


 Sign Out
Sign Out

Myelosuppression: Different degrees of myelosuppression (leucocytopenia, thrombocytopenia and anemia) can occur, depending on the dose. Frequently, leucocytopenia with the risk of life-threatening infections and thrombocytopenia with the risk of bleeding have to be taken into consideration. The lowest leucocyte and thrombocyte counts normally occur 1-2 weeks after start of treatment and recover within 3-4 weeks. Anemia usually occurs after several cycles of treatment. A combination treatment with other myelosuppressive agents may require dose adjustments. Single high-dose treatment leads more frequently to leucocytopenia than fractionated dose-regimen. In pre-treated (chemotherapy and/or radiotherapy) patients or patients with renal function impairment, a more severe myelosuppression can be expected. With ifosfamide as with other cytostatics, blood counts have to be taken before each chemotherapy cycle as well as during the intervals between cycles. Depending on the blood picture, appropriate dose adaptations (see table) should be made.
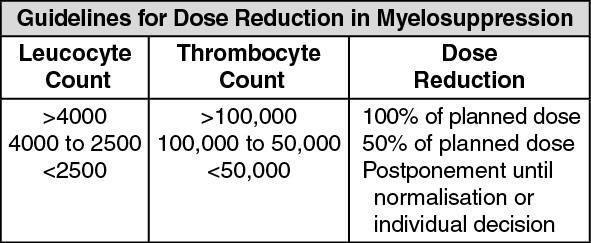 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageUrotoxicity and Nephrotoxicity: Hemorrhagic cystitis (macro- and microhematuria) is a frequent, dose-dependent complication of ifosfamide.
Note: Fractionated dosing, adequate hydration, maintenance of fluid balance and particularly concomitant treatment with Uromitexan (mesna) can markedly reduce the frequency and severity of hemorrhagic cystitis.
Disorders of glomerular renal function with an increase in serum creatinine, a decrease in creatinine clearance and proteinuria can occasionally occur, or more frequently, disorders of tubular renal function with hyperaminoaciduria, phosphaturia, acidosis or proteinuria. Severe nephropathies are rare. Possible risk factors for disorders of glomerular renal function are high doses of Holoxan and additional treatment with platinum-containing drugs. Risk factors for disorders of tubular renal function are previous nephrectomy, additional treatment with platinum-containing drugs or concomitant irradiation of the abdomen with inclusion of the kidneys or the remaining kidney. Caution is advisable when potentially nephrotoxic drugs eg, aminoglycosides, acyclovir or amphotericin B are used concomitantly. These drugs do not potentiate the tubular kidney disorder, but may cause further deterioration of glomerular function.
In rare cases, patients with chronic tubular kidney disorder may develop Fanconi's syndrome resulting in rickets or, in adults, osteomalacia. Predisposing factors are high cumulative doses of the drug and young age (particularly <3 years). Glomerular and tubular kidney function must therefore be evaluated and checked before start of therapy, during and after therapy.
During long-term treatment with ifosfamide, sufficient diuresis and regular monitoring of renal function is necessary. This applies especially to children. In case of beginning nephropathy, irreversible kidney damage has to be expected if treatment with ifosfamide is continued. A careful risk-benefit evaluation is required.
Caution is required in unilaterally nephrectomized patients, in patients with impaired renal function and in patients pre-treated with nephrotoxic drugs (eg, cisplatin). In these patients, frequency and intensity of myelotoxicity, nephro- and cerebral toxicity are increased.
Central Nervous System: In 10-20% of cases, encephalopathy occurs and develops within a few hours up to a few days after start of treatment. Risk factors are a poor state of health, impaired renal function (creatinine >1.5 mg/dL), pre-treatment with nephrotoxic drugs (eg, cisplatin) and postrenal obstructions (eg, pelvic tumours). Other possible risk factors are old age, a history of alcohol abuse, decreased levels of serum albumin or hydrogen carbonate, hepatic dysfunction or concurrent high-dose treatment with antiemetic drugs. The most common symptom of encephalopathy is drowsiness which can progress to somnolence and coma. Other symptoms can be weakness, forgetfulness, depressive psychoses, disorientation, restlessness, confusion, hallucinations, cerebellar symptoms, incontinence and convulsions. The encephalopathies are usually reversible and disappear spontaneously within a few days after the last ifosfamide administration. Severe courses are rare, and deaths were only seen in isolated cases and in connection with very high doses of Holoxan. With a fractionated dose regimen, encephalopathies are less frequent and less severe.
Note: Due to the CNS toxicity of ifosfamide, patients must be carefully monitored. In the event of encephalopathy, ifosfamide treatment has to be discontinued and must not be resumed. In case of ifosfamide-induced encephalopathy, drugs acting on the CNS (eg, antiemetics, tranquilizers, narcotics or antihistamines) should be discontinued if possible, or used with special caution.
Other Side Effects: Nausea and vomiting are dose-dependent side effects. Moderate to severe forms can be seen in about 50% of the cases. Another frequent side effect is reversible alopecia which occurs in up to 100% of patients, depending on dosage and duration of treatment. Because of its alkylating mechanism of action, Holoxan can cause partly irreversible impairment of spermatogenesis with resulting azoospermia or persistent oligospermia. Less frequently irreversible ovulation disturbances with resulting amenorrhea and reduced levels of female sex hormones.
Additionally, there can occur, in isolated cases, chronic interstitial pulmonary fibrosis. Toxic-allergic pulmonary edema was reported in a single case.
In isolated cases, SIADH (syndrome of inadequate ADH secretion, Scwartz-Bartter syndrome) with hyponatremia and water retention. Hypokalemia was reported in a single case.
In rare cases, inflammation of the skin and mucous membrane.
In rare cases, hypersensitivity reactions, in isolated cases, progressing to shock.
In rare cases, blurred vision and episodes of dizziness.
An increase in liver enzymes and/or in the bilirubin level can also occur occasionally. Anorexia, diarrhea, constipation, phlebitis or pyrexia may more seldom be seen. Polyneuropathy, pneumonitis, impaired vision or an increased reaction to radiation were seen in isolated cases. There have been isolated reports of supraventricular or ventricular arrhythmias, ST-segment changes and heart failure after very high doses of ifosfamide and/or after pre-treatment or concomitant treatment with anthracyclines. In this context, it is again necessary to stress the need for regular electrolyte monitoring and special caution when treating patients with a history of heart disease. As with cytotoxic therapy in general, especially with alkylating agents, treatment with ifosfamide involves the risk of secondary tumours as a late sequelae.