Gastrointestinal Reactions: Nausea, diarrhea, vomiting, staining of teeth and/or tongue. In common with virtually all other broad spectrum antibiotics, pseudomembranous colitis has been reported.
Hematological Effects: Eosinophilia, leukopenia, neutropenia, including agranulocytosis, thrombocytopenia, thrombocytosis, and decreased hemoglobin, pancytopenia and prolonged prothrombin time have been reported. A positive direct Coomb's test may develop in some individuals.
Nervous System/Psychiatric: As with other beta-lactam antibiotics, CNS side effects such as myoclonic activity, psychic disturbances, including hallucination, confusional states, or seizures have been reported, paresthesia, encephalopathy.
Allergic Reactions/Skin: Rash, pruritus, urticaria, erythema multiforme, Stevens-Johnson syndrome, angioedema, toxic epidermal necrolysis (rarely), exfoliative dermatitis (rarely), candidiasis, fever including drug fever, anaphylactic reactions.
Renal Function: Oliguria/anuria, polyuria, acute renal failure (rarely). The role of imipenem/cilastatin sodium in changes in renal function is difficult to assess, since factors predisposing to pre-renal azotemia or to impaired renal function usually have been present. Elevations in serum creatinine and blood urea nitrogen have been observed. Urine discoloration. This is harmless and should not be confused with hematuria.
Local Reaction: Erythema, local pain and induration, phlebitis and/or thrombophlebitis.
Liver Function: Increases in serum transaminases, bilirubin and/or serum alkaline phosphatase; hepatic failure (rarely), hepatitis (rarely) and fulminant hepatitis (very rarely).
Other: Hypotension.


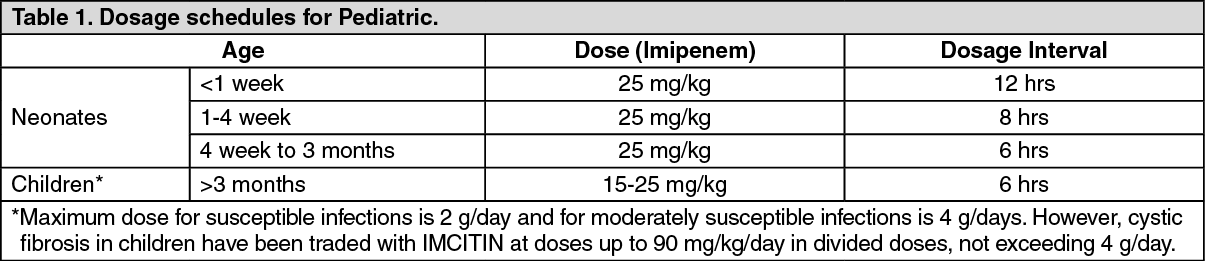 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image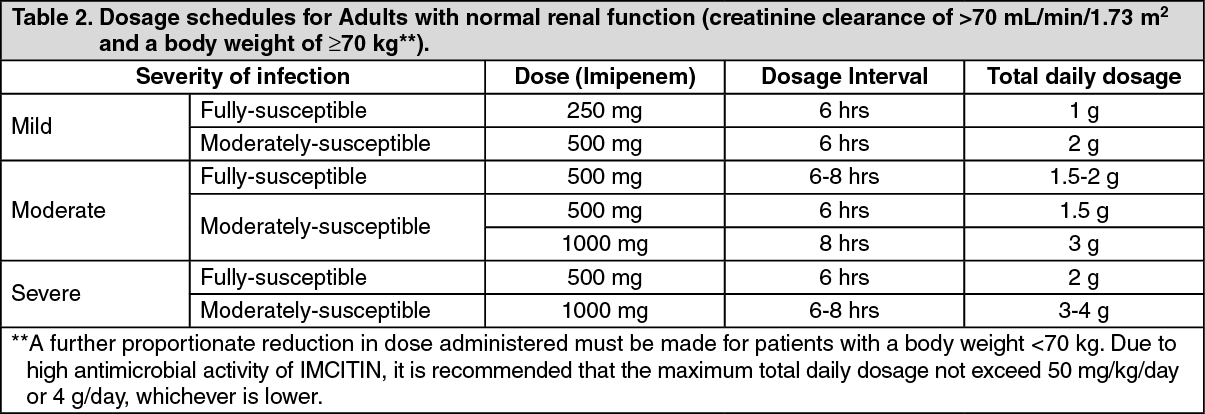 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image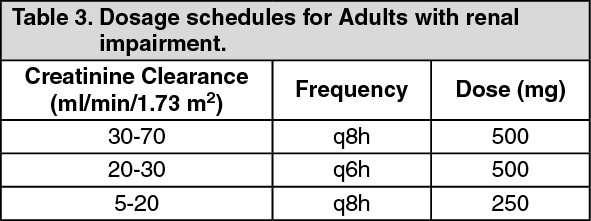 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image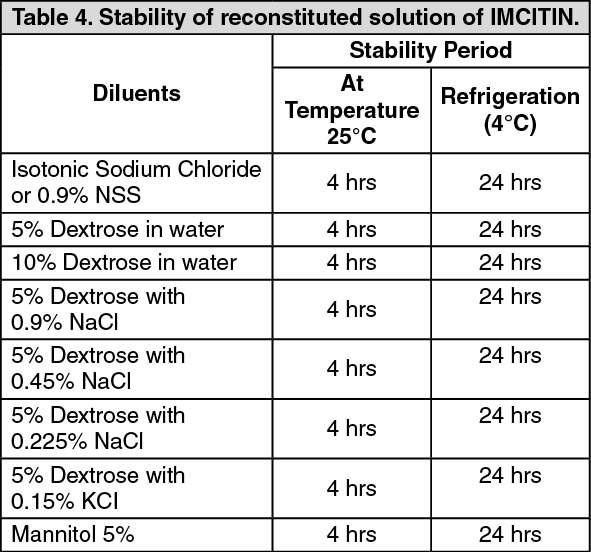 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out