
Note 9: Time required to "alleviate" 6 primary influenza symptoms (cough, sore throat, headache, nasal congestion, body aches and pains, fatigue [tiredness]) and body temperature, where alleviation was defined as the state where all of the scores and temperature remain unchanged for 21.5 hours or longer after all of the scores decrease to 1 or below and temperature returned to less than 38.0°C for 20 to <65 years old and less than 37.8°C for patient ≥ 65 years old.
Pharmacokinetics: Absorption: Blood Concentrations: The following table shows pharmacokinetic parameters of favipiravir after an oral administration in 8 healthy adults at 1600 mg twice daily for 1 day, then 600 mg twice daily for 4 days followed by 600 mg once daily for 1 day (1600 mg/600 mg BID). (See Table 2 and Figure 4.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Following multiple oral administration of favipiravir for 7 days
Note 10 to a healthy adult who appeared to have little AO activity, the estimated AUC of unchanged drug was 1452.73 μg・hr/mL on Day 1 and 1324.09 μg・hr/mL on Day 7.
Note 10: 1200 mg + 400 mg on Day 1, then 400 mg twice daily on Days 2 to 6 followed by 400 mg once daily on Day 7. The approved dosage of favipiravir is "1600 mg orally twice daily for 1 day followed by 600 mg orally twice daily for 4 days".
Distribution: Results in non-Japanese: When favipiravir was orally administered to 20 healthy adult male subjects at 1200 mg twice daily for 1 day followed by 800 mg twice daily for 4 days (1200 mg/800 mg BID)
Note 11, the geometric mean concentration of the drug in semen was 18.341 μg/mL on Day 3, and 0.053 μg/mL on the second day after the treatment. These men levels became below the limit of quantification (0.02 μg/mL) in all subjects in 7 days after the end of the treatment. The mean ratio of the drug concentration in semen to that in plasma was 0.53 on Day 3 and 0.45 on the second day after the treatment.
Note 11: The approved dosage of favipiravir is "1600 mg orally twice daily for 1 day followed by 600 mg orally twice daily for 4 days".
The serum protein binding ratio was 53.4 to 54.4% (in vitro, centrifugal ultrafiltration).
Reference: Animal data: When a single dose of
14C-favipiravir was orally administered to monkeys, it was distributed broadly in tissues. Radioactivity of each tissue peaked in 0.5 hours after the administration and changed in parallel with the radioactivity in plasma. The ratio of radioactivity in lung tissues to that in plasma was 0.51 in 0.5 hours after the administration, and the drug was distributed rapidly to respiratory tissues which were considered infection site. Radioactivity in kidney was higher than that in plasma, with a ratio of 2.66. Radioactivity in each tissue, except bones, decreased to ≤ 2.8% of the peak within 24 hours after the administration.
Metabolism: Favipiravir is mostly metabolized by aldehyde oxidase (AO), and partly to a hydroxylated form by xanthine oxidase (XO). In studies using human liver microsomes, formation of the hydroxylate ranged from 3.98 to 47.6 pmol/mg protein/min, with an inter-individual variation of AO activity by 12 times at maximum. A glucuronate conjugate was observed in human plasma and urine as a metabolite other than the hydroxylated form.
Excretion: Favipiravir was mainly excreted as a hydroxylated form into the urine, and little amount unchanged drug was observed. In an oral 7 day
Note 12 multiple dose study with 6 healthy adults, cumulative urinary excretion ratio of the unchanged drug and the hydroxylated form was 0.8% and 53.1%, respectively, during 48 hours after the last administration.
Note 12: 1200 mg+ 400 mg on Day 1, then 400 mg twice daily on Days 2 to 6 followed by 400 mg once daily on Day 7. The approved dosage of favipiravir is "600 mg orally twice daily for 1 day followed by 600 mg orally twice daily for 4 days".
Specific Populations: Patients with Hepatic Impairment: When favipiravir was orally administered to subjects with mild and moderate liver function impairment (Child-Pugh classification A and B, 6 subjects each) at 1200 mg twice daily for 1 day followed by 800 mg twice daily for 4 days (1200 mg/800 mg BID), compared to healthy adult subjects, C
max and AUC at day 5 were approximately 1.6 fold and 1.7 fold, respectively in subjects with mild liver function impairment, and 1.4 fold and 1.8 fold, respectively in subjects with moderate liver function impairment.
When favipiravir was orally administered to subjects with severe liver function impairment (Child-Pugh classification C, 4 subjects) at 800 mg twice daily for 1 day followed by 400 mg twice daily for 2 days (800 mg/400 mg BID)
Note 13, compared to healthy adult subjects, C
max and AUC at day 3 were approximately 2.1 fold and 6.3 fold, respectively.
Note 13: The approved dosage of favipiravir is "1600mg orally twice daily for 1 day followed by 600 mg orally twice daily for 4 days".
Drug Interaction Studies: In vitro: Favipiravir inhibited irreversibly AO in a dose and time dependent manner, and inhibited CYP2C8 in a dose dependent manner. There were no inhibitory activity to XO, and weak inhibitory activity to CYP1A2, 2C9, 2C19, 2D6, 2E1 and 3A4. The hydroxylated metabolite showed weak inhibitory activity to CYP1A2, 2C8, 2C9, 2C19, 2D6, 2E1 and 3A4. Inductive effect of favipiravir on CYP was not observed.
Drug-drug Interaction Clinical Studies: Effects of co-administered drugs on pharmacokinetics of favipiravir: see Table 3.
Click on icon to see table/diagram/image
Effects of favipiravir on pharmacokinetics of co-administered drugs: see Table 4.
Click on icon to see table/diagram/image
Toxicology: Preclinical safety data: In pharmacokinetic study, when a single dose of
14C-favipiravir was orally administered to monkeys, it was distributed broadly in tissues. Radioactivity of each tissue peaked in 0.5 hours after the administration and changed in parallel with the radioactivity in plasma. The ratio of radioactivity in lung tissues to that in plasma was 0.51 in 0.5 hours after the administration, and the drug was distributed rapidly to respiratory tissues which were considered infection site. Radioactivity in kidney was higher than that in plasma, with a ratio of 2.66. Radioactivity in each tissue, except bones, decreased to ≤2.8% of the peak within 24 hours after the administration.
Juvenile Animal Study: In a one month study with juvenile dogs [8 weeks old], death cases have been reported after day 20 with a dosage [60 mg/kg/day] which was lower than the lethal dosage for young dogs [7 to 8 months old]. In juvenile animals [6-day-old rats and 8-week-old dogs], abnormal gait, atrophy and vacuolation of skeletal muscular fiber, degeneration/necrosis/mineralization of papillary muscle have been reported.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image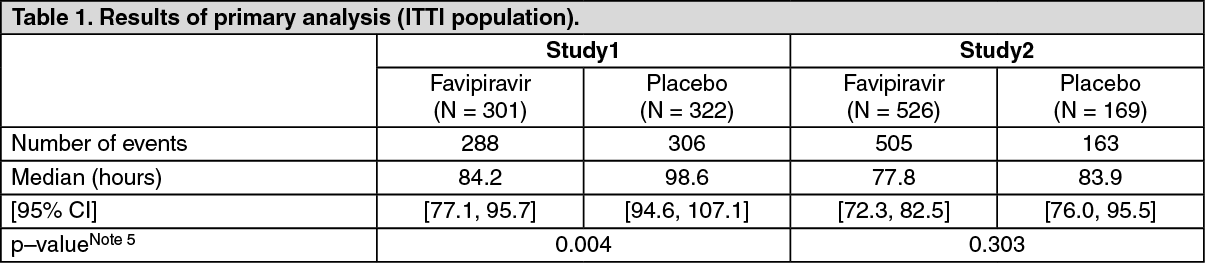 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image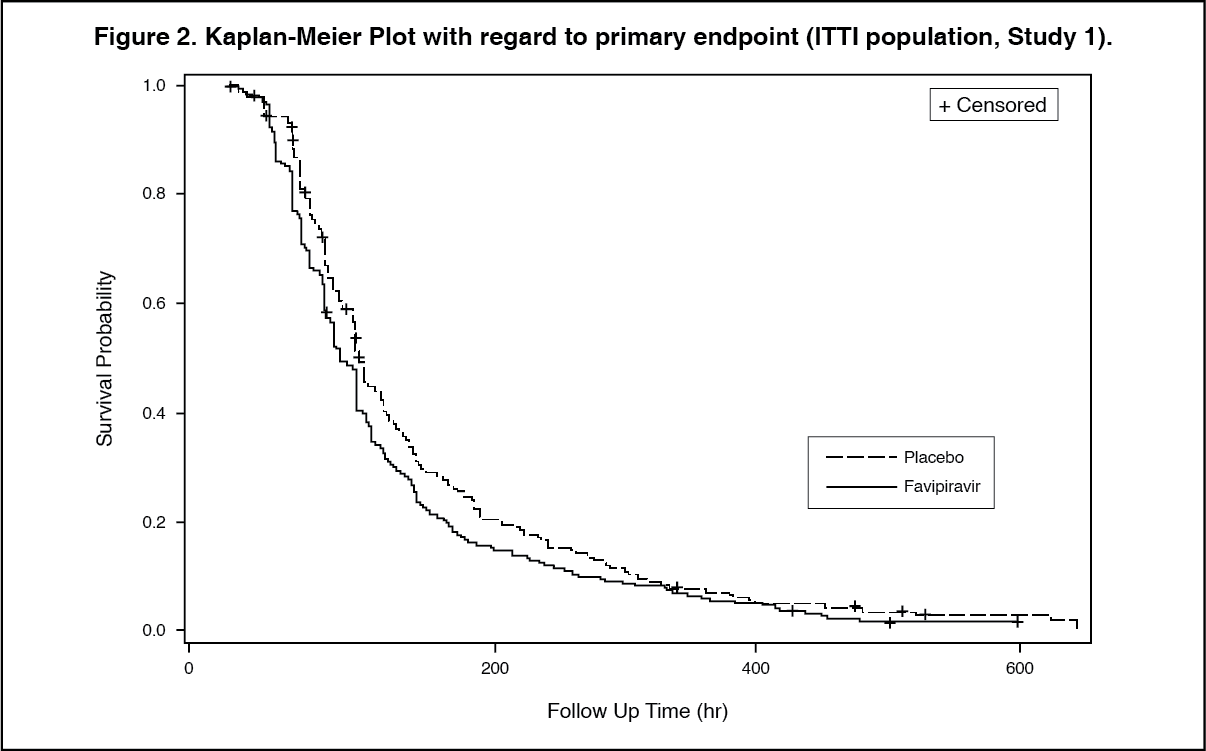 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image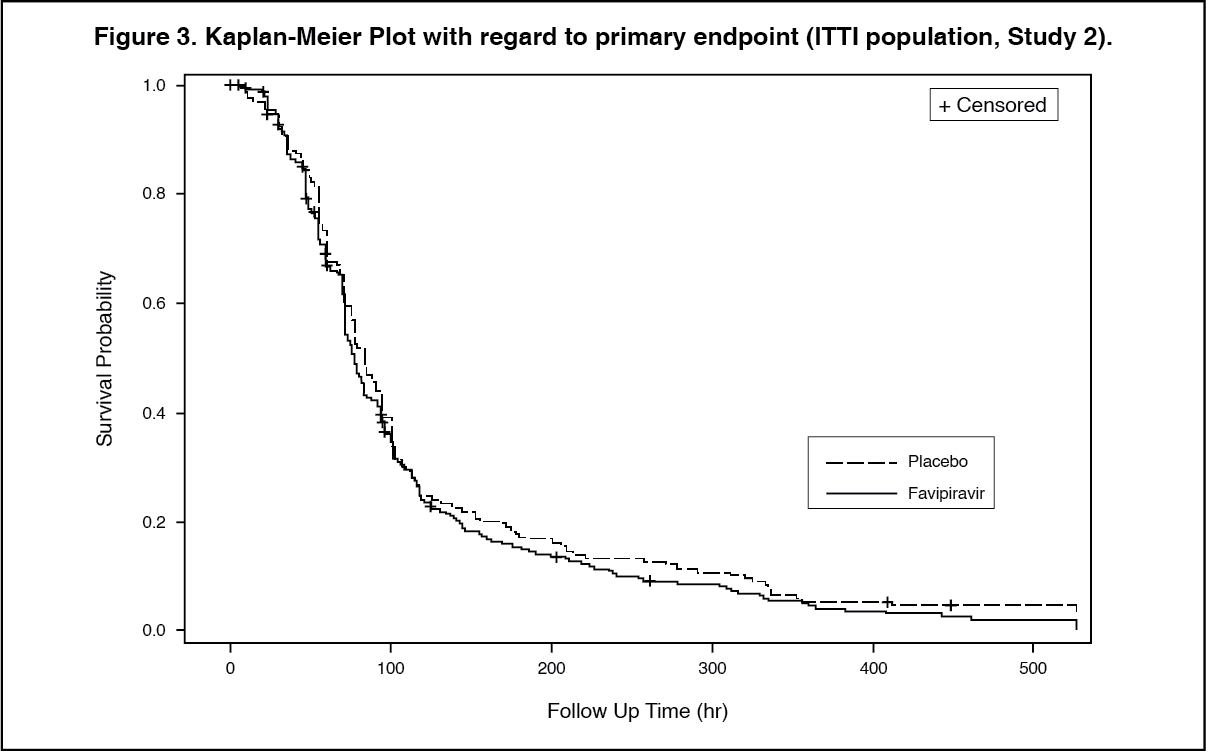 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image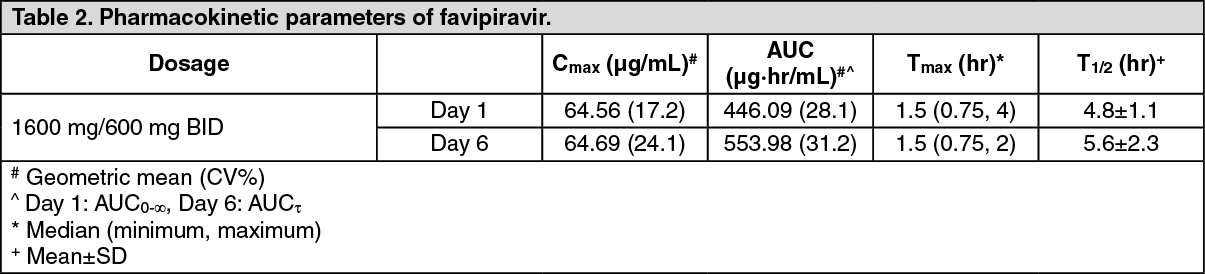 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image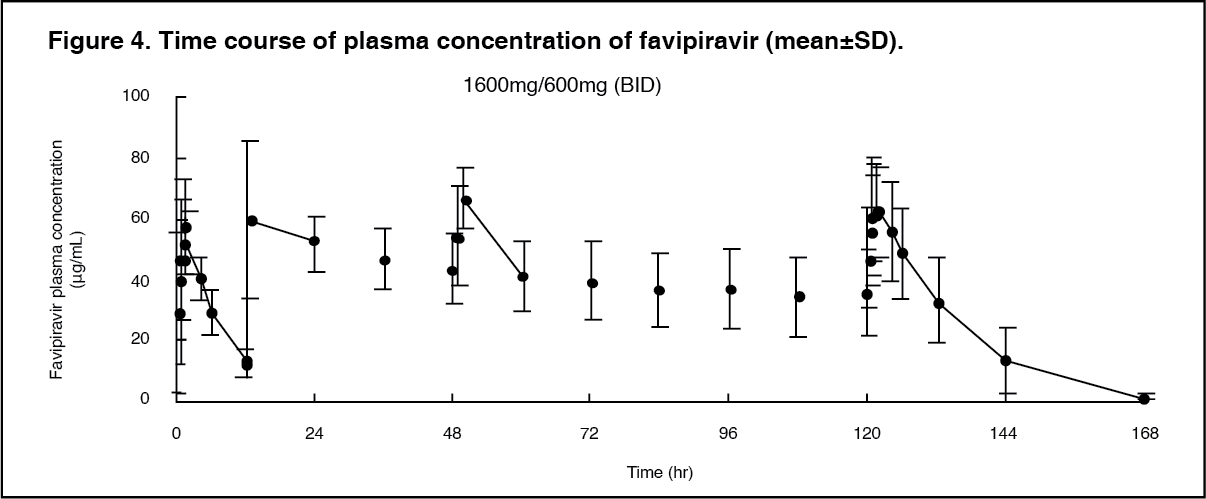 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image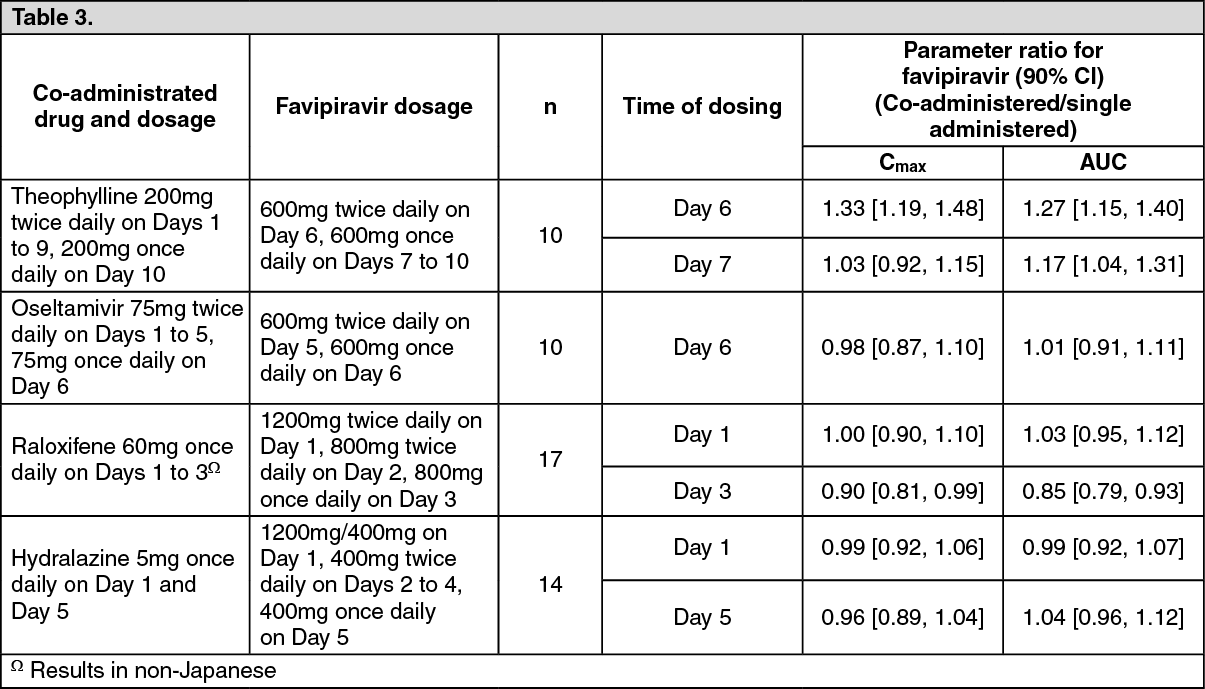 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image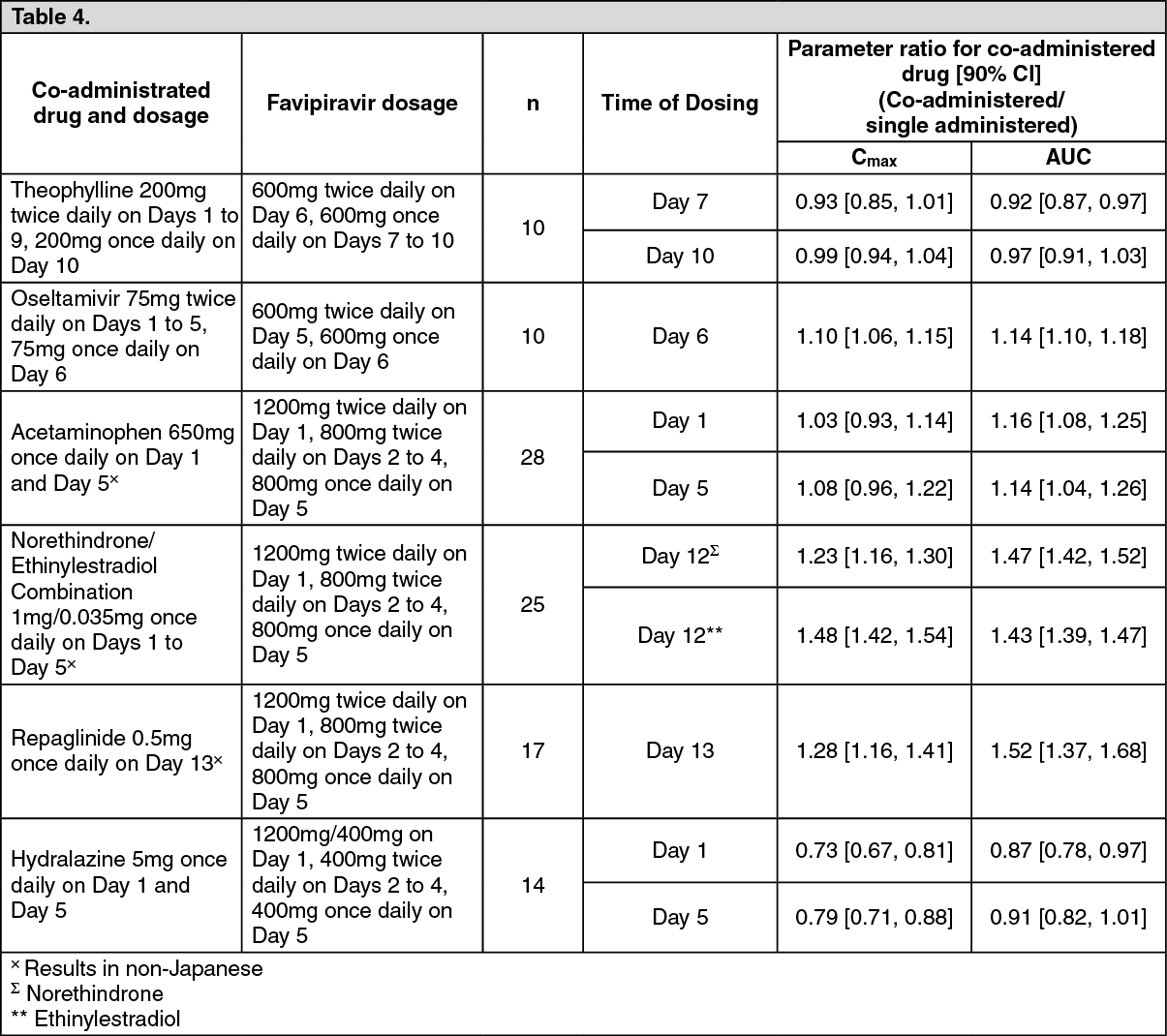 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image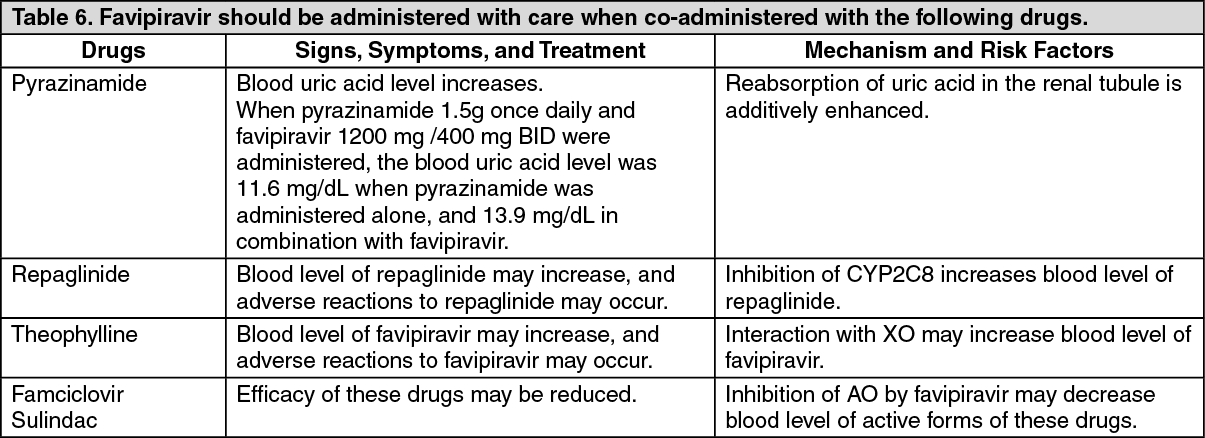 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out