PI: Intravenous: The most common adverse reactions observed at a rate ≥5% in subjects with intravenous treatment in the clinical trials were headache, cough, injection site reaction, nausea, pharyngitis and urticaria.
PI: Subcutaneous: The most common adverse reactions observed at a rate ≥5% of subjects with subcutaneous treatment in the clinical trials were infusion site reactions, headache, fatigue, arthralgia and pyrexia.
ITP: The most common adverse reactions observed at a rate ≥5% in subjects in the clinical trials were headache, vomiting, fever, nausea, back pain and rash.
CIDP: The most common adverse reactions observed at a rate ≥5% in subjects in the clinical trial were headache, fever, chills, hypertension, rash, nausea and asthenia.
Clinical Trials Experience: Because clinical studies are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of one drug cannot be directly compared to rates in other clinical trials of another drug and may not reflect the rates observed in clinical practice.
PI: Intravenous Administration: The most serious adverse event observed in clinical study subjects receiving GAMUNEX-C IV for PI was an exacerbation of autoimmune pure red cell aplasia in one subject.
In four different clinical trials to study PI, out of 157 subjects treated with GAMUNEX-C, 4 subjects discontinued due to the following adverse events: Coombs negative hypochromic anemia, autoimmune pure red cell aplasia, arthralgia/hyperhidrosis/fatigue/myalgia/nausea and migraine.
In a study of 87 subjects, 9 subjects in each treatment group were pretreated with non-steroidal medication prior to infusion, such as diphenhydramine and acetaminophen.
Table 14 lists all adverse events occurring in greater than 10% of subjects irrespective of the causality assessment. (See Table 14.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Table 15 lists the adverse reactions reported by at least 5% of subjects during the 9-month treatment. (See Table 15.)
Click on icon to see table/diagram/image
Table 16 lists the frequency of adverse reactions, which were reported by at least 5% of subjects, and their relationship to infusions administered. (See Table 16.)
Click on icon to see table/diagram/image
The mean number of adverse reactions per infusion that occurred during or on the same day as an infusion was 0.21 in both the GAMUNEX-C and GAMIMUNE N, 10% [Immune Globulin Intravenous (Human), 10%] treatment groups.
In all three trials in primary humoral immunodeficiencies, the maximum infusion rate was 0.08 mL/kg/min (8 mg/kg/min). The infusion rate was reduced for 11 of 222 exposed subjects (7 GAMUNEX-C, 4 GAMIMUNE N, 10%) at 17 occasions. In most instances, mild to moderate hives/urticaria, itching, pain or reaction at infusion site, anxiety or headache was the main reason. There was one case of severe chills. There were no anaphylactic or anaphylactoid reactions to GAMUNEX-C or GAMIMUNE N, 10% in clinical trials.
In the IV efficacy and safety study, serum samples were drawn to monitor the viral safety at baseline and one week after the first infusion (for parvovirus B19), eight weeks after first and fifth infusion, and 16 weeks after the first and fifth infusion of IGIV (for hepatitis C) and at any time of premature discontinuation of the study. Viral markers of hepatitis C, hepatitis B, HIV-1, and parvovirus B19 were monitored by nucleic acid testing (NAT, Polymerase Chain Reaction (PCR)), and serological testing.
PI: Subcutaneous Administration (PK and Safety Study): Adverse experiences were divided into 2 types: Local infusion site reactions, and Non-infusion site adverse events. Table 17 lists those adverse events occurring in ≥ 2% of infusions during the SC phase of the study. (See Table 17.)
Click on icon to see table/diagram/image
Table 18 lists the adverse reactions occurring in ≥5% of subjects and the frequency of adverse reactions per infusion. All local infusion site reactions were
a priori considered drug-related. (See Table 18.)
Click on icon to see table/diagram/image
There were no serious bacterial infections in the SC phase of the PK and safety study.
Local Infusion Site Reactions: Local infusion site reactions with SC GAMUNEX-C consisted of erythema, pain and swelling. The majority of local infusion site reactions resolved within 3 days. The number of subjects experiencing an infusion site reaction and the number of infusion site reactions decreased over time as subjects received continued weekly SC infusions. At the beginning of 570 the SC phase (week 1), a rate of approximately 1 infusion site reaction per infusion was 571 reported, whereas at the end of the study (week 24) this rate was reduced to 0.5 infusion site 572 reactions per infusion, a reduction of 50%.
ITP: In two different clinical trials to study ITP, out of 76 subjects treated with GAMUNEX-C, 2 subjects discontinued due to the following adverse events: Hives and Headache/Fever/Vomiting.
One subject, a 10-year-old boy, died suddenly from myocarditis 50 days after his second 578 infusion of GAMUNEX-C. The death was judged to be unrelated to GAMUNEX-C.
No pre-medication with corticosteroids was permitted by the protocol. Twelve ITP subjects treated in each treatment group were pretreated with medication prior to infusion. Generally, diphenhydramine and/or acetaminophen were used. More than 90% of the observed drug related adverse events were of mild to moderate severity and of transient nature. The infusion rate was reduced for 4 of the 97 exposed subjects (1 GAMUNEX-C [Immune Globulin Injection (Human), 10% Caprylate/Chromatography Purified], 3 GAMIMUNE N, 10% [Immune Globulin Intravenous (Human), 10%]) on 4 occasions. Mild to moderate headache, nausea, and fever were the reported reasons.
Table 19 lists any adverse events, irrespective of the causality, reported by at least 5% of subjects during the 3-month efficacy and safety study. (See Table 19.)
Click on icon to see table/diagram/image
Table 20 lists the adverse reactions reported by at least 5% of subjects during the 3-month efficacy and safety study. (See Table 20.)
Click on icon to see table/diagram/image
Serum samples were drawn to monitor the viral safety of the ITP subjects at baseline, nine days after the first infusion (for parvovirus B19), and 3 months after the first infusion of GIV and at any time of premature discontinuation of the study. Viral markers of hepatitis C, hepatitis B, HIV-1, and parvovirus B19 were monitored by nucleic acid testing (NAT, PCR), and serological testing. There were no treatment related emergent findings of viral transmission for either GAMUNEX-C or GAMIMUNE N, 10%.
CIDP: In the CIDP efficacy and safety study, 113 subjects were exposed to GAMUNEX-C and 95 were exposed to Placebo. (See Pharmacology: Pharmacodynamics: Clinical Studies under Actions). As a result of the study design, the drug exposure with GAMUNEX-C was almost twice that of Placebo, with 1096 GAMUNEX-C infusions versus 575 Placebo infusions. Therefore, adverse reactions are reported per infusion (represented as frequency) to correct for differences in drug exposure between the 2 groups. The majority of loading-doses were administered over 2 days. The majority of maintenance-doses were administered over 1 day. Infusions were administered in the mean over 2.7 hours.
Table 21 shows the numbers of subjects per treatment group in the CIDP clinical trial, and the reason for discontinuation due to adverse events. (See Table 21.)
Click on icon to see table/diagram/image
Table 22 shows adverse events reported by at least 5% of subjects in any treatment group irrespective of causality. (See Table 22.)
Click on icon to see table/diagram/image
The most common adverse reactions with Gamunex-C were headache and pyrexia. Table 22 lists adverse reactions reported by at least 5% of subjects in any treatment group. (See Table 23.)
Click on icon to see table/diagram/image
The most serious adverse reaction observed in clinical study subjects receiving GAMUNEX-C for CIDP was pulmonary embolism (PE) in one subject with a history of PE.
Laboratory Abnormalities: During the course of the clinical program, ALT and AST elevations were identified in some subjects.
For ALT, in the IV PI study treatment emergent elevations above the upper limit of normal were transient and observed among 14/80 (18%) of subjects in the GAMUNEX-C group versus 5/88 (6%) of subjects in the GAMIMUNE N, 10% group (p = 0.026).
In the SC PI study treatment emergent laboratory abnormalities during the SC phase occurred in several subjects. Four subjects (4/32, 13%) had elevated Alkaline Phosphatase and one subject (1/32, 3%) had a low Alkaline Phosphatase. One subject (1/32, 3%) had an elevated ALT and three subjects (3/32, 9%) had an elevated AST. No elevations were >1.6 times the upper limit of normal.
In the ITP study which employed a higher dose per infusion, but a maximum of only two infusions, the reverse finding was observed among 3/44 (7%) of subjects in the GAMUNEX-C group versus 8/43 (19%) of subjects in the GAMIMUNE N, 10% group (p = 0.118).
In the CIDP study, 15/113 (13%) of subjects in the GAMUNEX-C group and 7/95 (7%) in the Placebo group (p=0.168) had a treatment emergent transient elevation of ALT.
Elevations of ALT and AST were generally mild (<3 times upper limit of normal), transient, and were not associated with obvious symptoms of liver dysfunction.
GAMUNEX-C may contain low levels of anti-Blood Group A and B antibodies primarily of the IgG
4 class. Direct antiglobulin tests (DAT or direct Coombs tests), which are carried out in some centers as a safety check prior to red blood cell transfusions, may become positive temporarily. Hemolytic events not associated with positive DAT findings were observed in clinical trials.
Postmarketing Experience: Because adverse reactions are voluntary and reported post-approval from a population of uncertain size, it is not always possible to reliably estimate their frequencies or establish a causal relationship to product exposure.
GAMUNEX-C Postmarketing Experience: The following adverse reactions have been identified and reported during the post marketing use of GAMUNEX-C:
Hematologic: Hemolytic anemia.
Infections and Infestations: Aseptic meningitis.
The following adverse reactions have been identified and reported during the overall post marketing use of IGIV products:
Respiratory: Apnea, Acute Respiratory Distress Syndrome (ARDS), TRALI, cyanosis, hypoxemia, pulmonary edema, dyspnea, bronchospasm.
Cardiovascular: Cardiac arrest, thromboembolism, vascular collapse, hypotension.
Neurological: Coma, loss of consciousness, seizures/convulsions, tremor.
Integumentary: Stevens-Johnson syndrome, epidermolysis, erythema multiforme, bullous dermatitis.
Hematologic: Pancytopenia, leukopenia, hemolysis, positive direct antiglobulin (Coombs test).
General/Body as a Whole: Pyrexia, rigors.
Musculoskeletal: Back pain.
Gastrointestinal: Hepatic dysfunction, abdominal pain


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image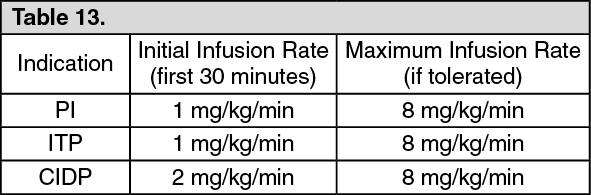 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image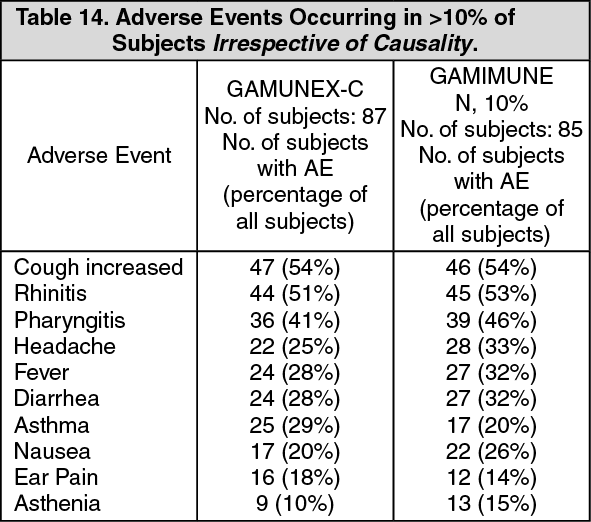 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image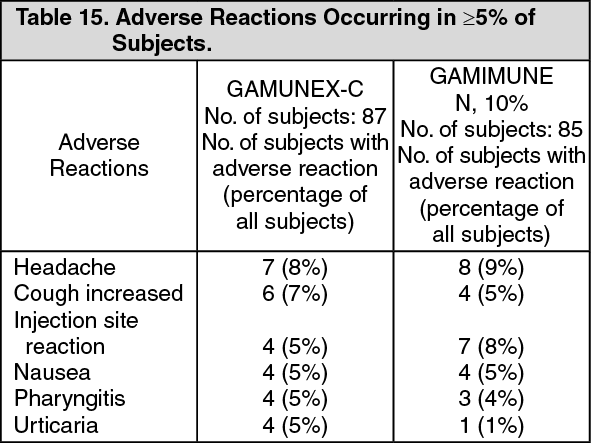 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image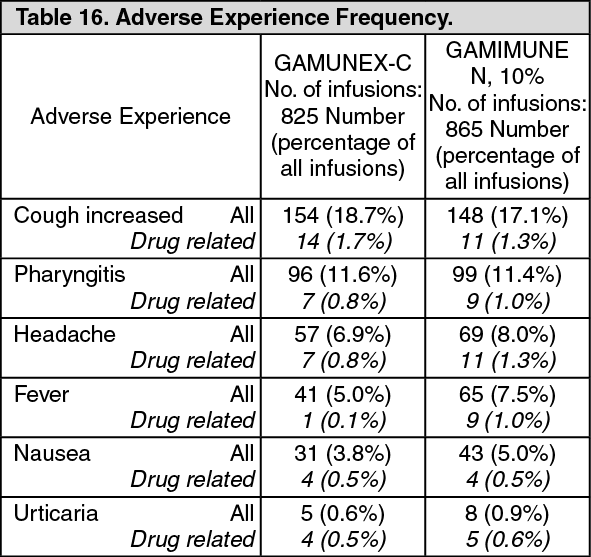 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image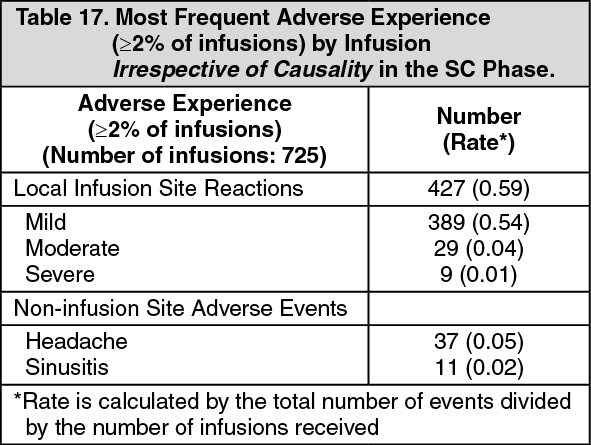 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image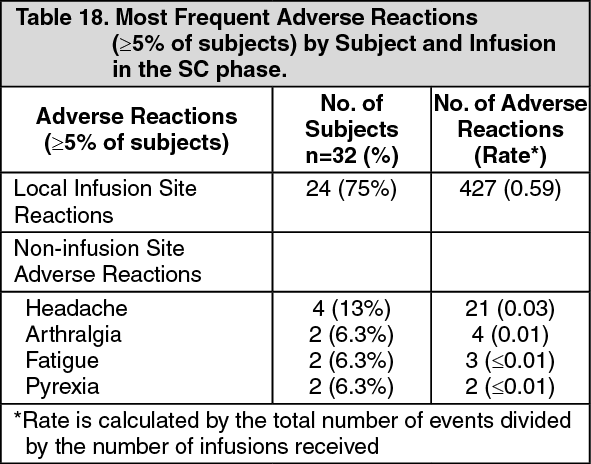 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image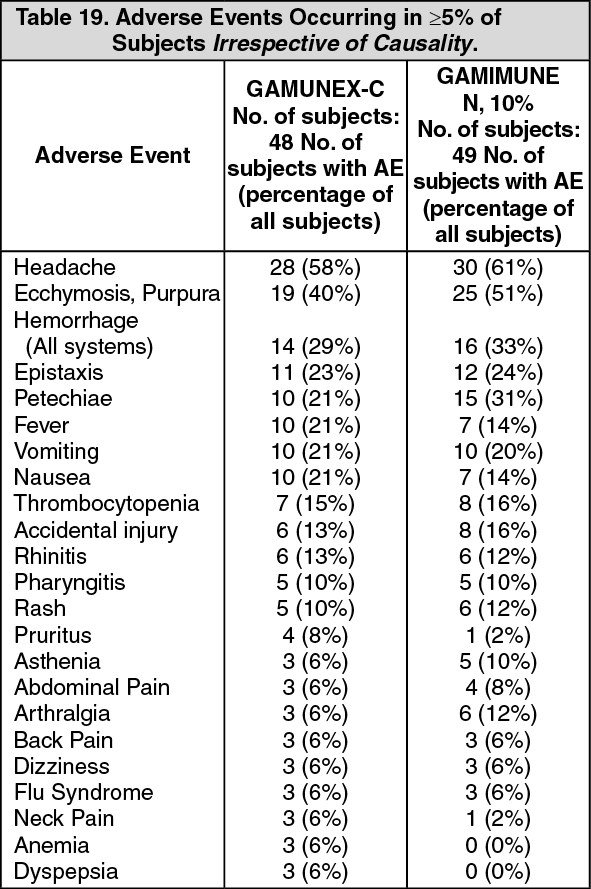 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image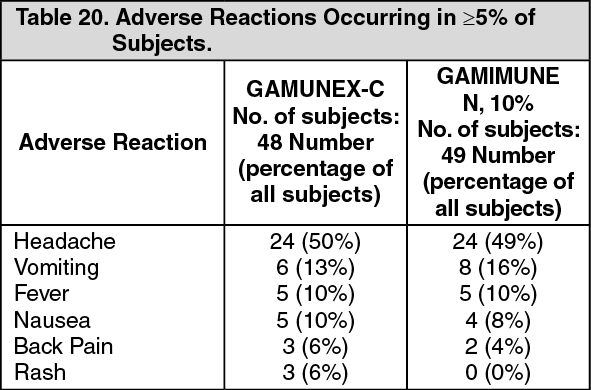 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image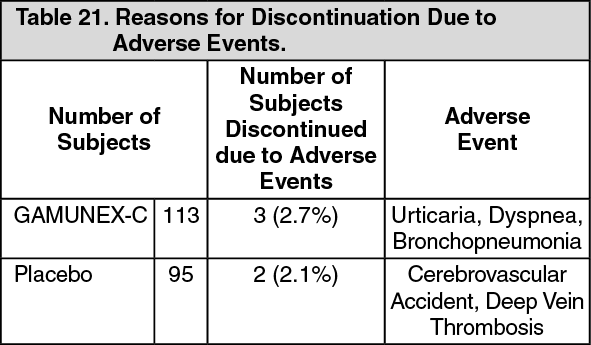 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image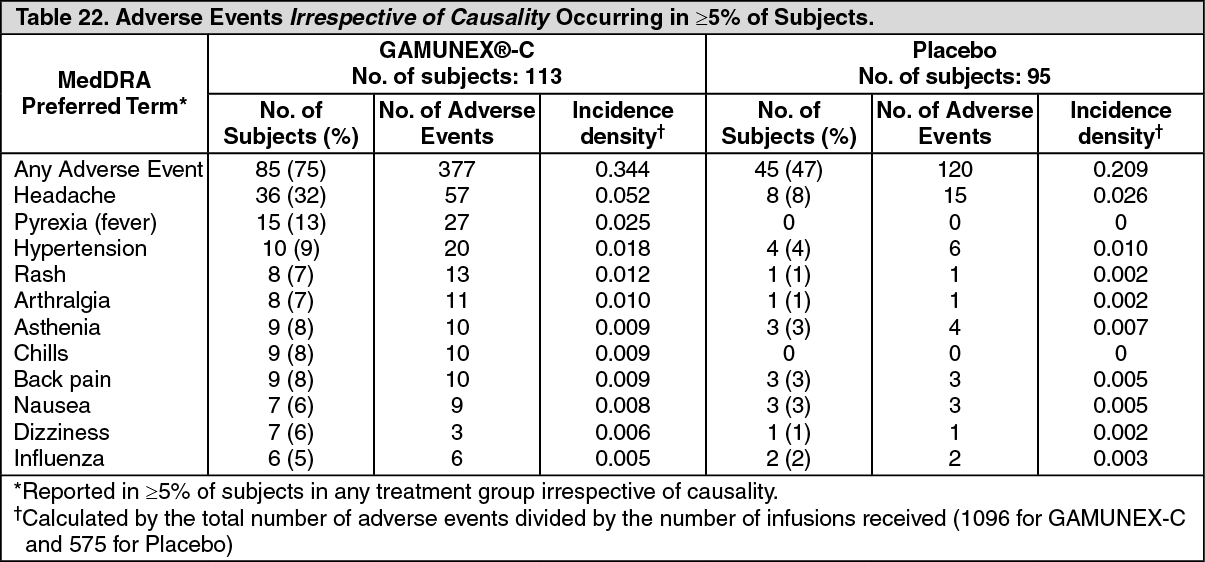 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image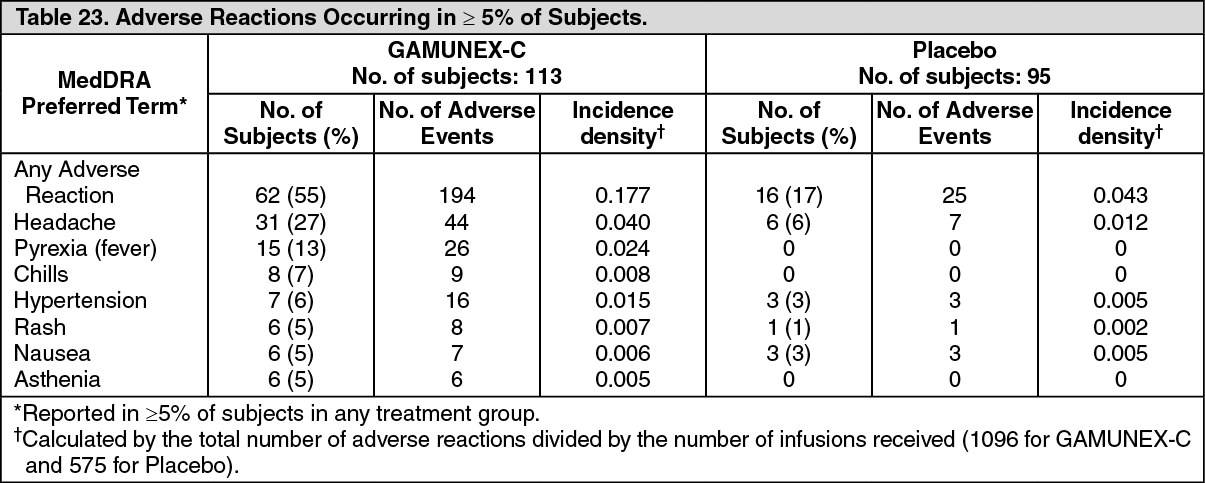 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out