PHARMACOLOGY: Mechanism of Action: Finerenone is a nonsteroidal, selective antagonist of the mineralocorticoid receptor (MR), which is activated by aldosterone and cortisol and regulates gene transcription. Finerenone blocks MR mediated sodium reabsorption and MR overactivation in both epithelial (e.g., kidney) and nonepithelial (e.g., heart, and blood vessels) tissues. MR overactivation is thought to contribute to fibrosis and inflammation. Finerenone has a high potency and selectivity for the MR and has no relevant affinity for androgen, progesterone, estrogen, and glucocorticoid receptors.
Pharmacodynamics: In FIDELIO-DKD, a randomized, double-blind, placebo-controlled, multicenter study in adult patients with chronic kidney disease associated with type 2 diabetes, the placebo-corrected relative reduction in urinary albumin-to-creatinine ratio (UACR) in patients randomized to finerenone was 31% at Month 4 (95% CI 29-34%) and remained stable for the duration of the trial.
In patients treated with Firialta, the mean systolic blood pressure decreased by 3 mmHg and the mean diastolic blood pressure decreased by 1-2 mmHg at month 1, remaining stable thereafter.
Cardiac Electrophysiology: At a dose 4 times the maximum approved recommended dose, finerenone does not prolong the QT interval to any clinically relevant extent.
CLINICAL STUDIES: The FIDELIO-DKD study was a randomized, double-blind, placebo-controlled, multicenter study in adult patients with chronic kidney disease (CKD) associated with type 2 diabetes (T2D), defined as either having an UACR of 30 to 300 mg/g, eGFR 25 to 60 mL/min/1.73 m
2 and diabetic retinopathy, or as having an UACR of ≥300 mg/g and an eGFR of 25 to 75 mL/min/1.73 m
2. The trial excluded patients with known significant non-diabetic kidney disease. All patients were to have a serum potassium ≤4.8 mEq/L at screening and be receiving standard of care background therapy, including a maximum tolerated labeled dose of an angiotensin-converting enzyme inhibitor (ACEi) or angiotensin receptor blocker (ARB). Patients with a clinical diagnosis of chronic heart failure with reduced ejection fraction and persistent symptoms (New York Heart Association class II to IV) were excluded. The starting dose of Firialta was based on screening eGFR (10 mg once daily in patients with an eGFR of 25 to <60 mL/min/1.73 m
2 and 20 mg once daily in patients with an eGFR ≥60 mL/min/1.73 m
2). The dose of Firialta could be titrated during the study, with a target dose of 20 mg daily.
The primary objective of the study was to determine whether Firialta reduced the incidence of a sustained decline in eGFR of ≥40%, kidney failure (defined as chronic dialysis, kidney transplantation, or a sustained decrease in eGFR to <15 mL/min/1.73m
2), or renal death.
A total of 5674 patients were randomized to receive Firialta (N=2833) or placebo (N=2841) and were followed for a median of 2.6 years. The mean age of the study population was 66 years, and 70% of patients were male. The trial population was 63% White, 25% Asian, and 5% Black. At baseline, the mean eGFR was 44 mL/min/1.73m
2, with 55% of patients having an eGFR <45 mL/min/1.73m
2. Median urine albumin-to-creatinine ratio (UACR) was 852 mg/g, and mean glycated hemoglobin A1c (HbA1c) was 7.7%. Approximately 46% of patients had a history of atherosclerotic cardiovascular disease.
At baseline, 99.8% of patients were treated with an ACEi or ARB. Approximately 97% were on an antidiabetic agent (insulin [64.1%], biguanides [44%], glucagon-like peptide-1 [GLP-1] receptor agonists [7%], sodium-glucose cotransporter 2 [SGLT2] inhibitors [5%]), 74% were on a statin, and 57% were on an antiplatelet agent.
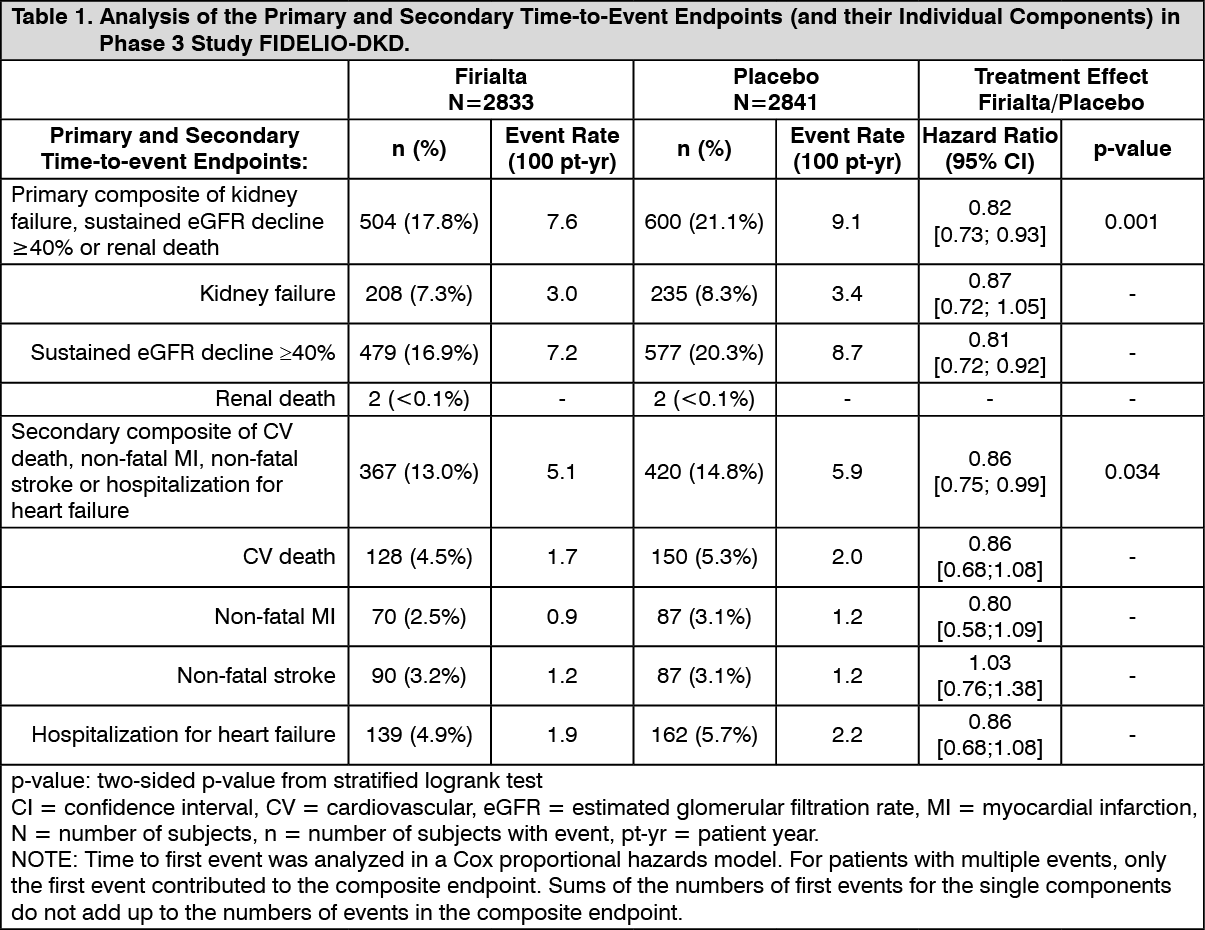
Firialta reduced the incidence of the primary composite endpoint of a sustained decline in eGFR of ≥40%, kidney failure, or renal death (HR 0.82, 95% CI 0.73-0.93, p=0.001) as shown in Table 1 and Figure 1. The treatment effect reflected a reduction in a sustained decline in eGFR of ≥40% and progression to kidney failure. There were few renal deaths during the trial.
Firialta also reduced the incidence of the composite endpoint of cardiovascular (CV) death, non-fatal myocardial infarction (MI), non-fatal stroke or hospitalization for heart failure (HR 0.86, 95% CI 0.75-0.99, p=0.034) as shown in Table 1 and Figure 2. The treatment effect reflected a reduction in CV death, non-fatal MI, and hospitalization for heart failure.
The treatment effect on the primary and secondary composite endpoints was generally consistent across subgroups. (See Table 1 and Figures 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics: Finerenone exposure increased proportionally over a dose range of 1.25 to 80 mg (0.06 to 4 times the maximum approved recommended dosage). Steady state of finerenone was achieved after 2 days of dosing. The estimated steady-state geometric mean C
max,md was 160 μg/L and steady-state geometric mean AUC
τ,md was 686 μg.h/L following administration of finerenone 20 mg to patients.
Absorption: Finerenone is completely absorbed after oral administration but undergoes metabolism resulting in absolute bioavailability of 44%. Finerenone C
max was achieved between 0.5 and 1.25 hours after dosing.
Effect of Food: There was no clinically significant effect on finerenone AUC following administration with high fat, high calorie food.
Distribution: The volume of distribution at steady-state (Vss) of finerenone is 52.6 L. Plasma protein binding of finerenone is 92%, primarily to serum albumin, in vitro.
Elimination: The terminal half-life of finerenone is about 2 to 3 hours, and the systemic blood clearance is about 25 L/h.
Metabolism: Finerenone is primarily metabolized by CYP3A4 (90%) and to a lesser extent by CYP2C8 (10%) to inactive metabolites.
Excretion: About 80% of the administered dose is excreted in urine (<1% as unchanged) and approximately 20% in feces (< 0.2% as unchanged).
Specific Populations: There are no clinically significant effects of age (18 to 79 years), sex, race/ethnicity (White, Asian, Black, and Hispanic), or weight (58 to 121 kg) on the pharmacokinetics of finerenone.
Renal Impairment: There were no clinically relevant differences in finerenone AUC or C
max values in patients with eGFR 15 to < 90 mL/min/1.73m
2 compared to eGFR ≥ 90 mL/min/1.73 m
2. For dosing recommendations based on eGFR and serum potassium levels see Dosage & Administration.
Hepatic Impairment: There was no clinically significant effect on finerenone exposure in cirrhotic patients with mild hepatic impairment (Child Pugh A).
Finerenone mean AUC was increased by 38% and C
max was unchanged in cirrhotic patients with moderate hepatic impairment (Child Pugh B) compared to healthy control subjects.
The effect of severe hepatic impairment (Child Pugh C) on finerenone exposure was not studied.
Drug Interaction Studies: Clinical Studies and Model-Informed Approaches: Strong CYP3A Inhibitors: Concomitant use of itraconazole (strong CYP3A4 inhibitor) increased finerenone AUC by >400%.
Moderate CYP3A Inhibitors: Concomitant use of erythromycin (moderate CYP3A4 inhibitor) increased finerenone mean AUC and C
max by 248% and 88%, respectively.
Weak CYP3A Inhibitors: Concomitant use of amiodarone (weak CYP3A4 inhibitor) increased finerenone AUC by 21%.
Strong or Moderate CYP3A Inducers: Concomitant use of efavirenz (moderate CYP3A4 inducer) and rifampicin (strong CYP3A4 inducer) decreased finerenone AUC by 80% and 90%, respectively.
Other Drugs: There was no clinically significant difference in finerenone pharmacokinetics when used concomitantly with gemfibrozil (strong CYP2C8 inhibitor), omeprazole (proton pump inhibitor), or an aluminium hydroxide and magnesium hydroxide antacid. There were no clinically significant pharmacokinetic differences for either finerenone or concomitant digoxin (P-gp substrate) or warfarin (CYP2C9 substrate). There were no clinically significant differences in the pharmacokinetics of either midazolam (CYP3A4 substrate) or repaglinide (CYP2C8 substrate) when used concomitantly with finerenone.
NONCLINICAL TOXICOLOGY: Carcinogenesis, Mutagenesis, Impairment of Fertility: Finerenone was non-genotoxic in an in vitro bacterial reverse mutation (Ames) assay, the in vitro chromosomal aberration assay in cultured Chinese hamster V79 cells, or the in vivo micronucleus assay in mice.
In 2-year carcinogenicity studies, finerenone did not show a statistically significant increase in tumor response in Wistar rats or in CD1 mice. In male mice, Leydig cell adenoma was numerically increased at a dose representing 26 times the AUC
unbound in humans and is not considered clinically relevant. Finerenone did not impair fertility in male rats but impaired fertility in female rats at 20 times AUC to the maximum human exposure.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image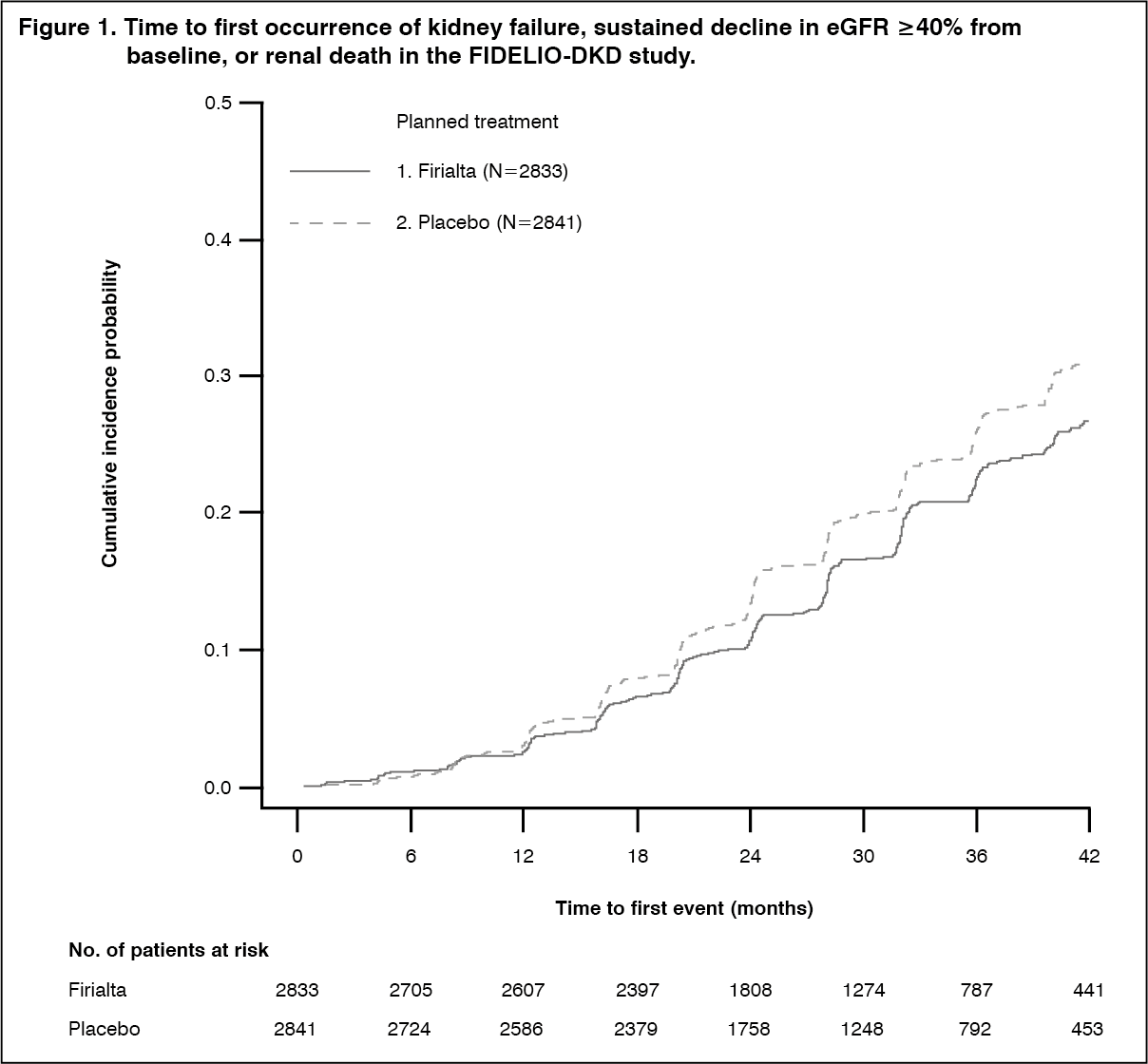 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image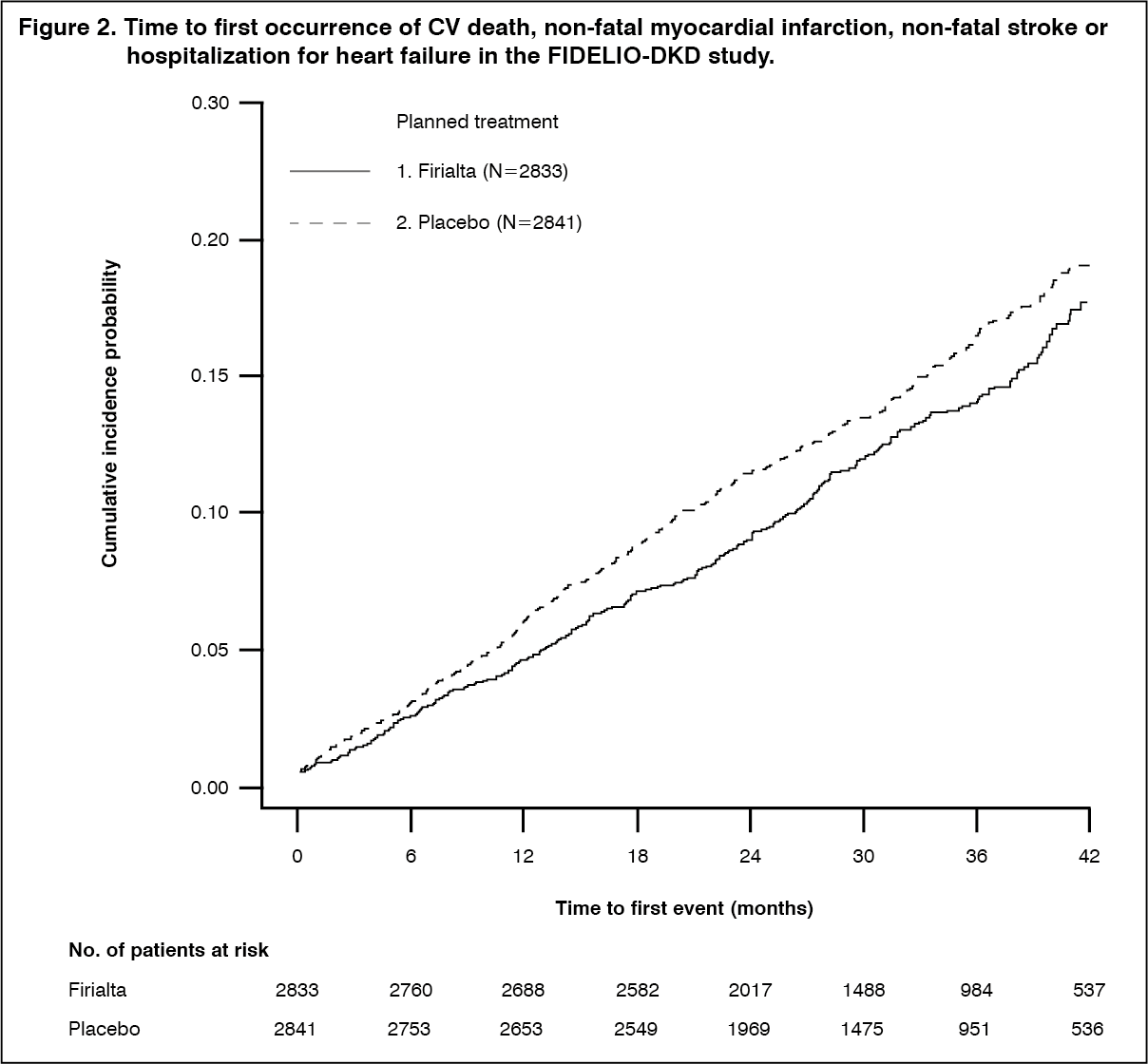 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image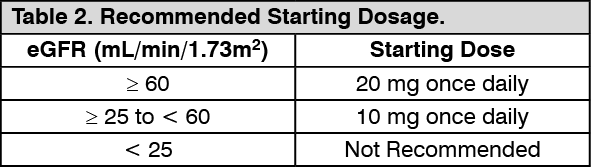 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image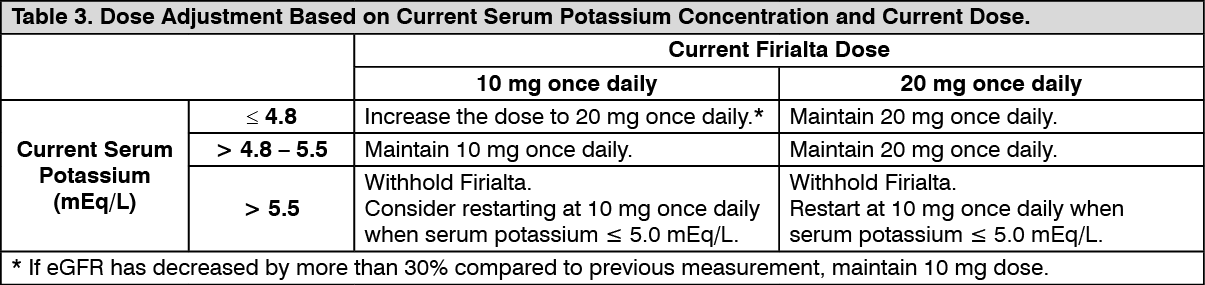 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out