Take the tablet at about the same time each day, with some liquid if necessary. Follow the direction of the arrows until all 21 tablets have been taken. During the next 7 days take no tablets. A period should begin during these 7 days (the withdrawal bleed). Usually it will start on day 2-3 after the last tablet. Start taking the next pack on the 8
th day (the day after the 7-day tablet-free break) even if the period continues. This means that new packs will always start on the same day of the week, and withdrawal bleed will occur on about the same days, each month.
Start with the first pack: Start taking Gveza on the first day of the cycle (that is, the first day of period). Take a tablet marked with that day of the week. For example, if period starts on a Friday, take a tablet marked Friday. Then follow the days in order. Gveza will work immediately, it is not necessary to use an additional contraceptive method.
Missed dose: Depending on the day of the cycle on which one tablet has been missed, patient may need to take additional contraceptive precautions, for example a barrier method such as a condom. Take the tablets according to the following principles: If less than 12 hours late when taking a tablet, the protection against pregnancy is not reduced. Take the tablet as soon as remembered and then continue taking the tablets again at the usual time.
If more than 12 hours late in taking a tablet, protection against pregnancy may be reduced. The more tablets forgotten, the greater the risk that the protection from pregnancy is reduced. There is a particularly high risk of becoming pregnant if tablets are missed at the beginning of the pack or at the end (the last of the 21 tablets). Therefore, follow the rules given as follows.
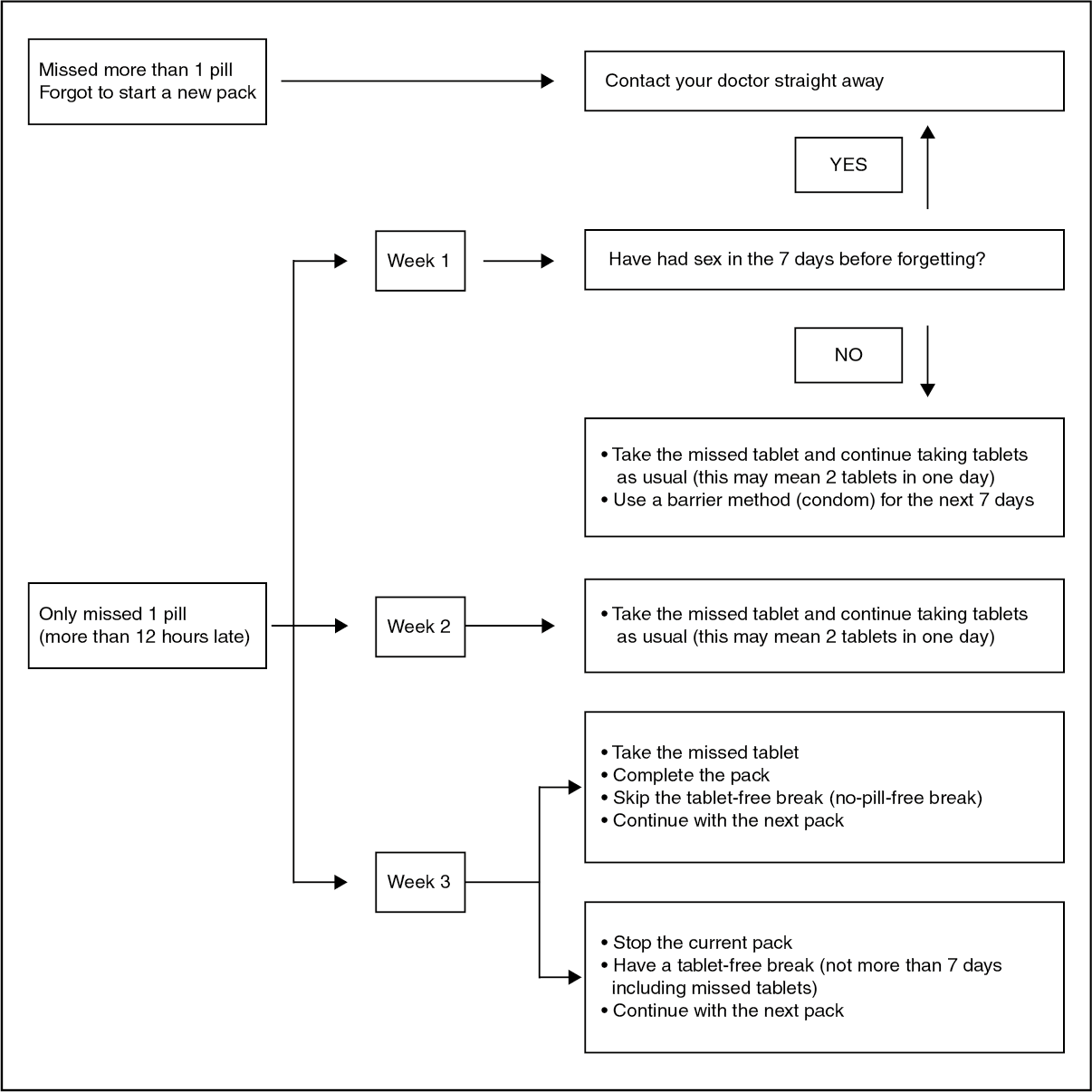
More than one tablet forgotten in a pack: Contact a doctor.
Do not take more than 2 tablets on a given day, to make up for missed pills.
If tablets are forgotten in a pack, and there is no expected bleeding that should start in the normal tablet free break, pregnancy is a possibility. Contact a doctor before starting the next pack.
1 tablet missed during week 1: If patient has forgotten to start a new pack, or have missed tablet(s) during the first 7 days of the pack, there is a risk of being pregnant (if they had sex in the 7 days before forgetting the tablet). In that case contact a doctor before starting the next pack. See also the "missed pill chart" for details.
If patient has had no sex in the 7 days before the oversight, take the missed tablet as soon as remembered (even if this means taking two tablets at the same time) and take the next tablets at the usual time. Use extra contraceptive precautions (barrier method) for the next 7 days.
1 tablet missed during week 2: Take the missed tablet as soon as remembered (even if this means taking two tablets at the same time) and take the next tablets at the usual time. The reliability of the pill is maintained. There is no need to use extra contraceptive precautions.
1 tablet missed during week 3: Choose either of the following options, without the need for extra contraceptive precautions.
1. Take the missed tablet as soon as remembered (even if this means taking two tablets at the same time) and take the next tablets at the usual time. Start the next pack as soon as the current pack is finished so that no gap is left between packs. A withdrawal bleed may not occur until the end of the second pack but may have spotting or breakthrough bleeding while taking the tablets. Or
2. Stop taking tablets from the current pack, have a tablet-free break of 7 days or less (also count the day a tablet is missed) and continue with the next pack. (See Figure.)
 Click on icon to see table/diagram/image
Dosage adjustment in hepatic impairment:
Click on icon to see table/diagram/image
Dosage adjustment in hepatic impairment: Contraindicated in patients with hepatic dysfunction.
Dosage adjustment in renal impairment: I.V.:
Note: Contraindicated in patients with renal dysfunction.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image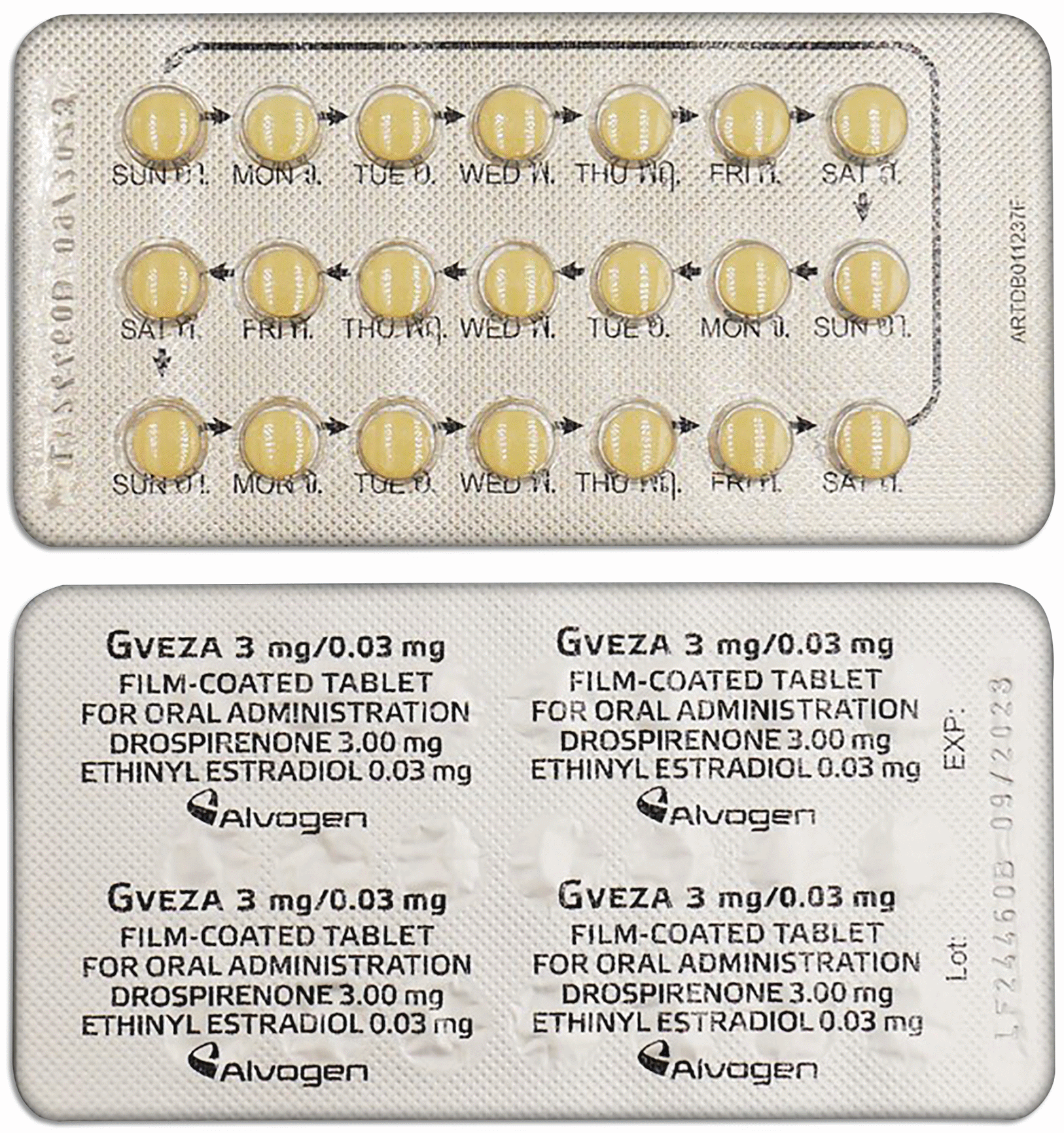

 Sign Out
Sign Out
